
Abstract
Background: Cluster headache (CH) is the most frequent trigemino-autonomic cephalgia. CH can manifest as episodic (eCH) or chronic cluster headache (cCH) causing significant burden of disease and requiring attack therapy and prophylactic treatment.
Methods: Treatment costs (direct costs) due to healthcare utilisation, as well as costs caused by disability and reduction in earning capacity (indirect costs), were obtained using a questionnaire in CH patients treated in a tertiary headache centre based at the University Duisburg-Essen over a 6-month period.
Results: A total 179 patients (72 cCH, 107 eCH) were included. Mean attack frequency was 3.5 ± 2.5 per day. Mean direct and indirect costs for one person were €5963 in the 6-month period. Direct costs were positively correlated with attack frequency (r = 0.467, p < 0.001). Burden of disease measured with HIT-6 showed a significant correlation with attack frequency (r = 0.467, p < 0.001). Twenty-four (13.4%) of the participants were disabled and not able to work.
Conclusion: CH leads to major socioeconomic impact on patients as well as society due to direct healthcare costs and indirect costs caused by loss of working capacity.
Introduction
Cluster headache (CH) is the most frequent of the so-called trigemino-autonomic cephalgias. The 1-year prevalence of CH is about seven to 119 per 100,000. In Germany about 5600 to 95,200 individuals were estimated to be affected. CH shows male preponderance (3.5:1) (1,2). It is characterised by severe unilateral attacks of head and facial pain lasting for 15–180 minutes. Attacks are accompanied by prominent ipsilateral cranial autonomic features (3). Most patients show a striking circannual and circardian periodicity of cluster attacks that may be caused by the underlying role of the hypothalamus (4). Headache occurs in about 85% of patients as episodic cluster headache (eCH), with a mean duration of the episodes of 8.6 weeks (5). The remaining 15% suffer from chronic cluster headache (cCH), in which no remission longer than 1 month occurs within 1 year (3). Treatment of CH consists of two main principles: (i) aborting acute attacks and (ii) prophylaxis. Attack treatment is performed with oxygen inhalation, subcutaneous or intranasal administration of triptans or intranasal lidocaine. Prophylactic therapy includes verapamil or lithium as treatment of first choice or steroids, topiramate, melatonin, long-acting triptans, and occipital nerve blocks (6,7). A minority of patients will not respond sufficiently to the above-mentioned therapies and therefore be considered refractory to attack treatment or prophylaxis (8). Invasive treatment options [occipital nerve stimulation (ONS); deep brain stimulation (DBS)] are suggested in some of these patients refractory to prophylaxis (9).
Frequent and chronic CH causes a high burden of disease as well as significant direct and indirect costs within the healthcare system (10–12). There is, however, a shortage of data about direct and indirect costs of CH, despite published single-case studies revealing high expenses for acute and prophylactic treatment (13,14). In a study from the headache centre in Copenhagen, a significantly higher number of days of work absence compared to the general population and decreased work ability during cluster episodes were reported in 82% of the patients. CH results in disease-related lifestyle changes in 96% of patients (12). Therefore, this study was carried out in a tertiary headache centre in cooperation with a healthcare management institute to estimate the expenses for treatment of eCH and cCH over a 6-month period. Further aims were the relationship between costs, burden of disease as well as attack frequency within the 6-month period.
Methods
Study design
This retrospective study focused on direct and indirect costs caused by CH. The observational period was defined from 1 January until 30 June 2010. All included patients were treated at the outpatient headache centre of the Department of Neurology, University of Duisburg-Essen, Germany, during this period by an experienced neurologist who diagnosed the headache type according to the ICHD-II criteria (3). The headache centre provides medical care for patients with difficult-to-treat headaches referred by neurologists, headache specialists or their insurance company in a metropolitan region with about 5 million inhabitants. Patients suffering from rare headaches or patients refractory to regular treatment were referred from all over Germany.
