
Abstract
Background
This study estimates the socioeconomic impact of migraine headaches on paid and unpaid work productivity in the adult German population in 1 year.
Methods
We used data on headache frequency (days per month) from a longitudinal population-based study. Prevalence estimates of migraine were derived from the Global Burden of Disease Collaborative Network. Demography data were derived from official statistics in 2017. Aggregate headache days in 1 year were translated to losses in paid and unpaid productive hours based on estimates of presenteeism and absenteeism along with other socioeconomic parameters. Paid hours lost were distributed across the industry sectors. In this way, an age-, gender- and industry sector-specific monetary value was calculated for paid hours lost. Unpaid hours lost were valued by assigning the unpaid activities to their nearest market substitute. In a last step, value-added multipliers derived from input-output tables were used to calculate the economic value chain effects.
Results
A total of 15.5 million persons (20 years or older) suffer from migraine in Germany. Our analysis shows that 60% of those have three or fewer headache days per month, while patients suffering chronic migraine (15+ headache days per month) account for 5.4% of the adult migraine population. Females bear 65% of the total 836 million headache days per year. The socioeconomic losses due to migraine amount to €100.4 billion (€6493 on average per patient) in one year.
Conclusion
In addition to time losses in paid work, migraine causes substantial socioeconomic losses to unpaid work activities due to its disproportionate prevalence among females. Economic value chain effects provide a novel perspective on losses beyond a patient’s time loss. Overall, the elements of socioeconomic burden provide a strong rationale that innovative migraine therapies could be of high value to society.
Introduction
Migraine is an illness that is associated with acute, and often sudden, attacks that can manifest as a host of different symptoms. Migraine is classified into episodic and chronic, based on the monthly frequency of migraine-related headaches experienced by the patient over the past 3 months (1).
The most common symptom of migraine is the unilateral headache of moderate to severe intensity that lasts from 4–72 hours. Other symptoms include nausea, vomiting, fatigue, photophobia and phonophobia (1). Migraine substantially impacts a patient’s quality of life (2), and the quality of life worsens with increase in disease severity (3). Patients suffering from migraine symptoms are impaired in their ability to engage in everyday activities (4). Migraine headache frequency was also found to correlate with being overweight, unemployed, and suffering from depression and anxiety (3). Due to the lack of curative therapy and the stigma associated with the disease (5), migraine poses a tremendous burden to patients and their families. This, collectively, adds up to a burden that affects the society in its entirety.
Migraine is more prevalent among females and its prevalence peaks in the working age group. The Global Burden of Disease study’s estimates of 2017 show that the prevalence of migraine globally is 18% among all age groups (6). The estimates from the Global Burden of Disease 2016 show that migraine is the second leading cause of years lived with disability worldwide, with low back pain and other hearing loss in the first and third places, respectively (7,8). In Germany, the prevalence of migraine amongst all age groups is higher than the global average at 21% (6).
In this study, we aimed to quantify the socioeconomic burden of migraine arising in the adult German population. We focused on migraine-related headaches experienced in 1 year. We used data on headache frequency from the German Headache Consortium (GHC) study, a longitudinal population-based study, together with prevalence estimates from the Global Burden of Disease (GBD) Results Tool (6) to calculate the number of experienced headache days. Furthermore, we translated this health burden into potential losses in productive time due to absenteeism and presenteeism in paid and unpaid work. Finally, we monetised those socioeconomic losses as sector-specific gross value added, which is a metric measuring economic activity from a macroeconomic perspective. We also examined the indirect and induced economic effects related to productive activities along the value chain using value-added multipliers.
Methods
The study population
To investigate the headache frequency of the prevalent migraine population in Germany, we analysed population-based cohort data from the GHC study. Supported by the German Federal Ministry of Education and Research, the GHC study started in 2003, details of which can be found in Yoon et al. (9). The current analysis is based on the follow-up period of the GHC study conducted between March 2010 and April 2012. During the follow-up period, information from 5159 participants was obtained. Participants’ age ranged from 21 to 71 and 53.2% of them were female. Participants completed questionnaires on headache frequency once every 3 months, giving a total of eight time points for which data were collected. Detailed headache characteristics were collected retrospectively during the first year using a longer version of the same questionnaire. A migraine diagnosis was made when respondents met ICHD-2 guidelines’ criteria for definitive or probable migraine (10). Further details about this follow-up period can be found in Schramm et al. (11). To quantify the socioeconomic burden of migraine in Germany, we included respondents who met the modified ICHD-2 criteria for definitive or probable migraine with or without tension-type headache. A total of 1272 participants (Figure 1) fulfilled the case definition relevant to our study (see characteristics by study wave in Supplemental Table S1).

