
Abstract
Introduction
Headache is a frequent but neglected side effect of angiography, and the criteria for angiography related headache have been based on only a few studies.
Methods
One-hundred and thirty nine patients who underwent cerebral angiography and 30 controls who underwent peripheral angiography participated in this prospective, non-randomized, case-control study. Participants were instructed to tell the angiography staff in case a headache developed and were questioned about their headache just after, 24 hours after, and one week after angiography.
Results
In the cerebral angiography group 42 patients (30.2%) had procedural headache compared to three of the controls (10%). Two different types of headache related to angiography were observed: one during angiography, which was related to contrast injection, and the other occuring within 24 hours. Both headaches were more frequent in patients with a history of primary headache, but were distinctly different from the premorbid headache. Headache characteristics are described in detail.
Discussion
Both types of headache related to angiography did not match the ICHD-3beta criteria for angiography headache, but were similar to headaches reported in studies that were not included in the current criteria. The timing and characteristics of these headaches are discussed in the light of our and previous reports. We suggest that the present ICHD-3 beta criteria are inadequate in properly defining angiography headache and should be revised in the light of the present literature.
Introduction
Despite the development of newer and less invasive techniques such as CT and MR angiography in the past decades, catheter angiography still remains the gold standard for the diagnosis of many intracranial vascular diseases. The complication rate of digital substraction angiography (DSA) has been reported to be 0.5–3.0% and embolic or hemorrhagic stroke, seizures, punction site related problems, contrast agent related problems and headache have been reported to occur in relation to DSA (1,2). Although not a serious problem, headache holds an important place among the complications of angiography, and its incidence varies between 0.3–51% (3,4,5).
Suggested causes for angiography related headache are irritation of the trigeminovascular system by contrast agents or mechanical stimuli such as the catheter itself. One or more factors may lead to activation of platelets or irritation of the vascular endothelium, resulting in the release of vasoactive peptides and subsequent development of a headache (3,5,6,7).
International Classification of Headache Disorders-3 beta.

Methods
One-hundred and thirty nine patients who underwent cerebral DSA in the Interventional Radiology Unit of the Akdeniz University Hospital, Antalya, between 2013–2015, and who agreed to participate, were included into the study, and 30 patients who underwent peripheral angiography served as a control group. All patients and controls provided informed consent and a local ethics committee provided approval. This was a prospective, non-randomized, case-control study. Patients and controls matching the study criteria were selected in order of admission.
Indications for DSA were stenosis detected on a MRA/CTA in a patient without any symptoms of stroke/TIA in 29%, cerebral infarction in 40%, transient ischemic attacks in 9% and clarification of a suspected AVM or aneurysm detected on other neuroimaging modalities in 22%. Patients with subarachnoid hemorrhage and patients who presented with secondary headaches due to the reason for DSA were not included in order to avoid interference with the angiography-related headache. Patients who were aphasic, comatose or too confused to answer the questions were not included. Because sedation during the procedure may interfere with the patient’s ability to properly feel, grade, understand and remember the characteristics of any headache during angiography, patients who were sedated were also not included.
Before the procedure, all patients and controls were questioned about their prior history of headaches. Characteristics of the premorbid primary headache were noted in detail. All patients and controls were instructed to tell the angiography staff in case a headache developed, and a detailed headache questionnaire was provided for the angiography staff to fill out. All patients and controls were informed about the possibility of “flushing” after the injection of contrast media, and were instructed to differentiate this phenomenon from a headache. After angiography, all patients and controls were seen face to face within 6 hours and were asked about any new developing headache. They were given a chart to fill in the characteristics and timing if any headache developed within the first 24 hours, and within one week of the procedure. All participants were either seen in person or contacted by phone 24 hours and one week after the procedure, and asked if any headache had developed.
Statistics were analyzed with the help of the SPSS 21.0 software program. Relations between categorical variables were analyzed by Fisher’s Exact test or Pearson chi-square test. The Mann-Whitney U test was used to compare two groups of means when the data were not distributed normally. P < 0.05 was considered as statistically significant.
Results
The mean age of the 139 patients in the cerebral angiography group was 58.2 ± 13.1 years, and there were 84 men and 55 women. The mean age of the 30 patients in the control group was 55.1 ± 14.2 years, and there were 27 men and three women.
