
Abstract
Background
Pharmacological treatment of cluster headache constitutes the core of clinical management, but evidence is sparse. We aimed to generate insight in the existing treatment and identify associations between clinical features and treatment response.
Methods
Patients aged 18–65 diagnosed with cluster headache according to the ICHD-2 completed a questionnaire followed by a structured interview. Multiple logistic regression was used to identify associations.
Results
The population consisted of 400 patients with an episodic: chronic ratio of 1.7:1. Episodic patients were more likely to respond to triptans (odds ratio = 1.77, confidence interval: 1.08–2.91, p = 0.023) and oxygen (odds ratio = 1.64, confidence interval: 1.05–2.57, p = 0.031) than chronic. Oxygen response was less likely if pain intensity was very severe (odds ratio = 0.53, confidence interval: 0.33–2.57, p = 0.006) and the risk of a poor response increased with disease duration (odds ratio = 0.79, confidence interval: 0.65–0.96, p = 0.016). Among current users of sumatriptan injection and oxygen, the proportion achieving 100% relief was higher with sumatriptan injection (p > 0.001) than with oxygen. No associations were identified regarding verapamil. Only 57% of current users of preventive medication responded at a 50% level.
Conclusion
Episodic cluster headache is more responsive to acute therapy than chronic. Further, sumatriptan injection was more effective than oxygen and the responder-rate was limited with verapamil. More effective acute and preventive therapies are needed for cluster headache patients.
Introduction
Cluster headache (CH) is a severely disabling primary headache disorder and pharmacological treatment constitutes the core of clinical management (1). The first line of acute treatment is sumatriptan administered subcutaneously (henceforth referred to as sumatriptan injection) (2) and inhalation of 100% oxygen (3). Transitional treatment is often used to relieve the patient until maintenance prophylactic is adequately titrated. Transitional treatment consists of oral steroids or greater occipital nerve (GON) blocks (4). Preventive treatment aims to reduce attack frequency with verapamil being the first choice, but only 50–80% of CH patients are responders (5) and its use is hampered by side effects as many patients need very high doses. Due to the narrow therapeutic window, the side effects and the evidence level, lithium is less attractive and remains a second line of treatment (6). Other preventive agents, for example topiramate, can be used but evidence is also very sparse (6). In the clinic, various types of treatment are combined in the efforts to provide relief to the patients and increase quality of life.
Current knowledge does not allow physicians to personalize therapy and hence the strategy at present is trial and error. If clinical characteristics could predict positive treatment outcome this would greatly assist headache clinicians in targeting efforts, ultimately decreasing the personal burden of CH (7). We aimed to generate knowledge of the existing treatment of CH and, if possible, identify associations between clinical features and treatment response.
Methods
The study is a cross-sectional investigation (performed 2012–2017) based on data from the Danish Cluster Headache Survey. We applied the same methodology as in previous studies (8–13) and the primary analysis of the dataset has previously been published (8).
Patients
In total, 400 patients (aged 18–65 years) participated in the study (Figure 1). Included patients were diagnosed with episodic CH (eCH) or chronic CH (cCH) according to the International Classification of Headache Disorders (ICHD), second edition (14). Patients were recruited primarily from the Danish Headache Center, a tertiary headache center, and a few were recruited from private practitioners and from an online advertisement (www.forsogsperson.dk). A headache specialist at the Danish Headache Center validated all diagnoses. The aim of the original sleep investigation required a population of 109 patients but to ensure future investigations, 400 patients were included.

Title: Flow chart for participation in the questionnaire study Figure legend: Not needed.
Patient consent, protocol approvals and registration
All patients gave informed written consent according to the Helsinki declaration and the Capital Region of Denmark Ethical Committee approved the study (H-2-2012-016) as part of a sleep study (15). After this study was completed the survey did not need approval according to the ethics committee (file-number: 17008910).