Inclusion criteria were: (i) diagnosis of CH, (ii) age≥18 years at study time, (iii) adequate knowledge of German language to understand interviews and study purposes. All study participants were interviewed about clinical characteristics, intake of acute and prophylactic medication, consultations of medical services, social environment and occupational background, absent days caused by CH within the above-mentioned 6-month period and partial or complete reduction in earning capacity. All interviews were done in July and August 2010. Informed consent was obtained from all patients. The study was approved by the local ethics committee. There was no financial funding of this study.
Research instruments
The custom-made questionnaire consisted of 28 items, including questions on socio-demography, and headache-specific data (e.g. onset and history of disease, frequency of attacks, acute and prophylactic medication). The five-page survey was developed by the authors. Time for completing the interview (face-to-face or telephone) was estimated to be less than 30 minutes. Interviews were performed by one trained medical student (J.F.) or the first author (C.G.). In terms of resource use, patients were asked about medications, outpatient visits, hospitalisations, rehabilitation, physiotherapy, osteopathy, absent days and reduction in earning capacity (partial or complete). In Germany, the definition of severely handicapped by law is graded from 0 to 100%. This is recognised as an equalising instrument offering various financial and other benefits. For this reason, chronically ill patients frequently apply for such a document. Therefore participants were asked about this topic. Additionally, the Headache Impact Test (HIT-6), a standardised questionnaire for measurement of impact of headache and headache-related disability, validated for use in German language, was obtained (15). The HIT-6 consists of six questions of which the first three ask for pain intensity, restrictions in daily activities and the wish to rest during headache attacks, whereas questions 4 to 6 ask for overall restrictions in daily life within the last 4 weeks. The headache impact severity level was categorised as follows: (a) little or no impact (49 or less), (b) some impact (50–55), (c) substantial impact (56–59), (d) and severe impact (60–78) based on the HIT-6 interpretation guide (16).
The number of attacks was calculated for the 6-month period by multiplying attack frequency per day with the individual period of cluster episode. The calculated total number of attacks during the study period was used as a measurement of impact of headache.
Analysis of direct and indirect costs of cluster headache
Direct and indirect costs of CH were calculated following a bottom-up approach; healthcare costs were estimated from a societal perspective. Intangible costs were not included in this evaluation. Costs were calculated for a time period of half a year. All costs are expressed in Euros and adjusted for the year 2010.
Unit costs were obtained from a number of sources. The costs of drugs were calculated based on the cheapest package of each medication. Each dose was estimated at 1 mg and multiplied by a patient’s individual daily dose. Items of the German medical fee schedule concerning costs of resource use through outpatient contacts were identified. Costs for hospitalisation were calculated according to relevant Diagnosis Related Groups (DRG) based on treatment of CH (G44.0) as the main diagnosis. Rehabilitation costs were estimated by average costs for neuro-rehabilitation per day (17). In addition, indirect costs caused by disability and reduction in earning capacity (partial or complete) were calculated according to the friction cost approach. The friction cost approach to estimating indirect costs means that the price of labour is set at zero after the friction period and is reduced to 80% during the friction period. We estimated a friction period of 3 months (17). The calculations for the cost per day from the societal perspective used average labour costs (18).
Furthermore, the impact of burden of disease and correlation with attack frequency on treatment costs was evaluated.
Costs of illness were calculated through multiplication of estimated prices and the resource consumption.
Statistics
Statistical analysis was done with the statistical package SPSS PASW Statistics 18.0.0. Descriptive statistics are presented as means ± standard deviation (SD). Chi-squared tests were used for comparison of categorical variables and t-tests for comparison of numerical variables. Correlation was used for coherences of several variables among each other; p-values below 0.05 (two-tailed) were defined as significant.
Results
Patient characteristics
Patient characteristics

eCH: episodic cluster headache; cCH: chronic cluster headache.