In the cerebral angiography group, 42 patients (30.2%) had a total of 55 headaches. Thirteen patients had more than one headache. In the control group, only three patients (10%) had a headache. During the angiographical procedure, headache was seen in 10 patients (eight women, two men) in the patient group and in one male control. Within the first 24 hours after the procedure, headache was seen in 26 patients (13 women, 13 men) in the patient group and in one male control. Between days 1–7 after the procedure, headache was seen in 19 patients (nine women, 10 men) in the patient group and in one male control.
History of primary headache in patients undergoing cerebral or peripheral angiography (HA: Headache; AG: Angiography; PAG: Peripheral angiography; TTH: Tension-type headache; N/A: Not applicable).

Comparing patients undergoing cerebral angiography with headache to patients with no headache:
p = 0.001; bp = 0.000; cp = 0.149;
p = 0.01; ep = 0.02; fp = 0.077;
p = 0.063; hp = 0.01; kp = 0.74;
p = 0.001; np = 0.029; op = 0.034;
Characteristics of headache related to cerebral angiography: Timing, duration and location of headache (HA: Headache; AG: Angiography; PAG: Peripheral angiography; TTH: Tension-type headache; N/A: not applicable).

Characteristics of headache related to cerebral angiography: Intensity, quality and accompanying symptoms (HA: Headache; AG: Angiography).
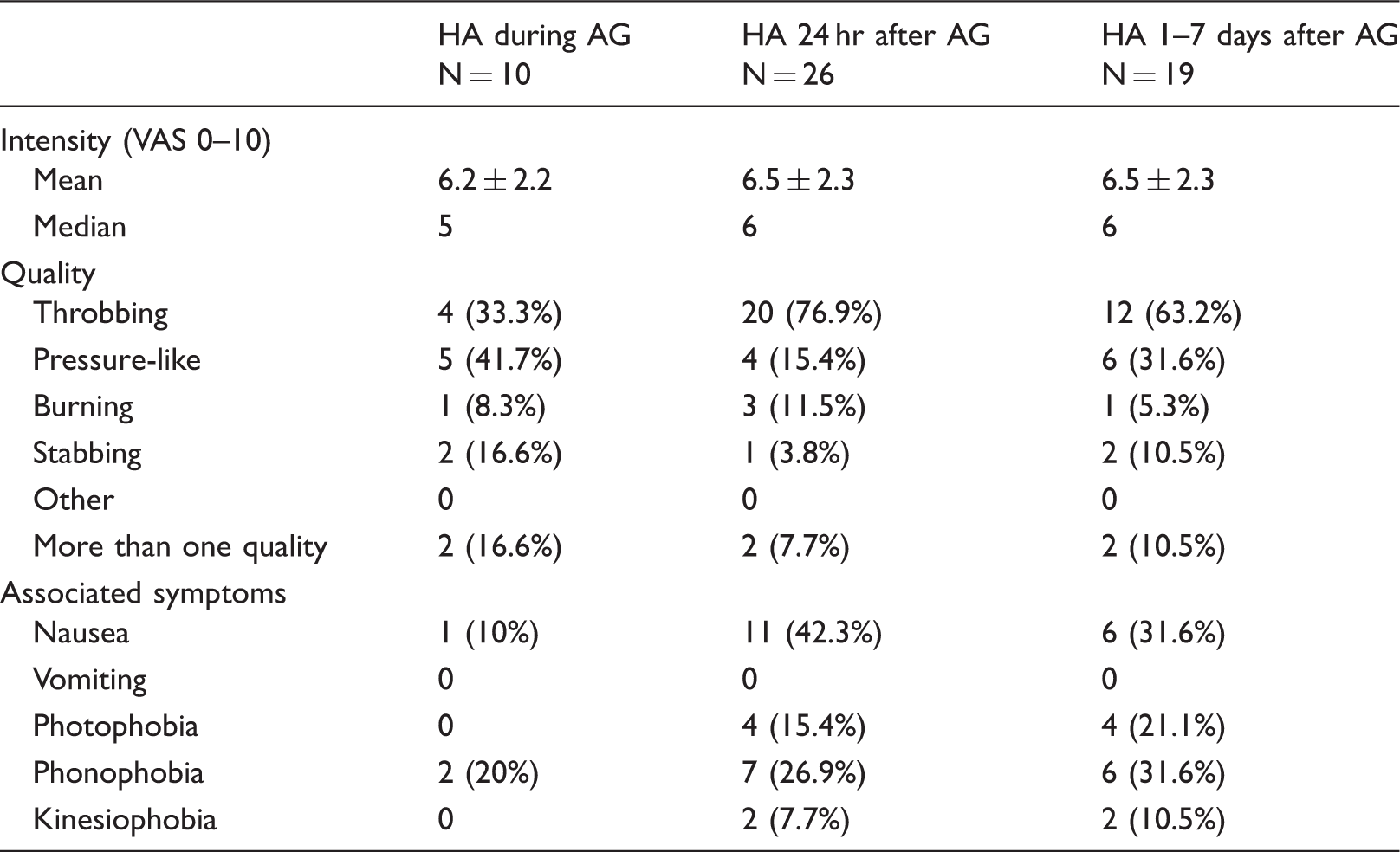
Headache that occured during the first 24 hours after the procedure was bilateral in most patients and one control, started approximately six hours after angiography and lasted about three hours. Pain was mainly generalized or located frontotemporally. The quality of the pain was generally throbbing and of moderate intensity. Nausea was seen in less than half and photo- or phonophobia in about 25% of patients. (Tables 3 and 4).