Flow-diagram of the GHC study sample from 2003–2012, and included sub-sample in the current analysis.
To derive the size of the German migraine population in 2017 by age and gender, we used the prevalence estimates reported by the GBD Results Tool (6) and the population projection by the German Federal Statistical Office (12). This is shown in the left panel of Figure 2. The subgroups of interest for this study were males and females, stratified by the following six age groups: 20–29, 30–39, 40–49, 50–59, 60–69 and 70+ years old. This subgrouping was chosen for its relevance to the subsequent socioeconomic evaluation.

Data sources analysed to quantify the number of migraine-related headache days in Germany in 1 year.
Quantifying the migraine-related health burden
To quantify the number of migraine-related headache days in Germany in 1 year, we analysed the distribution of patients in terms of headache frequency for the eight observation time points of the GHC study. All available data points were pooled and averaged separately for males and females to reflect the mean number of migraine-related headache days per observation in 1 month. In this way, we were able to derive the distribution of the GHC sample across the following headache frequency categories: 0, 1–3, 4–7, 8–14, 15–19, 20–23 and 24+ headache days per month. The right panel in Figure 2 presents the distribution of migraine-related headache days at each of the eight observation time points. The average headache frequency distributions by gender were used to extrapolate headache frequency on the derived German migraine population for the 12 corresponding age and gender prevalence cohorts. Consequently, we computed and aggregated the number of resulting headache days for all the cohorts in one year.
Modelling the loss in productive time
To model the productivity losses related to the calculated number of headache days, we used estimates on the average amount of time spent per day on productive activities. This was done for the predefined age and gender subgroups to reflect the different economic profiles among the migraine patient population. The 2017 employment rates from official statistics (13) were used with the assumption that migraine patients in Germany are not subject to biased employment rates compared to the general German population. Using German national accounts and official labour market statistics, the employed migraine patients were assigned age-, gender- and industry sector-specific annual working hours (14–16). This was then divided by 365 to reflect average hours of paid work spent per day (not distinguishing between weekdays). Furthermore, age and gender-specific information from the German time use survey was used to determine the average daily amount of time spent on unpaid work (17). Unpaid work refers to productive activities with no direct remuneration and that are replaceable by other individuals. The following activities for unpaid work were considered: Gardening, improvements and home repair, preparation of meals, maintenance of dwelling, manufacturing and care of textile fabrics, purchases and procurement, planning and organization, informal care, childcare, other care and voluntary work.
After deriving these estimates on the average daily amount of productive time spent in paid and unpaid work, we estimated the productivity loss related to experiencing one headache day. As productivity impairment could not be derived directly from the GHC study data, assumptions on the occurrence of absenteeism (not going to work) and presenteeism (being impaired at the workplace) associated with a headache day were based on estimates from the literature. We used parameters on absenteeism and presenteeism from a study conducted in the United States examining the work impairment related to the onset of a migraine attack on a workday (18). In this selected study, patients with episodic migraine reported the impairment related to a migraine attack. While migraine attacks vary widely in their severity and duration, we used the estimates of that study to assume that 32% of the headache days were not associated with any productivity losses, 11% were associated with a full day of absenteeism from work, and 57% with some impairment while working (18). This, thereby, reflects the different potential impacts of a headache day on the patient’s productivity (18). The same assumptions on absenteeism and presenteeism were applied for unpaid work.
Monetary valuation of paid and unpaid hours
To attach a monetary value to the aggregated loss in productive time, we used a macroeconomic measure of gross value added based on the German national accounts (16). Taking its industry-specific values per working hour, the gross value added directly captures the value of lost hours in paid work.
Despite the fact that unpaid work contributes to a society’s prosperity by creating value added (19,20), unpaid work activities are not considered in the formal national accounts systems. To monetise hours lost in unpaid work nonetheless, we assigned the unpaid work activities to the industry sector of their nearest market substitute following the market replacement cost approach (also known as the proxy good approach), Supplemental Table S3 (21). This results in a hypothesised monetary value for unpaid work that is equivalent to the cost of purchasing the same service in the market. As monetised losses in paid and unpaid hours are not perfectly comparable, we present the gross value added values separately when describing the results.