In the period reviewed, 135 patients had cluster attacks with 63 patients (46.7%) belonging to the eCH cohort. On average, patients had 3.5 ± 2.5 attacks per day (cCH: 3.8 ± 2.6, eCH: 3.3 ± 2.4; t =−1.508; p = 0.133) with a range from 1 to 12 attacks per day. The mean duration of bouts was 10.6 ± 7.5 weeks with a minimum of 1 week to a maximum of 6 months.
Attack-aborting medication was taken by 132 (73.7%) patients [(eCH: n = 66 (61.7%); cCH: n = 66 (91.7%)]. CCH patients took significantly more attack-aborting medication than eCH patients (χ2 = 20.783; p < 0.001). The allocation of intake of attack-aborting treatment and drugs is shown in Figure 1.
Attack-aborting treatment and drugs in 132 chronic and episodic cluster headache patients.
A total of 124 patients (69.3%) took prophylactic medication [63 (87.5%) of the chronic, 61 (57%) of the episodic patients (χ2 = 19.602; p < 0.001)]. The majority of the patients (n = 47; 37.9%) were treated with combinations of prophylactic medication. The allocation of intake of different prophylactic drugs is shown in Figure 2.
Prophylaxis with drugs in chronic and episodic cluster headache patients (n = 124).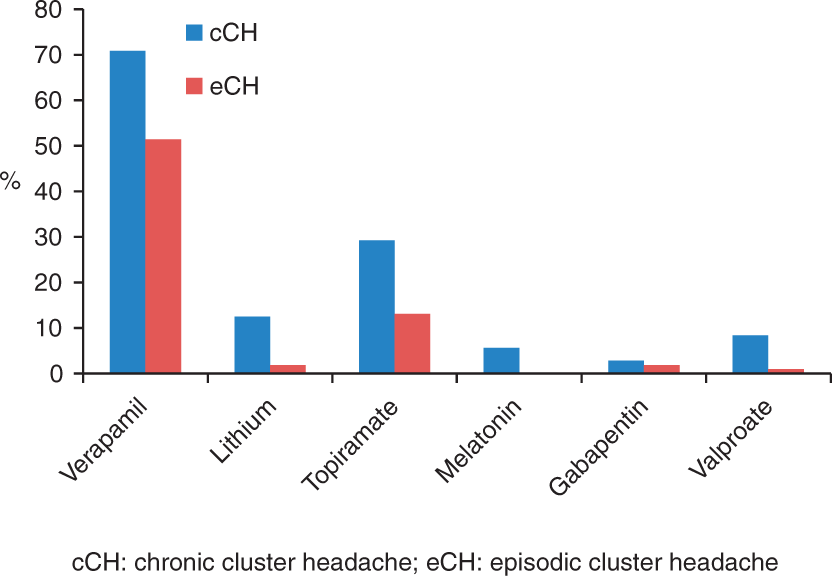
Exclusively consultations because of CH were captured for this study. The majority of patients received outpatient treatment. They consulted the outpatient headache centre of the Department of Neurology and sometimes in addition physicians in private practice. Fifty-three (73.6%) of the cCH patients consulted the outpatient headache centre with an average number of 1.8 ± 1.1 visits (range 1–6) during the 6-month study period. Forty-one (38.3%) of the eCH patients consulted the headache centre on average 1.9 ± 1.7 times with a range from 1 to 8 visits (p < 0.001). A neurologist in private practice was consulted by 19 cCH patients (26.4%, 4.4 ± 6.7 visits per patient) and by nine eCH patients (8.4%, 3.7 ± 1.9 visits per patient). General practitioners were consulted by 19 cCH patients (26.4%, 12.4 ± 17.3 visits per patient) and by 22 eCH patients (20.6%, 7.6 ± 12.6 visits per patient). A neurosurgeon was consulted by four cCH patients (5.6%, 1.8 ± 1.0 visits) and by one eCH patient (two visits). Six cCH patients (8.3%) visited a pain specialist 7.3 ± 5.2 times and one eCH patient went to a pain specialist five times.
