
Abstract
Background
A novel technique for injection of OnabotulinumtoxinA (BTA) towards the sphenopalatine ganglion (SPG) has shown promise in refractory chronic migraine (CM) and chronic cluster headache (CCH). Open label safety and efficacy data are presented here.
Methods
Patients with refractory CM or CCH who had received at least one injection and completed headache diaries were included. Efficacy was defined as ≥50% reduction in moderate-to-severe headache days for CM, or ≥50% reduction in attack frequency for CCH, at weeks five to eight.
Results
Over 261 injections, there were 123 adverse events (AE), of which one was serious. Most (93%) AEs were mild and all were transient. The 50% response to one injection was 81% for CM and 69% for CCH. The response gradually reduced over subsequent months for CM but stayed between 55% and 67% for CCH. Repeated injections were beneficial.
Conclusions
Injections resulted in improvement for both groups and was maintained with repeated injections. Repeat injection after three months may be beneficial in CM. Adverse events were not uncommon, but universally transient, presumably as a result of the mechanism of action of BTA. Repeated BTA injection towards the SPG could be an effective treatment for refractory CM and CCH. Larger, randomised, placebo-controlled trials are required.
Introduction
Despite being a treatable disease, migraine is the third most common cause of disability in the world and the most common amongst young women (1). Chronic migraine (CM) is defined as ≥15 headache days a month, of which at least eight days should fulfil the diagnostic criteria for migraine (2). CM patients experience high levels of disability anxiety and depression (3) and consequence restriction of their work and personal lives (4).
Cluster headache (CH) is less common, but is an excruciatingly painful condition which carries a high burden of disability and impacts patients’ social, financial and employment potential (5). Around 15% of CH patients have chronic cluster headache (CCH) (6), which is defined as CH occurring with no remission periods or remission periods of less than three months per annum (2). The first line oral preventative treatment is verapamil. However, this can cause cardiac arrhythmias, constipation, nausea and postural hypotension (7,8), limiting tolerability.
For those patients with CM and CCH who are refractory to, or cannot tolerate, conventional preventative treatments, alternative options should be considered. The sphenopalatine ganglion (SPG) has been a target for various different treatment techniques for intractable cluster headache including surgical ganglionectomy (9), intra-nasal administration of local anaesthestic (10), percutaneous radiofrequency ablation (11,12) and alcohol infiltration (13). Success rates ranged from 46 to 85% but effects such as permanent sensory loss, failure of the procedure or rapid wearing off of effect (14) were seen. More recently, an implantable neuro-stimulator has been used successfully with a more satisfactory safety profile (15,16). Unfortunately, the sole company providing this device has ceased to exist; therefore, it is not available to patients at present. Amongst migraine patients, trans-nasal administration of local anaesthetic was found to be an effective acute treatment in one randomised controlled trial (17), but required frequent administration (18). Electrical stimulation of the SPG during an induced migraine attack was beneficial to some patients in a small case series (19), but has not been investigated further.
Intramuscular injection of Onabotulinumtoxin A (BTA) in the head and neck is a safe and effective treatment for CM (20,21). Injection of BTA into the SPG is a novel technique that has shown promise in pilot studies of patients suffering from CM (22) and CCH (23). The SPG is formed by the synapse between parasympathetic preganglionic fibres from the superior salivatory nucleus and the postganglionic fibres, which provide innervation to the meningeal and cerebral blood vessels, lacrimal glands, and nasal, oral and pharyngeal mucous membranes (24,25). Injection of BTA at the SPG is considered to block the presynaptic release of acetylcholine (23), thereby preventing the passage of signals from the trigemino-cervical complex and activation of the trigemino-autonomic reflex, which are implicated in cluster headache and migraine (26).
This analysis of our early experience of open-label use of BTA targeting the SPG aims to provide evidence of the safety and efficacy of recurrent treatment with this novel method in CCH and CM patients who have not responded to conventional treatments.