Questionnaire
The survey consisted of 362 questions, including already-validated sections (Pittsburgh Sleep Quality Index (PSQI), Epworth Sleepiness Scale (ESS)), and specific CH questions developed by authors (MB, RJ). The ESS is a seven-item scale that evaluates the likelihood of falling asleep (16). The PSQI is a self-rated questionnaire that evaluates sleep quality (17). The patients filled out the questionnaire and afterwards underwent a semi-structured interview by a physician or trained medical student or study nurse (MB, NL, AP, MF) to rule out ambiguities. Missing data were only allowed for dosages of previous medication and are indicated in parentheses in the article.
Regarding treatment, patients were asked to fill out current and previous acute medications in sections: Oxygen, triptans, ergotamines and “other”. For each current treatment category, they filled out the percentage of attacks treated with the given therapy. Effect was only rated for current treatments. Patients were asked to rate effect in four categories (“Completely, the pain is gone”; “Some, the pain is halved or more”; “A little, it only takes the top off the pain”; “None, the pain is unchanged”). For acute therapies, we defined a 50% responder as a patient who reported “completely, the pain is gone” or “some, the pain is halved or more”. An acute 100% responder was defined as having answered “completely, the pain is gone”. For preventive treatment, the prespecified categories were verapamil, lithium, methysergide, prednisolone and other. The effect was rated in four categories (“completely, the attacks are gone”; “some, the attacks are halved in frequency or intensity”; “a little, the attacks are fewer or milder”; “none, the attacks are unchanged”). A 50% responder to a prophylactic medication was defined as having answered “completely, the attacks are no longer present” or “some, the attacks are halved in frequency or intensity”. A preventive 100% responder was defined as having answered “completely, the attacks are gone”. Pain intensity was rated on a five-point rating scale (none, mild, moderate, severe or very severe) and to increase the statistical power, mild, moderate and severe were grouped as one group called moderate. Patients in bout were defined as having an attack within the last month. Verapamil was divided into high and low dose, respectively defined as doses above or equal to 500 mg and lower than 500 mg. Medically refractory was defined, according to the consensus statement of the European Headache Federation (EHF) (18), as a cCH-patient diagnosed according to current criteria with at least three severe attacks per week and three failed prophylactic agents, (transitional medications not included).
Statistics
We used multiple logistic regression to calculate odd ratios (ORs) of association. A favorable outcome was defined as either a 50% response or 100% response. The pre-specified factors were sex, phenotype (eCH or cCH), years with CH (per decade), pain intensity (very severe and moderate), and specific factors previously linked to effect in the literature (19). Backward selection was used for model building. Model control of final models was done with the plots function. Binary variables were tested for interactions. Linearity assumption was tested for continuous variables and if an assumption violation was identified we used a 10-logarithm transformation. The comparison between oxygen and sumatriptan injection was done by chi-squared test. An independent two-group t-test was used to compare ESS and PSQI inside and outside bout. A p-value < 0.05 was considered significant. Most of the data is descriptive and reported as raw data, percentages and medians with interquartile range (IQR). We did not correct for multiple testing. R 3.4.1 (R Foundation for Statistical Computing, Vienna, Austria) and Rstudio 1.0.153 were used for all statistical analysis.
Data availability
The Danish Cluster Headache Survey contains sensitive information and can consequently not be shared in full form according to Danish data protection law. Deidentified data that underlie the results of this article can be shared on request.
Results
In total, 644 CH patients were invited, and 400 CH patients responded (62%) (Figure 1). The ratio between eCH and cCH was 1.7. The mean duration of CH was 14.9 years; however, the range varied from 0–54 years (Table 1). When completing the questionnaire, 271 patients were experiencing attacks (episodic in bout or chronic) leaving the remaining 129 eCH patients in remission.
Demographic factors and clinical characteristics for patients with cluster headache.

CH: cluster headache; eCH: episodic cluster headache; cCH: chronic cluster headache.
Acute treatment
Acute abortive treatment was used by 358/400 (90%) of the patients, of whom 165 patients (46%) used monotherapy (oxygen: 101, sumatriptan injection: 30, sumatriptan nasal spray: 8, oral triptan: 15, simple analgesics: 6, opioids: 4, SPG-stimulation: 1, psilocybin: 1). The most frequent combination was triptans (any type) and oxygen (n = 173, 45%), of whom 119 patients (30%) combined sumatriptan injection and oxygen. Acute medication shortened attacks by 65 min (72%) from a median of 90 min to 25 min.