In total, 15 of 179 patients (8.4%) were treated as inpatients in the Departments of Neurology, Neurosurgery or Neuro-Rehabilitation. Five cCH (6.9%) with eight hospital stays had a mean duration of 6.3 ± 1.5 days (range: 3–7 days) in a Department of Neurology and four eCH (3.7%) with five hospital stays had a mean duration of 7.4 ± 8.2 days (range: 1–21 days). Two cCH (2.8%) had two hospital stays in a Department of Neurosurgery with a mean duration each time of 10 ± 1.4 days (range: 9–11 days). Inpatient treatment in a Department of Neuro-Rehabilitation was done by 4 cCH (5.6%) with a mean duration of 29.8 ± 8.8 days (range: 21–42 days).
Costs per patient in the 6-month period
Costs of attack-aborting treatment per capita; drug treatment is dose-adjusted
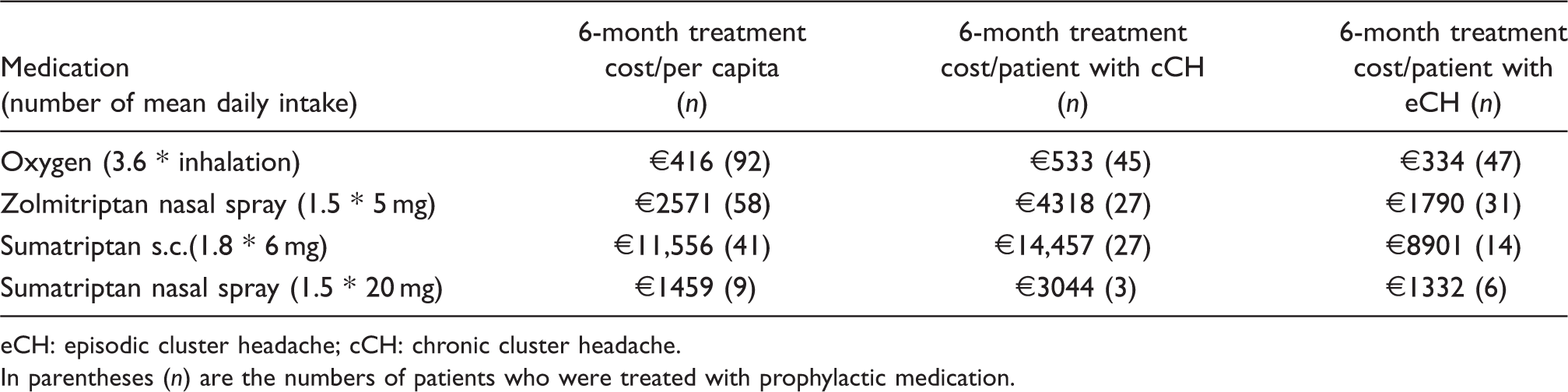
eCH: episodic cluster headache; cCH: chronic cluster headache.
In parentheses (n) are the numbers of patients who were treated with prophylactic medication.
Costs of prophylactic medication for different treatments per capita

Not used by any patient; eCH: episodic cluster headache; cCH: chronic cluster headache.
In parentheses (n) are the numbers of patients who were treated with prophylactic medication. Drug costs are dose-adjusted.
Total costs for all patients in the 6-month period
The following data refer to overall costs of all participants, namely 179 patients (72 cCH and 107 eCH patients). The costs of acute medication account for a total of €694,582 (cCH: €531,288 and eCH: €163,294) (Figure 3).
Allocation of total costs for several attack-aborting treatments (per 6 months).
The costs of prophylaxis accounted for a total of €39,378 (cCH: €26,171 and eCH: €13,206). Most of these costs are attributed to verapamil (€14,199 = 45.3%) (Figure 4).
