
Abstract
Background
Isolated middle cerebral artery dissection is uncommon and occurs in patients reporting headaches as the only symptom. This makes intracranial artery dissection challenging to diagnose and treat.
Case description: We describe two cases of positional headache caused by isolated middle cerebral artery dissection, confirmed using high-resolution magnetic resonance imaging. The two patients presented with sudden-onset headache, occurring when lying in the lateral decubitus position. When lying down in the decubitus position ipsilateral to the intracranial artery dissection, the headache aggravated and middle cerebral artery flow velocity increased on transcranial Doppler ultrasonography compared to when in the supine position. Both patients were treated with antiplatelet agents, and the headache completely resolved within 1–2 weeks.
Conclusion
We recommend additional imaging studies evaluating intracranial artery dissection as a cause of positional headache.
Keywords
Introduction
Middle cerebral artery (MCA) dissection is an uncommon cause of stroke and less frequent than dissection of vessels in the vertebrobasilar system or carotid artery (1). However, MCA dissection, once considered infrequent, is increasingly recognized as a significant clinical entity, particularly in young and middle-aged individuals, and accounts for 4% of all spontaneous cervicocephalic arterial dissections in Japan (2), with a recent systematic literature review reporting 61 cases of MCA dissection from January 1966 to July 2013 (3).
The headache attributed to intracranial artery dissections is mostly unilateral, localized ipsilateral to the dissected vessel, and generally exhibits sudden (even thunderclap) onset and severe intensity (4). MCA dissection is not easy to diagnose, and effective therapeutic approaches to managing intracranial artery dissection remain challenging. Furthermore, MCA dissection may be present in patients reporting headache as the sole symptom, without known trauma. We report two cases of headache that changed according to the head posture, which resulted from MCA dissection.
Case reports
Case 1
A 52-year-old man presented with a sudden-onset headache lasting 1 week in August 2017. He was generally healthy with no specific underlying disease but was diagnosed with tension-type headaches, which manifested in two episodes occurring 4 years and 1 year ago. At that time, he had been taking nonsteroidal anti-inflammatory drugs. He reported no recent headaches. A week before presentation, he experienced pulsatile and tightness pain in the right parietal and temporal lobes when lying in the right decubitus position. Pain was significantly relieved or disappeared completely in the supine position or when lying in the left decubitus position. He had no recent history of trauma and had not started any new medications. At the time of the visit, his blood pressure was 148/93 mmHg, pulse was 75 beats per minute, body temperature was 36.4°C, and respiratory rate was 20 breaths per minute. Physical and neurological examinations revealed no specific findings. While the pain intensity was mild to moderate, magnetic resonance imaging (MRI) was performed for possible secondary headaches with a positional headache limited to the right side. Acute cerebral infarction or cerebral hemorrhage was not observed on MRI (Figure 1(a)). However, contrast-enhanced MR angiography (MRA) showed localized irregular stenosis and enlargement at the end of the M1 segment of the right MCA. Other cerebral arteries, including internal and external carotid arteries, were normal (Figure 1(b)). High-resolution MRI (HRMRI) was performed to accurately assess the cerebral artery inner wall and evaluate the possibility of MCA dissection. Conventional brain MRI and 3D time-of-flight (TOF) MRA were performed using a 3-T MR scanner (MAGNETOM Skyra, Siemens, Germany). TOF MRA was performed using the following parameters: Slice thickness = 0.5 mm, repetition time/echo time (TR/TE) = 23/4.16 ms, flip angle = 16°, field of view (FOV) = 230 × 186.3 mm, and matrix size = 448 × 253. The HRMRI protocol at our institution involved 3D proton-density imaging with turbo spin-echo sequences using the following parameters: TR/TE = 2450/37 ms, FOV = 100 × 100 mm, and matrix size = 195 × 256. T1-weighted imaging and T1-enhanced imaging with turbo spin-echo sequences were performed using the following parameters: TR/TE = 670/9.1 ms, FOV = 100 ×100 mm, and matrix size = 282 × 256. HRMRI images were independently assessed by two neurologists and one radiologist blinded to patient’s clinical data, and discrepancies were resolved via consensus at a group meeting. Although there was no intimal flap in the right MCA at the location of local narrowing and dilatation, pathognomonic radiological findings, such as a crescent-shaped intramural hematoma displaying an eccentric signal void surrounded by semilunar hyperintensity, were observed on T1-weighted HRMRI (Figure 1(c)). We performed transcranial Doppler ultrasonography (TCD) to evaluate the arterial blood flow. When the patient was lying in the right decubitus position, the right MCA velocity was higher than that measured in the supine position (Figure 2). Furthermore, headache was aggravated in the right decubitus position. The patient was treated with 100 mg of aspirin daily, and his headache resolved within 2 weeks. After maintaining the antiplatelet treatment for 3 months, no recurrence of headache was reported and a follow-up HRMRI was performed, which revealed that dissection completely resolved and previously observed vessel stenosis and intramural hematoma were not detected. Thereafter, antiplatelet administration was discontinued.