Oxygen
In total, 353 out of 400 patients had used oxygen for CH, of whom 284/400 (71%) used it as a current acute treatment and 69 as a previous treatment (Figure 2). Thus, 47 patients were oxygen naïve. In the patients who listed oxygen as a current acute therapy, oxygen was used in a median of 95% (range: 1–100%) of the attacks. Complete response was achieved by 82/284 (29%) of users; however, 210/284 (74%) were 50% responders. Mean oxygen flowrate was 12.6 L/min. Among the 49 previous users, the median flowrate was 10.0 L/min (missing data in 20/69).

Title: Effect of first line therapies of Cluster headache Figure legend: Patient-reported effect of oxygen, sumatriptan injection and verapamil treatment of current users. Percentages are calculated as the exact number divided by the entire cohort (N = 400). Data presented for current users of oxygen, n = 284 patients. Data not presented of previous oxygen users (n = 69) and oxygen naïve patients (n = 47). Data presented for current users of sumatriptan injection, n = 138. Not shown data from current users of other triptans or patients using a triptan combination (n = 96), previous triptan users (n = 92, hereof 65 patients had used sumatriptan injection) and triptan naïve patients (n = 74). Data presented for current users of verapamil monotherapy, n = 193. Data not presented for current users of verapamil in combination with other preventatives (n = 28), previous verapamil users (n = 91) and verapamil naïve patients (n = 88).
In the logistic regression analysis, a favorable outcome of oxygen was associated with eCH, moderate pain intensity and few years with CH (Table 2). Sex, smoking (current and prior) and clinical features (restlessness and photophobia/phonophobia) was not associated with treatment outcome. Among patients who currently used oxygen, a higher chance of complete response was associated with eCH, male sex, moderate pain intensity, and fewer years with CH (Supplementary Table 1). Oxygen flowrate was not associated with complete response.
Logistic regression of oxygen response (50% level) and clinical features.

Note: Data is presented as odds ratios with confidence intervals and p-value. Oxygen naïve patients were excluded for the analysis (n = 47). For categorical variables, the reference is highlighted in italics. p-values highlighted in bold are significant (**p < 0.01 *p < 0.05).
eCH: episodic cluster headache; cCH: chronic cluster headache; OR: odds ratio; CI; 95% confidence interval.
Triptans
At the time of interview, 234 CH (59%) patients currently used triptans, and 92 CH patients marked triptan as previously used, leaving 74 (19%) patients as triptan naïve. The most frequently used administration form was injection (59%). In the injection group, 79/138 (57%) achieved pain freedom and 121/138 (88%) were 50% responders. Injectable sumatriptan was used in a median of 50% of attacks. Attack frequency was similar in the responder and non-responder group.
Nasal spray was used by 27/400 (7%) and 18/27 (67%) were 50% responders, of whom 10 (37%) were 100% responders. Oral triptans were used by 54/400 (14%), of whom 46/54 (85%) were 50% responders and 17 (32%) were 100% responders.
Two or three different forms of administration of triptans were used by 15/400 (4%) and all were 50% responders. In the combination group, triptans were used in a median of 90% of attacks. Overall, 10 CH patients (14%) in the triptan naïve group and 16 patients (17%) in the previous-triptan group reported contraindications (angina pectoris, cerebral or cardiac infarction).
A positive triptan response was associated with eCH (OR: 1.77, CI: 1.08–2.91, p = 0.023) in the logistic regression analysis. No association was found with sex, years with CH, attack duration or pain intensity (Table 3). Among the current users, we also found a positive association between eCH and 100% response (OR: 2.35, CI: 1.30–4.31, p = 0.005) (Supplementary Table 2). Sumatriptan injection was more likely to achieve 100% response compared to oral (OR: 0.36, CI: 0.18–0.71, p = 0.004) or nasal application (OR: 0.41, CI: 0.17– 0.97, P = 0.047). Sex was not significantly associated with a positive response.