Allocation of total costs for several prophylactic medications (per 6 months).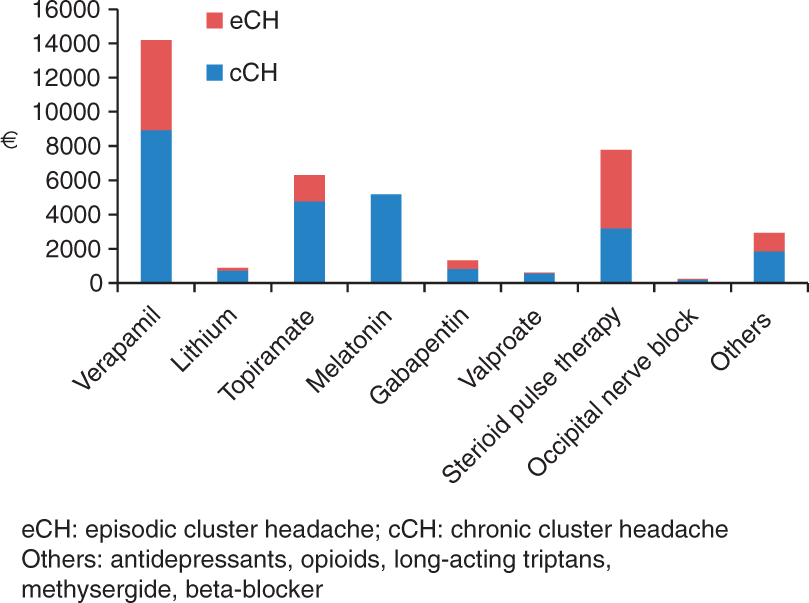
Costs and reimbursement for care of patients

In addition, costs for technical tests such as computer tomography, nuclear magnetic resonance imaging, long-term ECG and others (€1777), physiotherapy, massage and manual therapy (€4914), alternative practitioner and osteopath (€2470) and acupuncture (€2261) were calculated.
The total costs for inpatient treatment were €1505 for admission to the Department of Neurology, €20,349 for the neurosurgery procedure of bilateral occipital nerve stimulation and for inpatient rehabilitation €156 per day. Hospitalisation for headache treatment amounted to €24,086. Rehabilitation amounted to €18,556.
Two patients suffering from refractory CH were treated by occipital nerve stimulation within the period of the study (19). The costs of surgery and hospitalisation were €40,578.
Indirect costs for all participants in the 6-month period
Twenty-four (13.4%) patients were severely handicapped (23 patients 100%, one patient 50%) during the observation period (cCH: n = 16, eCH: n = 8). Based on a daily loss of €95, a total of €160,740 results for all the patients concerned. Moreover, 34 patients indicated having been unable to work for a few days/weeks, resulting in €58,672 for all participants. On average patients were absent from work due to illness for 8.5 days.
Total costs

cCH: chronic cluster headache; eCH: episodic cluster headache.
Additional results
The total score in the HIT was on average 56.68 ± 8.81 (range 41–78), for cCH on average 61.78 ± 8.05 (45–76), for eCH on average 53.25 ± 7.57 (41–78) for all participants.
There was no significant correlation between number of attacks per day and burden of disease measured by HIT-6. cCH patients had significantly higher scores in the HIT-6 than eCH patients (t =−7.288; p < 0.001).
A significant correlation was found between the total score of the HIT-6 and direct costs (r = 0.293, p < 0.001) and between the total score in the HIT-6 and number of attacks in the 6-month period (r = 0.467, p < 0.001).
Furthermore, a significant correlation was found between number of attacks in the 6-month period and the direct costs (r = 0.467, p < 0.001).
Forty-two patients (24%) had been officially classified as severely handicapped due to CH (eCH 12 patients; cCH 30 patients). The average degree was 40.2% for CH. The median degree is 30% in eCH patients and 50% in cCH patients.