Headache that occured 1–7 days after the procedure was bilateral in the majority of patients and one control. Pain was mainly generalized or located frontotemporally. The quality of the pain was generally throbbing or pressure-like and of moderate intensity. Nausea was seen in 33%, and photo- or phonophobia in about 25% of patients (Tables 3 and 4).
Headache was more common in women (p = 0.042) when all headaches were combined, but the difference between genders was not significant in any of the time periods when analyzed separately. Due to the low numbers of headaches in the control group, a statistical comparison to the patient group was not possible. Headache was more frequent in younger patients (p = 0.037) when all headaches were combined, but this could not be shown for any of the time periods when analyzed separately.
In the cerebral angiography group, 65 patients (46.8%) had no stenosis, 27 (19.4%) mild to moderate stenosis, 32 (23%) severe stenosis and 16 (11.5%) carotid occlusion. All but four stenoses were in the anterior circulation. Nine of the 10 patients (90%) who had a headache during angiography had no stenosis on angiography. There was a correlation between developing a headache during angiography and not having a stenosis (p = 0.027). There was no correlation with degree of stenosis with the other headaches (p = 0.081). An aneurysm or AVM was detected in 14 (33.3%) and two patients (4.8%) with headache respectively compared to 19 (19.6%) and four patients (4.1%) without headache. The difference was not significant (p = 0.08). There was also no significant difference in the presence of an aneurysm or AVM when the headache subgroups were compared to patients with no headache.
Discussion
We report a headache frequency of 30.2% among our 139 patients who underwent cerebral angiography compared to 10% of our patients who underwent peripheral angiography.
Research in the literature revealed similar reported frequencies. Angiography headache was reported in 33% of 45 patients by Ramadan et al. and 22% of 64 patients by Gündüz et al. (5,10). In another prospective study, the reported frequency of headache during the procedure, and within 24 hours after, dropped from 51% to 35% when patients with subarachnoid hemorrhage were excluded as we did in our study (3). In a retrospective study, Kwon et al. reported the frequency of angiography headache as 56% (11). Methodological differences may explain the different rates of angiography headache reported. Asking the patient to pay attention to whether any headache develops prior to angiography or just questioning the patient afterwards, including or excluding patients with sedation or disorders that themselves cause headache, such as subarachnoid hemorrhage, may be listed as methodological differences.
We observed two different types of angiography related headache in our patients: one during and one after angiography.
The headache during angiography almost exclusively occurred while the contrast agent was selectively administered, even in the one patient who developed an intraprocedural headache in the control group. The headache lasted less than 30 minutes, was of medium intensity, with a pressure-like and/or throbbing character, and was always localised in the vascular area of the catheterized artery ipsilateral or bilateral frontotemporally. Nausea, vomiting, or photo- or phonophobia did not accompany this headache. A great majority (80%) of these patients had a history of primary headaches, but the present headache was clearly different from the prior headaches. We also found a correlation between developing a headache during angiography and not having a stenosis, solely for headaches occuring during angiography. A possible explanation for this might be that a lower concentration of contrast agent might have reached the brain compared to a completely patent carotid artery.