Methods
Patient selection
All patients with resistant CM or refractory CCH who had received at least one percutaneous BTA injection at the SPG between August 2013 and June 2022 at the University Hospital in Trondheim, Norway, were identified for inclusion. All patients fulfilled International Classification of Headache Disorders-3 criteria for their diagnosed primary headache disorder (2). Resistant CM was defined as failure to respond to at least three classes of migraine preventatives and at least eight debilitating headaches per month for at least three months without improvement, according to European Headache Federation consensus (27). Refractory CCH was defined according to a pilot study of the same treatment (23) as failure to respond to at least two evidence-based oral preventative medication for CH. This definition was based on a criteria proposed by Silberstein et al. (28) and considered as moderate intractability. The consensus statement on the clinical definition of refractory CH from the European Headache Federation, published after the start of the inclusion period for this study, was not applied (29). The evidence based classes of preventative treatment for chronic migraine were defined as: anti-epileptic drugs (e.g. sodium valproate, topiramate), anti-depressants (either tricyclic or selective serotonin (-norepinephrine) reuptake inhibitors), beta blockers (e.g. propranolol) and angiotensin receptor blockers (candesartan) (30). Evidence based preventative treatments for cluster headache were defined as: verapamil, lithium, methysergide, topiramate, ergotamine, sodium valproate, melatonin, baclofen and steroids (31). The study was carried out in accordance with the Declaration of Helsinki and was approved by the Regional Committees for Medical and Health Research Ethics Mid-Norway (reference 476799). All patients provided their written informed consent for participation in the study.
Data collection
For the efficacy analysis, only subjects who had received open-label treatments and had complete headache diary data were included. Subjects were required to prospectively complete a paper baseline headache diary for at least two weeks prior to the injection and another diary between weeks five and eight after every injection received. Additionally, where headache diaries were available for one, two, three and four months post injection (including in subjects receiving repeated injections), these were reviewed to determine the pattern of response over time to one injection. For CM patients, headache days were defined as a headache with a duration of ≥4 hours with a peak severity of moderate or severe intensity, or response to abortive migraine treatment, in accordance with International Headache Society migraine trial guidelines (32). Subjects scored the severity of the pain on a 1–4 scale (equating to mild, moderate, severe and unbearable). Safety data were extracted from previously performed prospective clinical trial data, and from patient records for those who had received the injection on a compassionate-use basis.
Injection protocol
With the subject supine, the skin and deep structures were anaesthetised with 3–5 ml of local anaesthetic and a 1–2-mm skin incision was made. Using the BrainLab surgical navigation system (Brainlab AG, Munich, Germany), and the MultiGuide injection tool, which has been described previously (22), BTA was administered towards the SPG (Figure 1). Either an infra- or supra-zygomatic approach was selected according to the anatomy seen on a computed tomography (CT) scan. Subjects received 25 units of BTA suspended in 0.5 ml of 0.9% sodium chloride for each injection. For subjects with cluster headache, injection was ipsilateral to the pain, unless a recent side-shift had occurred in which case, bilateral injections were given. Subjects with CM were given bilateral injections.

Demonstration of injection of OnabotulinumtoxinA injection towards the sphenopalatine ganglion using a lateral approach, with surgical navigation software and the MultiGuide injection tool. Photograph by Geir Mogen.
Repeated treatments
Subjects were offered repeat injection if they reported subjective improvement after the first injection. No objective, numerical criteria were set for offering repeated injections. Subsequent injections were offered after approximately three months, or after the beneficial effect had worn off (if greater than three months).
Statistical analysis
Data from the paper headache diaries were analysed using SPSS, version 28 (IBM Corp., Armonk, NY, USA). In the case of skewed data, Wilcoxon signed rank test was employed. Statistical significance was defined as a p < 0.05. For CM, efficacy was defined as a reduction in the frequency of moderate-to-severe headache days per month of ≥50% at weeks five to eight. For CCH, efficacy was defined as a ≥ 50% reduction in weekly attack frequency at weeks five to eight.
Results
Patient demographics
Table 1 shows the demographics and baseline clinical characteristics of included subjects.
Demographics and baseline clinical characteristics of included subjects.
Abbreviations: PREEMPT = Phase 3 Research Evaluating Migraine Prophylaxis Therapy clinical trial protocol; SD = standard deviation; NA = not applicable.