Discussion
There are only very limited published data on economic consequences of CH. In our study direct and indirect costs in CH patients were high, with significantly more expenses for patients suffering from cCH.
Direct costs were predominantly a result of the expenses for attack treatment with triptans (especially when used as subcutaneous injections) and oxygen for attack treatment. In our study, most of the expenditure was caused by costs for triptans (75%), followed by oxygen (4.5%). In comparison with this, costs of prophylaxis were much lower (verapamil 1.7%, topiramat 0.01%, others < 0.01%). The overall expenses for acute treatment per capita were €3880 compared to €220 for prophylaxis within the 6-month period. This is in line with reported long-term costs of one patient suffering from secondary cCH in Germany over a 10-year period. The individual amounts are composed of costs for drugs and oxygen (89.7%), diagnostics (5.5%) and medical fees (4.8%) (13). During this time, the patient suffered 5447 attacks with overall costs of €47,030, representing 77.5% of all his medical costs during this period (even including other diseases) (13).
Reimbursement of treatment costs of any of the used substances for acute and prophylactic treatment as well as for oxygen in Germany are generally covered by health insurances. For some patients, reimbursement for oxygen is granted only after extensive discussions with the insurance company; but in the end, all patients receive reimbursement.
This is different from other countries. A recently published US-American trial on the use of oxygen for acute treatment of CH revealed that the costs were covered by their medical insurance for only 64% of oxygen users; 61% of CH patients stated that obtaining reimbursement was not difficult, while 7% stated it was very difficult. Total costs for oxygen were estimated at less than $1000 in 65% of the patients, in 31% between $1000 and $6000 and in 2.5% between $8000 and $12000 per year. Out-of-pocket costs covered by the patients themselves were less than $1000 in 87%, while 13% spent between $1000 and $12,000 (20). Comparing with our data, most of our participants had total costs for oxygen under $1000 per 6 months. Average costs were €416 (=$600). Only 5.6% of all participants had costs above $1000. In the US survey, use of non-medical oxygen, which is much cheaper, is reported in 12% of patients. Reasons for this are lower costs (stated by 66% of the patients), inability to go to the doctor to get a prescription (22%) and physician’s unwillingness to prescribe (18%). Since the question was not asked in our study, we have no comparable data.
Effective prophylactic medication that results in a 50% or more reduction in attack frequency may reduce the total costs enormously. However, a prospective trial or a matched-pairs analysis is necessary to prove this assumption. In terms of treatment costs, CH is a very expensive disease even if it is not a frequent headache disorder.
Only a few patients were treated as inpatients (6.2%), which might be a higher portion of patients in a population not treated in a specialist headache centre. Costs for patients suffering from refractory CH were similar to costs reported in other studies. An Italian headache centre reported direct costs of hypothalamic stimulation of about €27,000 per patient (14), whereas costs of bilateral occipital nerve stimulation were calculated at about €20,000 in our study.
To the best of our knowledge, no detailed cost analysis of other headache disorders is available from Germany. To demonstrate the dimension of costs per capita of eCH and cCH, a comparison with healthcare costs of multiple sclerosis in Germany was performed. Estimated direct healthcare costs were €17,165, direct non-medical costs €5922 and costs due to productivity losses €16,911, resulting in total mean annual costs per patient of €39,998 (21)
A recently published internet-based survey on costs of migraine in the US and Canada revealed $1036 within 3 months for chronic and $383 for episodic migraine in the US and $471 and $172 respectively in Canada (23). Even considering that direct comparison of healthcare costs between different countries is limited to different local statutory requirements, costs of CH are higher than expenditures for migraine care. Twenty-four patients (13.4%) were severely handicapped. Incapacity to work or early retirement was reported in 34 (19%) of the patients in our cohort within the 6-month period, whereas the Danish study reported early retirement in 8% and work absences during 1 year in 29.6% (12).