This headache we observed during angiography has only been reported in one study investigating angiography related headaches (10). In the studies of Ramadan et al. and Gil-Gouveria et al., all angiography related headaches developed hours after the procedure and none were reported to occur intraprocedurally (3,5). In the study by Kwon et al., the characteristics of angiography related headache were not investigated in detail (11). The relationship between contrast injection and the development of headache was not considered in any of these studies. Gündüz et al. reported that the headache during angiography lasted less than 10 minutes, was of mild intensity with a burning quality, and localised in the ipsilateral face and head (10). Unlike in our study, the headache was related to the degree of stenosis. The main difference between the headaches in these two studies is that, unlike ours, they reported none of the headaches to be related to injection of the contrast agent. It is well known that contrast injection frequently causes a temporary sense of heat in the head and face called “flushing”. But our patients were warned that this phenomenon may develop and were instructed to differentiate it from a headache. Headaches in both studies were located mostly ipsilateral to the catheterized vessel and were usually of less than 30 minutes’ duration. Gil-Gouveia et al. and Kwon et al. did not specify any criteria for angiography related headache, and used all headaches in temporary relationship with angiography as in our study (3,11). Ramadan et al. used the 1988 ICHD criteria for defining the type of headache, but the term “angiography headache” was not included in the ICHD-1 back then (5,12). Gündüz et al. used the second version of the ICHD criteria, where the criteria were the same as the ICHD-3 criteria but based only on the paper by Shouaib et al. (Table 1) (9,10,13).
Headache during cerebral angiography has also been evaluated in studies investigating headaches during endovascular therapeutic procedures. Gil-Gouveria et al. reported that 70% of the headaches occuring during endovascular procedures started immediately after injection of the contrast medium (6). The headache lasted less than 30 seconds, was of stabbing or pressuring character, of mild to moderate intensity and was located ipsilateral to the catheterized artery. Unfortunately all patients in that study were sedated, which makes it difficult to reliably evaluate the headache retrospectively.
In the light of these studies and ours, the characteristics of headache developing during angiography can be defined as a headache of mild to moderate intensity, with varying quality, mostly throbbing, pressure-like or burning, which is located either ipsilateral to the catheterized artery or bilateral. Despite some allegations, migrainous features or migraine headache do not seem to be a strict characteristic of this headache (5,9). Headache duration is short, and usually does not exceed 30 minutes. Our finding that this headache is closely associated with the administration of a contrast agent has been supported in one study but denied in another (6,10). The relation of this headache to the degree of stenosis is questionable. Headache during angiography is more common in patients with a history of primary headache, but the headache is distinctively different from the premorbid headache.
The second type of headache we observed within 24 hours of the procedure started approximately six hours after angiography, lasted about three hours and was of medium intensity, throbbing quality and generally was bilateral. Nausea, photo- and phonophobia were seen in frequencies comparable to migraine. This headache was also more frequent in patients with a history of primary headache, but did not show characteristics of the premorbid headache in more than half of the patients.
Gil-Gouveria et al. reported that the headache after angiography started within 10 hours of the procedure, was of mild intensity, stabbing quality and bilateral. Nausea and/or vomiting, photo- and phonophobia were seen more frequently than in our study (15%, 39% and 44% respectively). Premorbid primary headache was reported in 44% of patients, and as in our study the postprocedural headache was different from the premorbid one (3,6). In another study, the headache started approximately two hours after angiography, was unilateral in 60%, throbbing in 40%, and migraine accompaniments were present in about 25% (5). Kwon et al. did not give any detailed characteristics of the angiography headache, but reported that the headache resolved within 24 hours in 78% of their patients and was more frequent in those with cerebrovascular disease as the indication for angiography (11). We could not find any association between indication for angiography and headache, but in our study, in all patients, the indication was cerebrovascular disease.
In the light of these studies and ours, we conclude that headache within the first 24 hours after angiography usually starts 2–10 hours after the procedure, lasts about three hours, is located bilateral in the frontotemporal regions or is generalized, is of mild to moderate intensity and has a throbbing character. It is more common in those with a previous history of primary headache, but seems to be a different headache entity.
We think that the headache we observed during days 1–7 after angiography is difficult to relate to the procedure temporally.