Chronic migraine
Eleven of the 12 subjects were female. The median age of the cohort was 43 years (range 24–68 years) and the median disease duration of the chronic phase of migraine was 14 years (range 2–40) at baseline. Subjects had failed a mean of 4.8 (range 4–11) preventative medications and all had failed cranial botulinum toxin injection according to the PREEMPT protocol (21). One subject was a non-responder to anti-calcitonin gene-related peptide (CGRP) monoclonal antibodies, but all other subjects were included prior to the availability of these treatments in Norway. At baseline, the mean number of monthly moderate-to-severe headache days was 15.3.
Cluster headache
Fifteen of the 31 subjects were female. The median age of the cohort was 49 (range 24–87) years and the median disease duration of 10 years at baseline (range 1–35 years). Patients had failed a mean of 3.5 preventative treatments (range 2–5).
Safety
Data from 261 treatments in 43 individuals were retrieved and are shown in Table 2. Subjects received a median of 3 treatments (range 1–29) with median follow-up of 22 months (range 1–104). One serious adverse event (AE) was recorded in the CCH group, which was an unplanned hospital admission to investigate facial asymmetry, resulting in magnetic resonance imaging of the head with no pathological findings. The facial asymmetry resolved within twelve weeks. A relatively large number of AEs were reported (123 over 261 treatments); however, the vast majority (93%) of these were mild. Importantly, all AEs were transient and most resolved within 12 weeks. Additionally, no subject discontinued treatment due to AEs. The most common AE in the CM group was jaw pain or difficulty chewing (n = 24) and for the CCH group it was mild intermittent visual disturbances (n = 23). Blurring of vision occurred after 28 treatments, of which 19 reports were from one individual. Other, less frequent, but clinically important AEs were mild to moderate transient diplopia (occurring after 1.9% of treatments) and clinically identifiable transient facial weakness (occurring after 1.4% of treatments). The mean maximal pain experienced during the procedure scored on an 11-point numerical rating scale was 3.5 ± 2.3.
Adverse events of OnabotulinumtoxinA towards the sphenopalatine ganglion in patients with chronic migraine and chronic cluster headache.

Efficacy in chronic migraine
Fifty-five injections were carried out in 12 subjects and headache diary data were available for 43 of the injections (78%) in 11 subjects (92%) which were used for analysis. Ten of these subjects had been injected as part of a previous clinical trial and two on a compassionate use basis. Patient flow through the study is shown in Figure 2.

Patient flow through the study. Abbreviations: n = number of patients receiving each injection.
Response rates in up to four consecutive injections
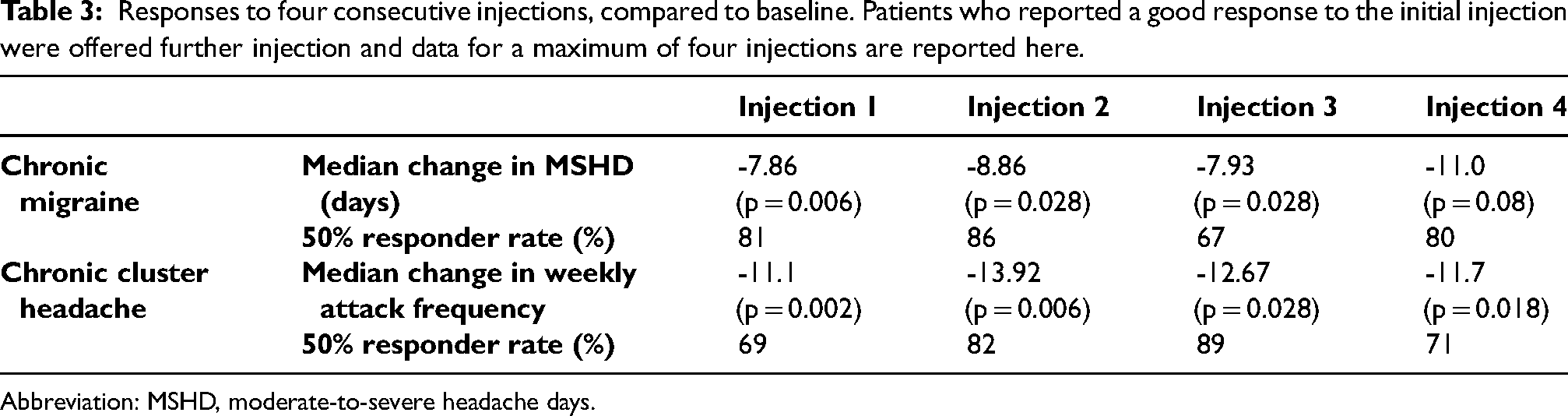
Table 3 shows the median change in moderate-to-severe headache days and 50% responder rates for up to four consecutive injections (measured at weeks five to eight after injection). The 50% response rate at weeks five to eight for the first injection was 81%. The response to further injections (in those who received them) were consistently high and is displayed in Figure 3.