With approximately 5600 to 95,200 affected individuals and the assumption that 10% suffer from cCH and 90% from eCH, between M€14 and 242 would accrue in cumulative costs for treatment of CH in Germany alone. Consistent with the episodic character of CH, not every patient suffers active periods every year. Moreover, we used the worst value for each item in our study, which results in slightly higher values for several items (like attack frequency). The absolute costs in Germany might actually be lower than those calculated in our study. In addition, due to misdiagnosis and under-diagnosis of CH, many patients will not have been treated (24). On the other hand, many patients may receive inadequate treatment in several disciplines, resulting in high expenses. Costs for unnecessary technical investigations (imaging), visits to the dentist and others do not accrue at a tertiary centre.
Treatment costs from the societal perspective are the focus of our study. From the patients’ perspective, the burden of disease, pain intensity and attack frequency are the main topics. High burden of disease, especially in chronic patients, results in long-lasting impairment, social dysfunction, reduced quality of life and psychiatric co-morbidity. A recent study revealed invalidity in 25% of cCH patients due to CH. Depressive symptoms (56%), signs of agoraphobia (33%) and suicidal tendencies (25%) were frequently reported (11). In this study, 11.2% (12 patients) of the eCH and 41.7% (30 patients) of cCH patients were severely handicapped (as defined by law).
Our study indicates that the HIT is a suboptimal test for estimating the burden of disease in CH. HIT-6 scores did not correlate significantly with attacks per day, which might be the most objective factor of a patient’s restriction in daily life. This could be caused by the last three questions in HIT-6 based on the previous 4 weeks. Patients suffering from eCH who were out of bout in the previous month before the interview rated lowest possible scores, while patients suffering from cCH or eCH patients who were in bout were more likely to choose the highest given scores. That does not indicate less restriction in life during bouts with an attack frequency of up to eight times per day. Therefore the total score of the HIT-6 is not a good predictor. Looking at costs, the number of attacks in the 6-month period has a much better predictive value than the HIT-6. It might have been better to use the Headache Disability Inventory because it refers to an unspecified period in the past (25).
Methodological considerations
There are several limitations to this study. All patients in our survey were treated in a tertiary headache centre. Therefore, the proportion of cCH patients is much higher in our cohort (eCH 60%: 40% cCH) than expected from population-based studies, which showed cCH in 10–20% (26). This is a selection bias resulting from recruiting patients in a tertiary centre. Allowing for a higher proportion of cCH patients in a tertiary headache centre may result in more patients refractory to treatment. There is no generally accepted definition of ‘refractory cluster headache’; suggestions made in the literature refer to a minimum number of medications, but do not specify the dose (27). Two patients within the study were refractory to treatment and consented to being treated with bilateral occipital nerve stimulation. Unfortunately, detailed analysis of additional refractory patients was not done. One can speculate that refractory patients need more (and more expensive) attack treatment (especially sumatriptan s.c.) and are more permanently disabled compared to others. However, age and gender distribution of our cohort represents a typical CH cohort compared to literature and our study population may therefore be comparable to other clinical populations (28). A further limitation of this survey is the retrospective character of the study – but over a 6-month period, data might be reliable. However, quality of data could be improved in further studies, by using prospective headache and treatment diaries.
Major advantages of this study are the high validity of the headache diagnosis, which strictly followed the ICHD-II, and the validity of the detailed analyses of direct and indirect costs.
We conclude that patients with CH are severely impaired regarding the frequency of attacks and cause a high economic burden. Thus, cCH in particular warrants special medical and further supportive care to reduce the burden of disease as well as direct and indirect treatment costs. From the medical and the socioeconomic point of view headache centres taking care of a higher number of patients may reduce impairment and economic consequences of the devastating pain disease CH. Future studies are needed to substantiate this assumption.
Footnotes
Conflict of interest
The authors declare that there is no external funding and no conflict of interest regarding the contents of this manuscript.