Logistic regression of triptan response (50% level) and clinical features

Note: Data is presented as odds ratios with confidence intervals and p-value. Triptan naïve patients and previous triptans users with contraindications were excluded from the analysis (n = 90). For categorical variables the reference is highlight in italics. p-values highlighted in bold are significant (*p < 0.05).
eCH: episodic cluster headache; cCH: chronic cluster headache; OR: odds ratio; CI: 95% confidence interval.
Comparison of oxygen and sumatriptan injection
Currently, 119 CH patients used both sumatriptan injection and oxygen. In this group, the proportion of 100% responders and 50% responders were significantly higher with sumatriptan injection than oxygen (p > 0.001 and p = 0.022).
Other acute treatments
Simple analgesics were used by 19 patients (5%) while SPG stimulation and opioids were each used by eight patients (2%), respectively. However, at the time of the interview, the SPG stimulator had only been made available to very few patients; therefore, firm conclusions regarding this specific treatment cannot be made based on data presented here. Four of the eight SPG-patients were 50% responders and four of the opioid users were 50% responders. Simple analgesics were used as monotherapy in six patients (32%), and in combination with other acute treatments by 13 patients (68%). Two patients reported current use of ergotamine or levomepromazine. Promethazine, combination-treatment (benzodiazepine, ibuprofen and anti-emetics), psilocybin, cannabis, D-lysergic acid amide seeds and icebags were all used by one patient, respectively.
Preventive treatment
In total, 250 patients (63%) of the study population currently used preventive therapy. Of these, 218 (87%) used it as monotherapy, 28 (11%) used two concurrent preventive treatments and only four CH patients (2%) used three or more preventive therapies at the same time. Of the 400 CH patients, 76 (19%) patients had never received preventive treatment.
Verapamil
Verapamil was currently used by 220/400 (55%) patients, making it the most frequent preventive therapy. Currently, 77 (35%) patients used high dose verapamil (≥500 mg/day). ECH patients most frequently used low dose verapamil (<500 mg/day), whereas cCH patients used all other preventive therapies, including high dose verapamil, most frequently. Previous usage of verapamil was reported by 91 out of 400 patients (23%). A reduction of 50% or more was reported by 126/220 (57%) of current users and no differences regarding age, sex, and CH duration were observed between patients on low or high dose verapamil (Table 4). No associations between clinical phenotypes (eCH/cCH and sex) and effect were identified. Verapamil responders and non-responders were similar in relation to comorbidities and lifestyle factors, except for alcohol consumption, which was twice as high for responders compared to non-responders (Supplementary Table 3).
Verapamil use among cluster headache patients.
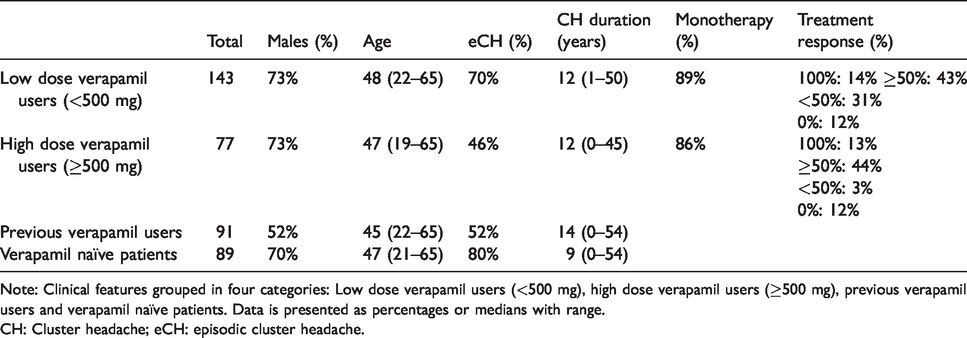
Note: Clinical features grouped in four categories: Low dose verapamil users (<500 mg), high dose verapamil users (≥500 mg), previous verapamil users and verapamil naïve patients. Data is presented as percentages or medians with range.