Responses to four consecutive injections, compared to baseline. Patients who reported a good response to the initial injection were offered further injection and data for a maximum of four injections are reported here.
Abbreviation: MSHD, moderate-to-severe headache days.

The 50% response rates at weeks five to eight after injection, over four consecutive injections for chronic migraine and chronic cluster headache patients. Abbreviations: CM = chronic migraine; CCH = chronic cluster headache; n = total number of patients receiving each injection for whom headache diaries were available.
Response onset and duration after an injection
Figure 4 shows the 50% response rate at each month after a single injection (including patients who had repeat injection). Response peaked at months two and three and fell to 25% at month four.

The 50% response rates at months one to four following all administered injections (including patients having repeated injections due to good response). n = number of cases where headache diaries were available at each time point. Abbreviations: CM = chronic migraine; CCH = chronic cluster headache; n = total number of patients receiving each injection.
Efficacy in cluster headache
Two hundred and five injections were carried out in 31 individuals and, of these, headache diary data at month two were available for 92 injections (45%) in 14 individuals (45%). Seven of these individuals were injected in a previous clinical trial and the remainder were injected on a compassionate use basis. Patient flow through the study is shown in Figure 2.
Response rates in up to four consecutive injections
Subjects were treated with up to four consecutive injections. Table 3 shows the change in median attack frequency at weeks five to eight and 50% response rates after each of the four injections. The 50% response rate at month two for the first injection was 69%. The 50% responder rates for each consecutive injection are also shown in Figure 3, alongside the number of subjects who received each injection. The 50% responder rate was highest after the third injection (89%). By contrast to the CM group, two non-responders were given a further injection after the first one as they reported good effect. One of these subjects responded to the second injection and one did not. Despite this, the overall response rate was higher after the second injection than the first. Repeated injections appear to be beneficial in those responding to the first injection; however, it is not possible to state whether there is benefit in carrying out a second injections in non-responders at present.
Response onset and duration after an injection
Figure 4 shows the 50% responder rates for each month after a single injection (including patients who had repeated injections) which remained between 53 and 69% at each month.
Discussion
Safety and tolerability
This study demonstrates that BTA injection towards the SPG is well-tolerated, with patients reporting only mild pain at the time of the injection. Just under half the AEs were related to localised pain and swelling in the cheek or jaw at the path of the injection needle. It is possible that a small degree of localised spread of BTA occurred to extra-ocular and facial muscles, causing the diplopia, facial weakness and perhaps also contributing to the reduced masticatory power. Alternatively, there may have been some localised trauma from the needle itself. In the case of diplopia, examination by an ophthalmologist was consistent with weakness of the rectus inferior muscle. Importantly, these events all resolved fully within 12 weeks, presumably as the effects of BTA wore off (33).