Economic effects along the value chain
The calculations described so far quantify the potential direct effects associated with migraine and its associated consequences. An impact on direct gross value added implies, macroeconomically, further indirect and induced economic effects along the value chain. In our approach, the indirect effects are described as economic effects arising due to the intermediate consumption of goods and services from suppliers associated with every productive activity. The induced effects originate from household spending of income generated by direct and indirect economic effects. Therefore, to explore those potential spillover effects, we used Leontief multipliers derived from input-output analysis (22–24). Leontief indirect and induced multipliers for gross value added are industry specific and are based on input-output tables from German national accounts (25).
All input parameters used in this study are listed in Supplemental Table S2.
Results
The prevalence of migraine among the population of 20 years or older in Germany was found to be 23%, with notable difference between females and males at 29% and 17%, respectively. In absolute terms, the number of adult migraine patients in Germany is estimated at 15.5 million in 2017 (Figure 3).

Estimated absolute number of migraine patients of 20 years or older in Germany in 2017.
The migraine population experienced a total of 836 million headache days in one year. While almost no difference was observed in the distribution of headache frequency between males and females, 65% of the total headache days were experienced by females due to its gender-specific and disproportionate prevalence. The absolute disease burden was similar in the age groups of 30–39, 40–49 and 50–59 years old, indicating that migraine-related headaches are most prevalent in the working age groups.
Figure 4 presents the proportional distribution of migraine prevalence and resulting headache days across the headache frequency categories. Patients experiencing eight or more headache days per month contributed 47.4% of the overall headache burden of the migraine population. Patients with chronic migraine (15 headache days per month and higher) make up 5.4% of the migraine population but disproportionally contribute 25.5% of the disease burden in terms of accrued headache days. Additionally, the sum of headache days of the chronic categories adds up to a comparable total to that accrued among patients in the 1–3 monthly headache days category (25.5% and 25.6%, respectively).

Proportion of migraine patients and headache days by health state in 1 year.
The accrued headache days resulted in a potential loss of 1.22 billion productive hours in 1 year. Figure 5 depicts the losses in hours by gender, activity and work impairment types. Two thirds (64.6%) of the estimated productivity losses were experienced by females, and among all hours lost, more than half (55.2%) were losses due to unpaid work activities. Within the unpaid work activities, three quarters (75.1%) of hours lost were experienced by females.

Productive hours lost in 1 year by gender, paid and unpaid work and impairment types.
Valuing the estimated loss of productive time according to gross value added per working hour, the direct socioeconomic burden of migraine amounted to €26.8 billion in paid work and €22.0 billion in unpaid work. Additionally, further losses in economic activity along the value chain amounted to €31 billion and €20 billion due to indirect and induced effects, respectively. The estimated losses in one year (for the total population and per patient) are summarised in Table 1.
Aggregate socioeconomic burden of migraine in Germany in 1 year (total population and per patient).
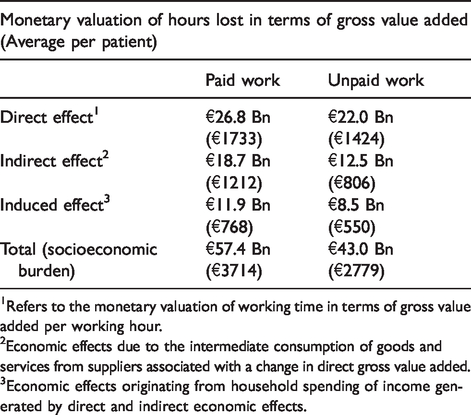
1Refers to the monetary valuation of working time in terms of gross value added per working hour.
2Economic effects due to the intermediate consumption of goods and services from suppliers associated with a change in direct gross value added.
3Economic effects originating from household spending of income generated by direct and indirect economic effects.
Discussion
As a disease with high epidemiological burden, migraine’s impact on society has ever been overcast by stigma, its historically obscure aetiology and the comorbidities often associated with the disease. In this study, we quantified the socioeconomic burden of migraine in Germany in 1 year. Our methodology covered the whole scope of the migraine population and accounted for the losses of paid and unpaid work. To date, no population studies were identified that measure the burden of migraine in Germany in terms of monetary losses due to both paid and unpaid work. Owing to the facts that migraine disproportionately affects females, and that females assume the bigger proportion of the overall unpaid work in Germany (26), the socioeconomic burden incurred by migraine has been, thus far, underreported.
Furthermore, while conventional cost of illness studies use individual income or hourly wages as a monetary valuation method, we monetised the burden of migraine-related headaches in terms of sector-specific gross value added. This is especially valuable since it sets the aggregate monetary figure in compatible relationship to the German national accounting system and enables our analysis to consider the potential economic effects along the value chain. In this way, we highlight the extent to which migraine burden affects the German society from a macroeconomic perspective.