CH: Cluster headache; eCH: episodic cluster headache.
A 100% response was only achieved in 30/220 patients (14%) currently using verapamil, and there was no difference in the proportion of 100% responders compared to verapamil-naïve patients or the total population. In both patients using high and low dose verapamil, 100% responder rates were identified. It is worth noting that 100% verapamil responders also responded well to acute treatment, especially triptans.
Regarding verapamil and sleep, we found that ESS scores (Mean (SD): 8.47 (5.69) vs. 9.40 (6.20), p = 0.203) and PSQI scores (Mean (SD): 9.41 (4.15) vs. 8.94 (4.27), p = 0.363) did not differ between patients in bout with and without verapamil treatment (n = 271). No differences in ESS or PSQI were found between patients using high and low dose verapamil.
Other preventive treatments
Compared to verapamil, use of second-line therapy was infrequent with lithium being the therapy most commonly reported. Lithium was currently used by 18 patients (5%), all cCH patients. Only three patients (17%) were 50% responders. Indomethacin was mainly used as an add-on, but 7/8 were 50% responders. Patients currently treated with gabapentin, topiramate or candesartan at 50% responder level were less frequent, respectively 30%, 50%, and 44%, but the populations were small (Supplementary Table 4).
Transitional
In total, 92 patients (23%) had tried transitional treatment and 28 were current users. The most frequent current transitional medication was GON blocks (22 out of 28, 79%) and of these 16 out of 22 (73%) were 50% responders but only two patients were not treated by additional preventive therapy. Oral prednisolone was used by six patients (25–75 mg) and none were 50% responders. No further analyses were done.
Medically refractory group
Thirteen patients (3%) were identified as having medically refractory cCH according to proposed EHF criteria (18), defined as a cCH patient with at least three severe attacks per week and who had failed at least three preventive agents. Females dominated this group (n = 11), with only two males meeting the criteria. The median age was 47 (range: 23–59) and median CH duration was 24 years (range: 1–44 years). Eight patients were not currently on preventive treatment, but five still used various preventive treatment with little or no effect. These patients had previously tried an average of 3.7 (range 3–6) different preventive treatments.
Their median attack duration was 75 min without medication and 22 min with acute medication, and median attack frequency was six per day. Oxygen was used by 10 patients and four were 50% responders. Triptans were used by seven and five were 50% responders.
Discussion
This study shows that eCH patients had a higher chance of achieving successful abortive treatment compared to cCH patients. Sumatriptan injection was found to be superior to oxygen in achieving complete relief, likely driven in part by a higher chance of relief in severe attacks. Verapamil was the dominant preventive therapy used, despite only achieving complete response in a small subset of patients. Effect of verapamil had no association with clinical features.
Acute treatment
Four randomized-controlled trials (RCTs) have examined oxygen treatment in CH (3,20–22). Five retrospective studies and one prospective study have investigated potential associations between clinical features and oxygen response (23–27). Already, in Kudrow’s landmark study from 1981 (28), oxygen was noted to be more efficient in younger eCH patients but this was not reproduced in a later RCT (3). Three retrospective studies also identified eCH patients as better oxygen responders (27,29,30); however, two retrospective studies (24,25) and one prospective study (23) failed to find a difference. The studies finding a difference (including this study), were based on 3973 patients, whereas the studies not finding an association were based on 702 patients. Overall, this indirectly supports our results that eCH patients respond better to oxygen therapy than cCH patients. Previously, clinical features such as restlessness (29) and photophobia/phonophobia (23) were suggested to decrease oxygen response; however, our study and two previous studies (24,30) could not confirm this. In the literature, there are conflicting results concerning oxygen and smoking (past/present) (23–25,27,29) but we did not find an association. In regard to sex and complete response, we found that males responded better than females, which is in line with a prior publication (27). Multiple other studies did not find an association with gender, but these studies did not single out the 100% responders. We did not find any association with treatment response and flowrates; however, the literature is inconsistent (21,25,31). These conflicting results suggest that the effect of oxygen is not a dose response but potentially an individual threshold response, meaning that oxygen concentration needs to exceed a specific concentration to be effective. Certain mask types might increase the effect of oxygen (22), but data on this was not collected. In the clinic, we encourage not excluding oxygen as a treatment before high flow and different mask types have been tried (22). Unfortunately, obtaining oxygen can be difficult and expensive for the patients in some countries and this may limit its usage internationally (27,30).