Overall, our data demonstrate a comparable and perhaps slightly more favourable safety profile than those seen in the PREEMPT 1 and 2 studies of intramuscular BTA in CM (20,21), but few studies have utilised the percutaneous technique for injecting the SPG to allow direct comparison with our method. All injections in the present study were carried out using the percutaneous infra- or supra-zygomatic approach, which can be performed under local rather than general anaesthetic, further mitigating the risks associated with the procedure. Additionally, our method requires a single CT scan of the face and sinuses prior to the first injection for planning purposes, rather than repeated CT scans or fluoroscopy at the point of injection, reducing the exposure to radiation. By contrast to lithium and verapamil which require regular blood drug level monitoring and electrocardiograms respectively, no additional monitoring is required with SPG injection of BTA. Ongoing improvement of the technology used in this study is expected to improve the AE profile of this treatment.
Efficacy in CM
This open-label study shows that BTA injection towards the SPG is an effective treatment for CM, resulting in a 50% responder proportion of 81% two months after treatment. Open label studies of galcanezumab (34) and fremanezumab (35) for high-frequency and refractory migraine, have demonstrated a ≥ 50% reduction in monthly migraine days at three months of 66.7% and 58.3% respectively. For comparison, the 50% responder rate in the PREEMPT randomised controlled trial of BTA in non-refractory CM was slightly lower at 47.1% versus placebo 35.1% (p < 0.001) (36) and a placebo controlled trial of fremanezumab in refractory migraine patients showed 50% responder rate of 34% versus 9% for placebo (37). However, SPG injection is a more invasive process than both the PREEMPT protocol and anti-CGRP monoclonal antibodies and would likely be used where these treatments have been unsuccessful or not tolerated.
In our study, the maximum effect after all injections combined was seen at two months post-injection and the increase in 50% responder proportion between months one and two was large (9% versus 81%). The response continued to be positive at month three, but reduced greatly at month four, which is in keeping with the “wearing off” effect expected from BTA after three months (33). Similar to intramuscular BTA and CGRP monoclonal antibodies, this is a treatment which will need to be repeated several times a year. Our results would suggest that the optimum time for repeating the injection may be between months three and four, similar to the PREEMPT protocol. For those patients who went on to have more than one injection, 50% responder rates to subsequent injections continued to be high over subsequent three treatments (range 67–80%), although it must be stressed that the number of patients treated was small. A similar effect was seen in patients who completed all BTA injections in the PREEMPT study (38). However, it should be noted that in PREEMPT, patients who did not gain benefit from the first injection were not offered further treatment. This was also the case in our study because, although patients were allowed to choose whether to continue with further injections, no non-responders in the migraine group chose to have further injections. Overall, if a patient responds well to the first injection, they would appear to benefit from further injections.
Efficacy in CCH
High quality evidence for the oral preventative treatment of CH is lacking, with lithium and verapamil only gaining level C recommendations from the American Headache Society (39). In an open label study of verapamil, 60% of chronic CH patients obtained a > 75% improvement (40). In the only randomised, placebo-controlled trial of verapamil, 80% of episodic CH patients had a ≥ 50% reduction in headache frequency versus none in the placebo group (41). Although our open label study included patients who were refractory to a mean of 3.5 conventional treatments (of which verapamil is first line), the 50% response rate was still high (69%). For comparison, an open label study of greater occipital nerve block in patients with CCH showed a 50% response rate of 57% to the first injection (42).
In the CCH group in our study, there was a reduction in attack frequency at every month up to four months post-injection (where follow up was available). Although it is possible that there is some effect after the BTA itself has worn off, it should be noted that the data here is skewed towards those patients who had a longer duration of effect and maintained their diaries. Some of the patients who were “lost to follow up” had in fact been reinjected before the three month follow up period was complete and therefore did not have available data at weeks five to eight. Therefore, unlike in the CM group, it is harder to state when the optimum time for reinjection might be as there was no clear “wearing off” point. Although BTA could safely be offered again after three months, some patients may be able to wait longer between injections. One patient who had a <50% response to the first injection did respond to a second injection. Currently, there is not enough evidence to support the practice of routinely re-injecting non-responders, especially given the invasive nature of the procedure.
The 50% response rate at month one was 53%, suggesting that BTA injection could be helpful as a transitional treatment with quick onset during a crisis period, or when initiating an oral preventative medication. Patients with episodic CH were not included in this study, but there may also be a role for injection at the start of a bout, in a similar manner to greater occipital nerve block.