Compared to many previous studies, our study shows some important differences. As our primary aim was to demonstrate the characteristics of headache during and after angiography, we took care to avoid circumstances that might cast doubt upon the origin of the headache. Subarachnoid hemorrhage is an important source of headache in the acute phase, as well as in the days or weeks after the insult, and might have interfered with the diagnosis of angiography related headache. Therefore we did not include any patients with subarachnoid hemorrhage, and all patients who were diagnosed with an aneurysm were patients in which the suspicion of an aneurysm was raised by other diagnostic modalities and who had never bled. Sedation during the procedure is an important disadvantage for patients in reliably remembering the exact timing and characteristics of the procedural headache. Therefore in our study we only included patients who were not sedated, except for the use of local anesthetics. Angiography related headache would be expected to occur either during or within 24 hours after the procedure. We followed up our patients up to one week after the procedure. In order to reveal the characteristics of the headache in detail, prior to angiography we instructed all participants to watch out for any headache that developed during and after the procedure. Doctors and nurses who performed the angiography were warned to fill out a standard form if the patient reported any headache. Another advantage of our study was that we had a control group consisting of patients undergoing peripheral angiography. Because pre-warning the patients that a headache may arise during angiography might trigger anxiety and headache in turn, it would have been difficult to tell whether or not the headache was caused by the procedure itself. Through the control group, we were able to exclude this nocebo factor’s contribution to the headache.
One limitation to our study is the difference in female/male ratios between the patient and control groups. On the other hand, the frequencies of prior headache histories were similar in both groups. Although it is well known that headache is more common in female patients, our numbers were too small to address the role of gender. Another important limitation is the small number of headache patients in our control group, which makes a satisfactory statistical comparison between the headache characteristics in both groups difficult. But because our main aim was to demonstrate headache characteristics related to cerebral angiography and their relation to prior headaches, we think that the numbers in our control group are satisfactory to show that headache is much more common with cerebral angiography compared to peripheral angiography.
Although angiography related headache is more common in patients with a history of primary headache, it generally does not show the characteristics of the premorbid headache. Therefore this headache should be distinguished from migraine triggered by angiography.
The International Classification of Headache Disorders version 3 beta defines angiography headache as given in Table 1. These criteria have some important limitations. They are based only on three studies (3,5,9), of which one is a retrospective study reporting complications of angiography in migraineurs, but which doesn’t deal with the properties of angiography headache itself (9). In the second study done by Ramadan et al., all headaches started hours after angiography and did not fulfill criteria C1 and C3a, but matched criteria C2 and C3b due to the migrainous character of the headache (5). In the study of Gil-Gouveia et al., the headache did not fulfill criteria C1 and C3a and most of the patients also did not match the migrainous headache criterion C3b (3).