Our findings regarding triptans were in line with the few published reports. Sumatriptan injection has been found to be less efficacious in cCH compared to eCH (32). In a logistic regression analysis, triptan response was negatively associated with age (29) and not associated with male sex or eCH, but the number of variables tested was very high (33). We kept sex in our model because it almost reached a significant level and because previously published evidence support that females respond less well to triptans (34).
Sumatriptan injection was more efficacious than oxygen in achieving 100% relief among patients using both types of acute treatment. Schindler et al. (25,26) also compared sumatriptan injection with oxygen and found that triptans were more effective than oxygen if flowrates were below 10 L/min. Another study found that simultaneous use of triptans was associated with a favorable outcome from oxygen inhalation (23). A larger cross-sectional study did not find any such differences in effectiveness, but this was not among patients who used both types of medication and triptans were categorized as one and not subdivided into different forms of administration (30).
In our cohort, eCH patients reported fewer attacks per day compared to cCH patients (3.3. vs. 4.1 attacks/day). Combined with the more cyclical nature of the episodic patients, this raises the question of whether a drug tolerance or medication-overuse headache is negatively influencing the chance of a positive response to acute treatment in cCH. Development of tolerance has, to the authors’ knowledge, not been investigated in CH, and medication-overuse headache in CH patients is debated. Potentially, eCH and cCH patients may have different underlying biology since patients also present with different chronorisk (12) and respond differently to anti-CGRP antibodies (35) and non-invasive vagal neurostimulation (36).
Previous users of acute and preventive treatments might have stopped due to lack of effect, side-effects, contraindications or another reason altogether. We did not investigate potential adverse events, but oxygen has previously been found to be less likely to have complications compared to triptans (30). Among current users, oxygen was used in almost every attack (94%) but triptans were only used in around half of all attacks. This coincides with the recommended two triptan applications per day (mean: 3.7 attacks/day).
Preventive treatment
Verapamil was the most frequently used preventive treatment, with 220 out of 250 current users. Based on the literature, we hypothesized that cCH and females would be negative predictors of effect (5), but we did not identify any associations between clinical features and effect. The 100% responders constituted 14% of current users, which was less than expected based on previous studies (37,38). Even though we did not identify any apparent phenotype differences, 100% responders are interesting and should be investigated more extensively. Numerically, responders to the first line of treatment drank twice the amount of alcohol compared to non-responders, perhaps due to alcohol provoking attacks.
Lethargy is described as a common side effect of verapamil (39), but CH is also associated with sleep disturbances (40). However, ESS and PSQI scores for cCH patients or eCH patients in bout with and without verapamil did not differ. Therefore, the lethargy is probably attributable to or masked by CH.
Preventive treatments, other than verapamil, were not commonly used and therefore no firm conclusions can be drawn. Lithium, topiramate and gabapentin may have serious side effects on quality of life and may lead to discontinuation of the treatment (41–43). It is worth noting the high number of 50% responders using indomethacin as an add-on medication, indicating that indomethacin is not only efficient in the rarer trigeminal-autonomic cephalalgias.
Chronic medically refractory CH patients, of whom the majority were female, were uncommon and only constituted 3% of the total population and 9% of the chronic population, mainly recruited from a tertiary headache center. This might be underestimated due to patients participating before refractoriness is established. To the authors’ knowledge, no prior publication has estimated the prevalence based on EHF criteria. Importantly, less than half the medically refractory patients were 50% responders for acute treatment, and sumatriptan appears to have reduced effect in frequent users and cCH patients (32,44).
In our study, we defined a 50% responder as having a frequency reduction of more than 50% and only 57% of current users achieved this. Despite a partial response, these patients may have an impaired quality of life and may struggle with side effects. This also emphasizes the need for more effective preventive treatments for CH.