Limitations of the study and future work
Because this was a retrospective analysis of early experience with the technique, the sample sizes were small, especially for the CM group. Incomplete headache diary completion limited the inclusion of patients, particularly in the CH group, which introduces a risk of responder bias. Only a minority of the patients who did not return diaries gave a (subjective) report of being a non-responder to the injection. The patients included in our analysis were refractory to medical treatment, having failed a number of preventative medications (mean = 3.5 for CCH and 4.8 for CM); therefore, their response to BTA injection may not be representative of all patients. However, because it is invasive procedure, it is likely this treatment would be reserved for refractory patients.
The data for repeated injections should be interpreted with caution as the criteria for selecting patients for more than one injection were biased towards those who had subjectively reported good response to the first injection. Indeed, very few (n = 2) of the CCH group and none of the CM group who were not 50% responders chose to continue with treatment. Finally, the contribution of the placebo effect to the positive outcomes from this intervention should not be underestimated.
Conclusions
This open label study shows a positive response in patients with difficult to treat CM and CCH to BTA injection towards the SPG, with 50% responder rates of 81% and 69%, respectively, to the first injection. Repeated injections can be effective, although the criteria for selecting patients require refinement. The relatively quick onset of action in CH makes this an attractive option for treatment of disease exacerbations. The optimum time for re-injection would be between months three and four in CM, whereas a longer period between injections could be considered in CCH, depending on individual response. Although mild AEs were not uncommon, only one serious AE occurred in this analysis of our early experience. All AEs were transient, and none resulted in patients discontinuing treatment. Loss to follow up and small number of patients were limitations in this study. However, this open label evidence supports the rationale for the larger, randomised, placebo-controlled trials that are ongoing in both of these populations to further assess the efficacy of this novel treatment.
BTA injection towards the sphenopalatine ganglion could be an effective treatment for refractory chronic migraine and chronic cluster headache. Where injections are repeated, response rates remain high. One hundred and twenty-three adverse events occurred over 261 injections, but 93% of these were mild, and all were transient.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SH and KAJ have no conflicts of interest. LS receives research funding from The Wellington Hospital, London, UK. IA has stocks in Keimon Medical. TWM has been an honorary lecturer for Roche, TEVA Norway AS and Lundbeck AS and is a programme committee member for Lilly. He is a shareholder in Vilje Bionics AS and Keimon Medical AS. MSM serves on the advisory board for AbbVie, Abbott, Eli Lilly, Kriya, Lundbeck, Pfizer, Salvia and TEVA and has received payment for the development of educational presentations from AbbVie, Eli Lilly, Lunbeck and TEVA. He has received research grants from Abbott, Ehler's Danlos Society and Medtronic. He holds a patent (WO2018051103A1) on System and method for diagnosing and treating headaches. He is the chair of the medical advisory board of the CSF Leak Association. ET has Intellectual Property Rights for the MultiGuide device that is used in this paper and which is licensed to Man & Science. He is a consultant for and owner of stocks in Man & Science. He has received personal fees for lectures/ advisory boards from Novartis, Eli Lilly, Abbvie, TEVA, Roche, Lundbeck, Pfizer and Biogen, and has stocks and IP in Nordic Brain Tech. He also has stocks in Keimon Medical. He has received non-personal research funding from several sources, including EU, Norwegian Research Council, Dam foundation, KlinBeForsk. Commissioned research (non-personal): Lundbeck, Pfizer. DB may benefit financially from a commercialization of a proposed treatment targeting the SPG and the intervention device used to perform the treatment through intellectual properties rights and has consulted for Man & Science within the past 12 months.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Joint Research Unit between St Olavs Hospital and Norwegian University of Science and Technology, NTNU Discovery, The Liaison Committee between the Central Norway Regional Health Authority and Norwegian University of Science and Technology (grant number 9885, 244278, 12/9996).
Ethical statement
The study was carried out in accordance with the Declaration of Helsinki and was approved by the Regional Committees for Medical and Health Research Ethics Mid-Norway (reference 476799). All patients provided their written informed consent for participation in the study.