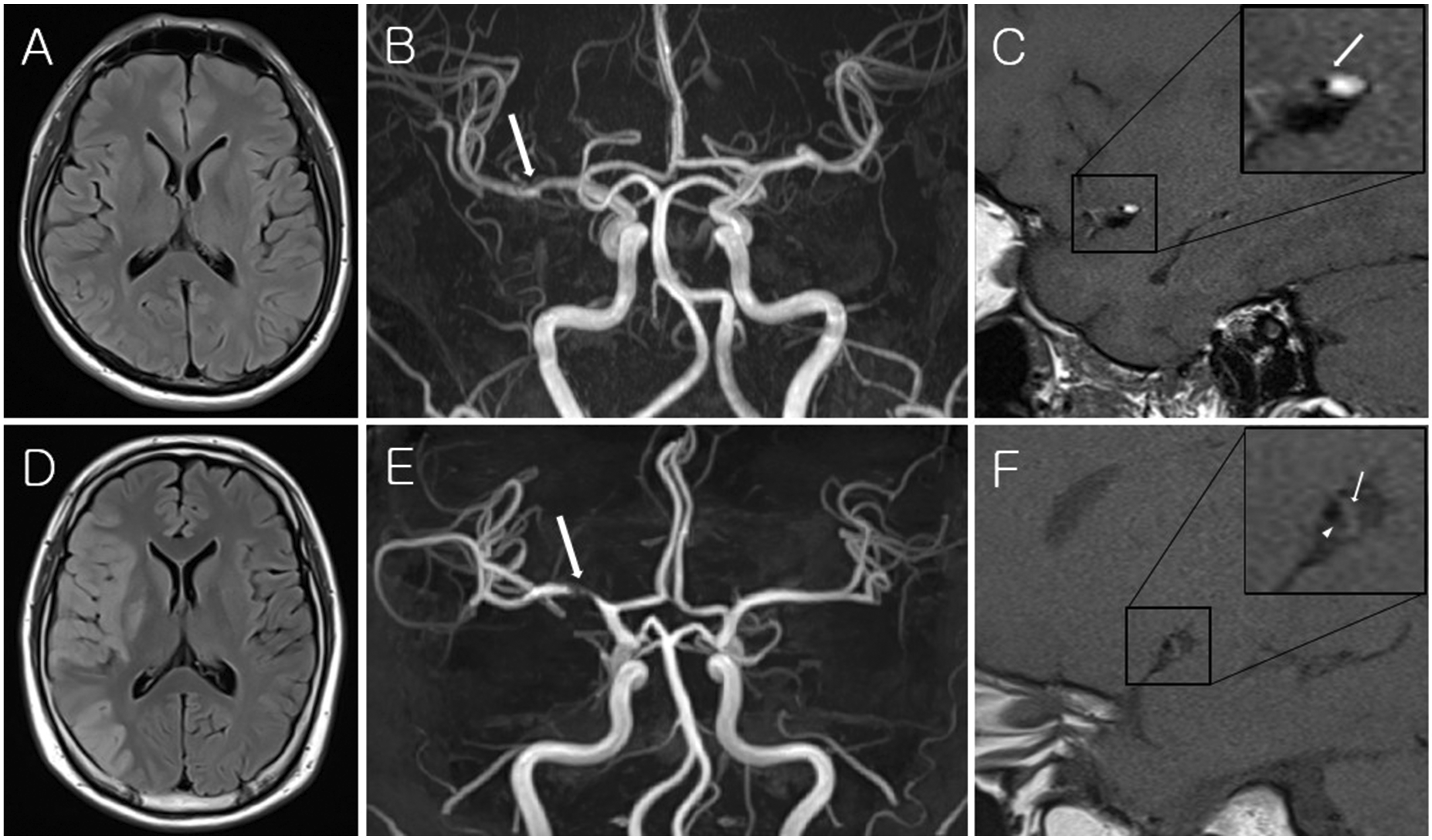
Radiographic images of Patient 1 ((a), (b), (c)). (a) Axial fluid-attenuated inversion recovery (FLAIR) imaging showed no hemorrhagic or ischemic stroke. (b) