
Abstract
Cluster headaches both episodic and chronic are some of the most challenging headaches to treat. Although effective treatments are now available, some patients continue to be unresponsive to standard therapy. We present 17 patients from our practice whom we treated preventively with frovatriptan, a new triptan with a long half-life. The promising results suggest that this medication may be an useful addition to our ammaterium against this painful disorder.
Introduction
Cluster headache is one of the most severe forms of pain known to man. The new IHS criteria recognizes two forms of this disorder; episodic and chronic (1). Until recently, when effective treatments became available, it was known as the ‘suicide’ headache. Episodic cluster headache has been effectively treated with verapamil, methysergide, valproic acid, lithium and topiramate (2–6). Subcutaneous sumatriptan, oxygen and i.m. dihydroergotamine (DHE) are effective for aborting cluster attacks (7–11). These same therapies may be less effective for chronic cluster. Unfortunately, some chronic cluster patients refractory to treatment.
Episodic cluster headache is distinguished by cycles of cluster attacks separated by pain free intervals which may last from months to years. When patients reenter the cycle, it is common to provide an interim therapy, also known as transitional therapy, to achieve rapid pain free status while concurrently starting and building up preventive treatments. Traditionally, steroids have been used as transitional therapy for up to 2 weeks in duration, but is often associated with unacceptable side-effects (12, 13).
Chronic cluster headaches is characterized by the absence of remission periods (14). These patients are often refractory to treatment and are frequently disabled. Many of these patients are on multiple medications but still have frequent breakthrough headaches. Some of these patients eventually resort to surgery for relief.
We present here a retrospective review of the response of episodic and chronic cluster headaches to the open label use of frovatriptan; both as preventive and transitional therapy. The primary endpoint is frequency of headache occurrence.
Methods
The patient population was drawn from a tertiary headache centre. All patients met the IHS criteria for episodic or chronic cluster headache. Episodic cluster headache patients were seen early in their cluster cycle. They were then started on frovatriptan simultaneously with a cluster preventive medication typically verapamil. They stayed on frovatriptan for up to 3 weeks. Oxygen was allowed for breakthrough headache treatment. They were seen in follow-up 2–4 weeks after initiation of therapy and answered questions on the efficacy of frovatriptan in preventing headache occurrence.
Chronic cluster headache patients were typically started on daily doses of frovatriptan at 2.5 mg or 5 mg after having tried and failed multiple other preventives (see Table 1). In general, patients have been on stable preventive medication for 3 months before starting Frovatriptan. They were instructed not to take any other triptan or vasoconstrictor for breakthrough headaches but could instead take oxygen for this.
Patient characteristics and details of treatment

E, episodic cluster headache; C, chronic cluster headache.
Results
We divided frovatriptan response, as measured by change in number of cluster headaches, into 3 groups. Good response was defined as having at least a 75% improvement or greater. Moderate response was defined as a response of 25–75% and poor response was a response of less than 25%.
In the group of 9 patients with episodic cluster headaches, 8 of them had a good response with 100% relief with no cluster headaches while on frovatriptan (Fig. 1). One patient (no. 17) had a moderate response with 50% improvement in their headaches. This patient was newly diagnosed, probably chronic and was in the 10th month of his cluster cycle when he was treated. Relief from headaches was obtained within 48 h of initiation of frovatriptan. The episodic group of patient was treated with frovatriptan from 4 to 14 days.