Our estimates of direct losses of paid work and unpaid work due to migraine are consistent with European studies having a similar research objective. An analysis of the Eurolight project, which focused on the personal impact of headache disorders on affected persons in nine European Union countries, provides good grounds for validating our estimates on the elements of losses in paid as well as unpaid working time due to migraine (4). In the referred study, personal impact was operationalised, among other measures, as lost workdays, lost housework days, and lost social days. Steiner and colleagues (4) report that, on average, one workday and 1.5 housework days are lost per month for an average migraine patient. Dividing our aggregated estimates by the number of migraine patients and by 12 months to allow for comparison, an average of 3.0 hours of paid work and 3.6 hours of unpaid work are lost per migraine patient per month. In Germany, the average number of daily working hours of employees is 3.73 hours (calculated as the working hours per year divided by 365) (16). Similarly, the average daily hours of unpaid work reported in the German time use survey are 2.9 hours (17). Consequently, in terms of missed average daily working time, our estimates are in line with those reported by Steiner and colleagues (4).
Another publication from the Eurolight project estimated the economic resource loss due to headaches in Europe. Those losses were classified in terms of direct costs, namely medical resource use, and indirect costs due to work absenteeism and reduced productivity at work (27). In that study, the average gender-specific gross annual earnings per country were used for monetary valuation of lost productive time. In this way, the average annual productivity costs of migraine per patient in Europe were estimated at €1136 (27). Our estimate of direct paid work loss, in this case exclusively for Germany, was estimated at €1733 per migraine patient per year. Given the methodological discrepancy between the two studies and the fact that Linde et al. (27) reported the average results across several European countries, our estimate lies within a comparable range.
Assumptions and limitations
The epidemiological and disease inputs we used to calculate the health burden in terms of headache days per year were derived from different data sources. While the understanding of the nature of migraine-related headaches has been evolving over the years, inconsistencies with disease classifications and patient definitions might have compromised the certainty of our calculations when using different data sources. We utilised the estimates on prevalence and incidence of migraine in Germany from the GBD Results tool. The GBD study reports granular figures for the subgroups of interest to our analysis and combines evidence from different sources (28). It is worthwhile to mention that a publication stemming from the GHC study (9) is cited in the GBD Data Input Sources Tool website as one source for deriving the prevalence of migraine in Germany (29) (Supplemental Figure S1).
Another potential limitation to our study emanates from the fact that as migraine’s severity increases, it correlates with other comorbidities. We used average estimates on productivity losses from a study exclusively conducted on patients with fewer than 15 headache days per month (18). The study population considered in our study, nonetheless, included patients in all headache frequency categories. In this way, we assumed that all headache days (regardless of monthly frequency or intensity) have an equal impact on productivity. This assumption is thought to be conservative as it does not account for the probability of higher productivity loss among patients with more than 15 headache days per month.
On the side of socioeconomic valuation, it was assumed that the migraine population does not systematically differ from the general population in its potential for productive activity. Results from the International Burden of Migraine Study (IBMS) (3) and the American Migraine Prevalence and Prevention (AMPP) study (30,31) suggest that chronic migraine is associated with a lower probability of full-time employment when compared to episodic migraine. However, the same relationship between employment status and headache was not observed in some European studies (32).
We assumed that the impairment while working with a migraine-related headache is 25% based on the study from Landy et al. (18). This was found to be conservative when compared to a systematic review of US studies on adult migraine patients, which reported a range of 42–80% for effectiveness while working with migraine symptoms, which corresponds to 20–58% impairment while working (33). In order to further validate the impairment assumptions, we compared the implemented figures to a recent study on the burden of migraine in five European countries (34). In this study, the impact of migraine was studied as the impairment on the collective population level rather than the headache day level. Thus, Vo et al. (34) reported a 15.4 percentage points higher total work productivity impairment in migraine patients with more than four monthly headache days compared to matched controls not suffering from migraine. When adjusting the reported figures from Landy et al. (18) to derive a compatible figure for a simulated migraine population with varying headache frequencies, the impairment (as unweighted average for episodic and chronic migraine patients) was consistent at 15.3%. Nonetheless, this comparison is limited by the methodological differences between both studies.