Treatment pattern and naivety
Treatment naivety rates were lower for both triptans and oxygen (19% and 12%, respectively) compared to a large internet survey from the USA in which 26% were triptan naïve and 33% were oxygen naïve (30). Two European studies also found lower use of oxygen (13.5–37%) and sumatriptan injection (2.4–45%); however, these data were collected on first visit to a headache specialist and therefore were not directly comparable to our cohort, and naivety may influence the distributions (45,46). Verapamil-naïve patients (22%) were also fewer in our cohort compared to previous publications (26,45–47). Still, one would expect that a cohort recruited primarily from a tertiary center would have few naïve patients. A possible explanation is that some of the patients were given the questionnaire at the first consultation. Only 23% reported use of transitional medication, which is lower than previous publications in which 34–65% had tried oral steroids (45–48).
Strengths and limitations
The advantage of our dataset was the large cohort with validated diagnoses and the semi-structured interview minimizing uncertainties and missing data. The response rate of 62% may suggest participation bias but it is similar to comparable studies (49). Patients were primarily recruited from a tertiary headache center, with the potential selection bias. The proportion of cCH patients was higher in our study than in a previous study from another tertiary headache center (45), but due to different methodologies the studies are not directly comparable. Consequently, results may only be representative for CH populations followed in tertiary headache centers where an overrepresentation of cCH patients is likely. Another limitation is that the treatment response was not the primary focus of the dataset. Power may be affected where post-hoc calculations were performed on relatively rare events (Supplementary Table 4). There is a risk of recall bias and no causality can be determined due to the retrospective design. In Denmark, the public health care system provides the patients with consultations and oxygen free of charge, and pharmacological medications are reimbursed to some extent (50). These opportunities provide treatment opportunities for all patients and minimizes the selection bias and social confounding; however, use of free-of-charge oxygen might be higher compared to other countries. Our use of perceived effect over time is different from the clinical trials; however, clinically, this measure is of utmost importance.
Conclusion
ECH patients respond more robustly to acute therapy than chronic patients. Effect of oxygen was associated with lower pain intensity and shorter CH duration, whereas efficacy of sumatriptan was not. Complete effect of acute therapy was most frequent among males and medically refractory cCH patients were mostly females. This study underlines the need for increased awareness of the effectiveness of existing therapies and new, more specific preventive treatment options.
Clinical implications
Episodic cluster headache patients respond better to acute therapy than chronic cluster headache patients. Oxygen response is more dependent on clinical features than sumatriptan response. Sumatriptan injection is better than oxygen in achieving complete relief. Female patients are most frequently refractory. Only 57% of current preventive users are 50% responders.
Supplemental Material
sj-pdf-1-cep-10.1177_0333102420970455 - Supplemental material for Real-life treatment of cluster headache in a tertiary headache center – results from the Danish Cluster Headache Survey
Supplemental material, sj-pdf-1-cep-10.1177_0333102420970455 for Real-life treatment of cluster headache in a tertiary headache center – results from the Danish Cluster Headache Survey by Anja Sofie Petersen, Nunu Lund, Rigmor Højland Jensen and Mads Barloese in Cephalalgia
Footnotes
Acknowledgement
The authors would like to acknowledge the participants and study nurse Mette Frank Fisker.
Author disclosures
ASP reports grants from Tryg Foundation, personal fees from Novartis, from null, outside the submitted work; and work as a current or prior sub-investigator in trials sponsored by Eli-Lilly, CCH Pharmaceuticals and Autonomic Technologies.
NL reports grants from Tryg Foundation, Candy Foundation, and Cool Sorption, personal fees from Lectures for ABG investment, outside the submitted work; and work as a prior sub-investigator for Autonomic Technologies and Xenon Pharmaceuticals.
RHJ has been principal investigator in studies sponsored by Eli-Lilly and ATI and has given lectures for Novartis, Lundbeck, Allergan, TEVA and ATI.
MB has given lectures for ATI.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the Tryg Foundation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.