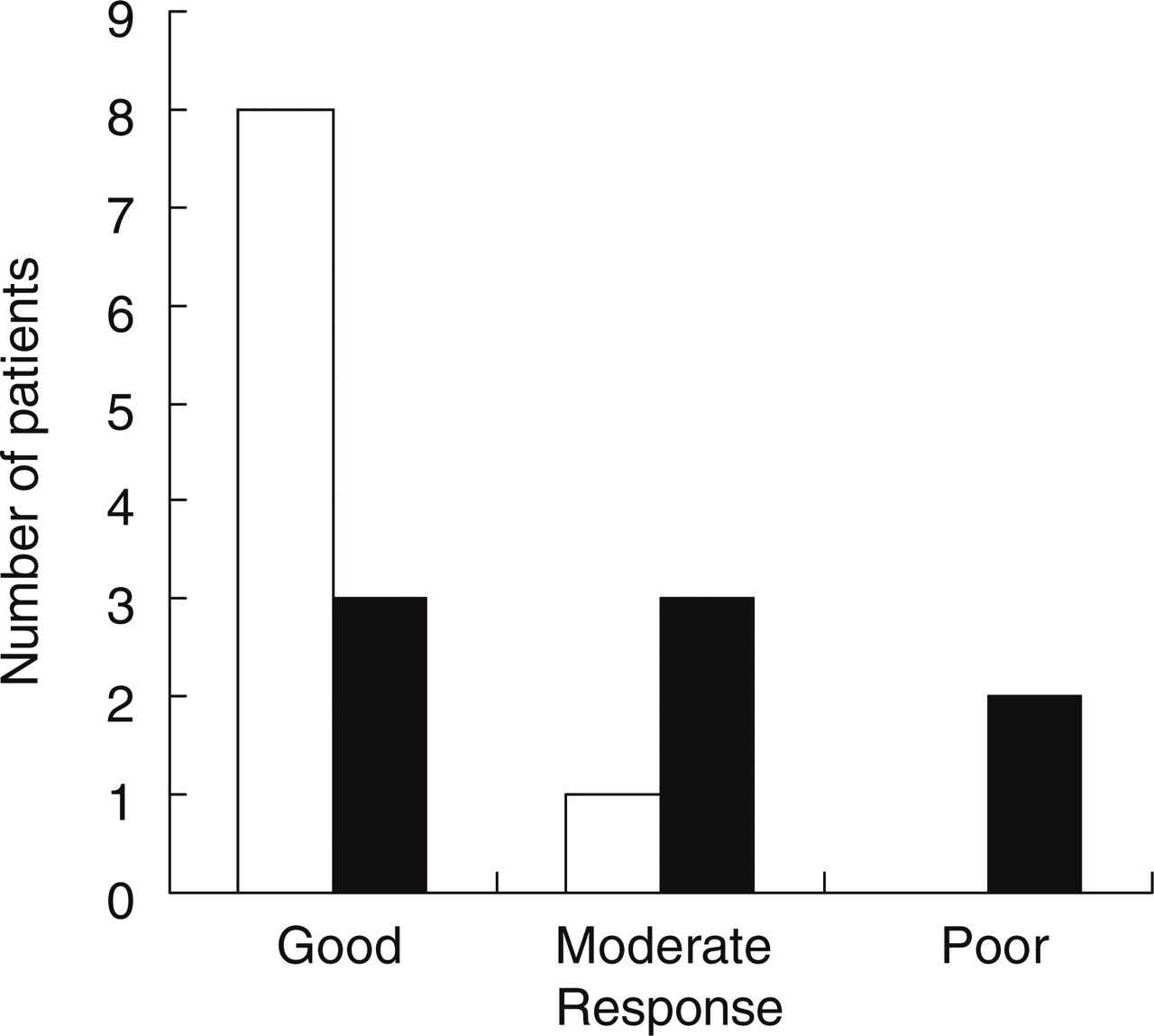
Response of episodic cluster headache (□) and chronic cluster headache patients (▪).
Of the 8 patients with chronic cluster headaches, 3 had complete relief (Fig. 1), 1 patient had at least a 75% response rate, 2 patients had 50% relief and 2 patients had no relief. Of these 7 patients, 1 took 5 mg q day, 6 took 2.5 mg bid and 1 took 2.5 mg q day. They remained on their prior preventive medications while on frovatriptan (Table 1).
No adverse events were reported with frovatriptan use in these patients. For the chronic cluster headache patients, 1 patient has been using frovatriptan continuously for 5 months and another for 8 months without reported adverse events.
Discussion
Episodic cluster headaches are usually easily treated once the correct diagnosis has been made. Verapamil, valproic acid, lithium and topiramate have been shown to be effective in cluster headache prophylaxis. These take time to titrate to effective doses. Traditionally, a bridging or transitional therapy has been given in these few weeks to provide quick relief from these intolerable headaches while the preventive medications are being increased. Cortico-steroids, and greater occipital nerve blocks, have been shown to be effective transitional therapies (15–17). Cortico-steroid use has been associated with adverse events and alternate transitional therapies should be considered (12, 13). Our study shows that frovatriptan is an effective transitional therapy and can be used safety with no increased adverse events in patients transitioning into longer term preventive therapy. Breakthrough headaches if any were easily treated with oxygen and generally relief from cluster pain was obtained immediately on commencing frovatriptan. The majority (8 of 9) of these episodic cluster patients had total relief and the remaining patient had at least a 50% response to frovatriptan on a total daily dose of 2.5 mg or 5 mg.
Patients with chronic cluster headaches make up a minority of cluster headache patients. They are the most difficult to treat. Many have tried and failed multiple preventive medications; or are only partially controlled. They have a poor quality of life with many being on long-term disability. The most intractable patients invariably seek more invasive therapy and different forms of surgery, e.g. trigeminal nerve rhizotomy, radiofrequency ablation of the trigeminal ganglion and gamma knife surgery have been performed with varying levels of success (18–20). More recently, deep brain stimulation and occipital nerve stimulators have been used with good results (21, 22). Naratriptan, another triptan with a long half life, has been reported to be effective as a prophylaxis for cluster headaches (23). The decision to try frovatriptan as chronic therapy was taken as a last resort before surgery. The response to frovatriptan was not as robust in chronic cluster headache patients as that for the episodic cluster patients. Three patients became totally pain free while on frovatriptan, 3 patients had at least a 50% response while 2 patients had no response. A higher maintenance dose was required with most being on the maximum recommended daily dose of 5 mg. Of the 3 patients who are doing well, 1 has been on a daily dose of 5 mg of frovatriptan for 8 months now, has been able to discontinue most other preventive medications and is able to work. Frovatriptan appears to be very effective as a transitional therapy for cluster headaches and is a valuable addition to the armaterium of medications used to treat chronic cluster headaches. This was an open label study and more controlled studies would be needed to better assess the promise of this new form of therapy for cluster headaches.