To monetise unpaid work activities, we followed the so-called specialist approach within the market replacement cost approach. By doing so, unpaid work activities were matched and assigned to market substitutes of nearest resemblance from the industry sectors in the national accounts system. Thus, it was assumed that unpaid work activities consume the same intermediate inputs as paid activities in the industry sectors they were assigned to.
Additionally, we assumed that headache does not occur more often on working days than on free time and weekends. This might have led to a bias in our estimates. Landy et al. (18), however, report that migraine attacks do not occur disproportionally in working days.
Finally, it might be argued that patients experiencing a headache day could compensate for the lost work in a following longer working day or a weekend day. Since our calculations cover the losses in unpaid work, and given the fact that a patient’s time resources are eventually finite, we assume that a patient attempting to compensate for the work loss would naturally infringe upon their own capability of pursuing other work activities, be it paid or unpaid. For that reason, we valued the first instance of time loss experienced by the patient, without attempting to trace down compensation and displacement effects that would still, under a higher level of complexity and uncertainty, translate into different forms of productivity losses.
Conclusion
Migraine is a disease that shows the highest prevalence among females of working age. It is necessary to consider and incorporate socioeconomic losses beyond the formal labour market to fully represent the societal burden of a disease. As our study shows, unpaid work is a crucial component of the societal burden of migraine: 42.8% of the total estimated yearly burden of €100.4 billion in Germany is due to unpaid work. Therefore, we argue that unpaid work should be included in future analyses with similar research enquiry. For that purpose, it is necessary that data on work capability, including unpaid work activities, becomes more comprehensively and frequently captured in future surveys and clinical studies.
Our research also emphasises that the socioeconomic burden of a disease reaches beyond the confines of the affected individuals. Migraine does not only affect the patients from the productivity loss perspective, it also hampers the society’s potential towards greater prosperity. Moving forward, and acknowledging the limitations of our research methodology, we believe that quantifying and monetising the burden posed by a disease from a macroeconomic perspective serves as a valuable tool for policy analysis. This could help decision makers within the healthcare system and beyond when allocating resources and determining priority areas warranting innovation and intervention.
Finally, it has been noted in the literature that medical care for patients with migraine in European countries is inadequate (35,36). Our results emphasise the urgency of the matter and that effective migraine treatments could have huge potential in improving quality of life as well as economic welfare. In recent years, a number of new prophylactic therapies for migraine have received regulatory approval. Nonetheless, patient access to new therapies at country level is subject to the availability of robust evidence on their comparative value and the stakeholders’ capability to reach agreements that facilitate the adoption of new therapies. Our study, on this account, creates the means for stakeholders to engage in a broader and more inclusive discussion to arrive at evidence-based decisions in areas of resource allocation and priority setting in healthcare.
Article highlights
This is the first study to quantify the socioeconomic burden of migraine in terms of paid as well as unpaid activities together with the macroeconomic value-chain effects. Forty-one percent of the potential productive time lost due to migraine is time spent in unpaid activities that were to be undertaken by females. This study aims to broaden the perspective on potential areas of impact of a disease. The macroeconomic perspective enables an inclusive discussion in policy analysis and decision making in healthcare.
Supplemental Material
sj-pdf-1-cep-10.1177_0333102420944842 - Supplemental material for The socioeconomic burden of migraine: An evaluation of productivity losses due to migraine headaches based on a population study in Germany
Supplemental material, sj-pdf-1-cep-10.1177_0333102420944842 for The socioeconomic burden of migraine: An evaluation of productivity losses due to migraine headaches based on a population study in Germany by Ahmed H Seddik, Jennifer C Branner, Dennis A Ostwald, Sara H Schramm, Martin Bierbaum and Zaza Katsarava in Cephalalgia
Footnotes
Acknowledgements
The authors would like to thank Dr Jürgen Frensch (Novartis Pharma GmbH) for his intellectual contribution during the development of the study concept.
Author contributions
AHS managed and coordinated the study. AHS and JCB equally contributed in developing the study concept, conducting the data analysis and writing the manuscript. DAO and ZK supervised and gave input on developing the study concept. S.SCH provided the GHC study data. MB supported development of the study concept. DAO, S.SCH, MB and ZK commented on the manuscript at all stages.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AHS, JCB, DAO and S.SCH have nothing to declare. ZK received honoraria from Allergan, TEVA, Lilly, Novartis, Merck and Daiichi Sankyo. MB is an employee of Novartis Pharma GmbH.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Novartis Pharma GmbH and WifOR Institute.
The GHC study was supported by the German Federal Ministry of Education and Research (BMBF), Germany.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.