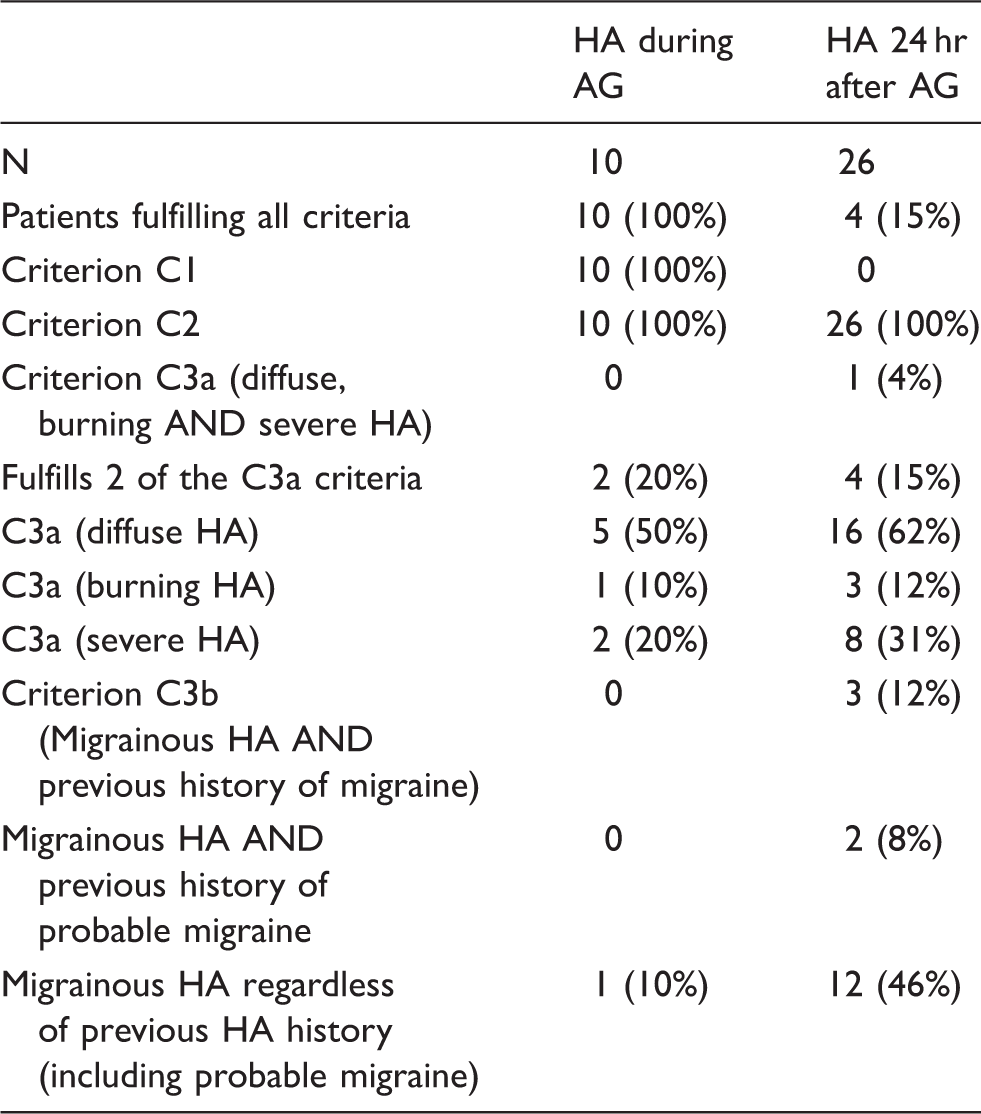
Patients with angiography headache fulfilling the ICHD-3 beta criteria for angiography headache (HA: Headache; AG: Angiography).
Given the data on angiography headache published after the criteria had been published, and the results of our study, we think that a revision of the current criteria, taking into consideration the following suggestions, would be needed. Headaches developing during and 24 hours after angiography seem to be two different headaches with different characteristics. The relationship of headache during angiography to injection of a contrast agent should be evaluated in more detail. If a certain relationship can be demonstrated, this headache could be classified elsewhere (for example section 8: Headache due to a substance or its withdrawal).
Criterion C seems to be unsuitable to define all headaches occurring in relation to angiography. It does not include headaches that do not start during the procedure due to criterion C1. We suggest revision of this criterion to “Headache may start during or within 24 hours after angiography”. We still think the exact time frame is debatable, and may be reduced further, as we found a mean starting time of six and median time of four hours after angiography. Another matter of debate would be whether these two headaches (headache during and within 24 hours of the procedure) should be classified separately as two different entities, as we found in our study. Criteria C1 and C2 could also be separated from criterion C and included in criterion B, as “Headache has developed during or within 24 hours after intra-arterial carotid or vertebral angiography and has resolved within 72 hours after the end of the angiography.” This could help criterion C to avoid mingling both timing and phenotype elements.
The weakest point of the criteria seems to be criterion C3; it restricts these headaches to either “diffuse AND burning AND severe” (criterion C3a) or migrainous, but with the necessity of having a previous history of migraine (criterion C3b). Our results contradict this criterion, as the headaches are diffuse to some extent but neither burning nor severe in the majority of patients. Migrainous headache in a patient with a previous history of migraine is also an insufficient criterion, as can be seen in Table 5. Changing this criterion to include patients with probable migraine doubles, and including all migrainous headaches regardless of a previous migraine history, quadruples the number of patients matching criterion C3b.
We suggest that criterion C3a should be changed entirely to include at least two of the following features: unilateral headache; throbbing or pressure-like quality; moderate intensity; possible presence of nausea but no vomiting. Criterion C3b could also be extended to include all patients with migrainous headaches regardless of a previous history of migraine.
More studies on this not so rare, but neglected headache will help to further refine the ICHD criteria to excellency.
Clinical implications
There are two different types of headache in relation to angiography: one during angiography that was closely related to contrast injection and one that occurred within 24 hours. Both headaches are more frequent in patients with a history of prior primary headache, but are distinctly different from the premorbid headache. These headaches do not match the ICHD-3beta criteria for angiography headache, but are similar to the ones reported in the literature. The current ICHD criteria are insufficient to encompass all patients with angiography headache and should be revised.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.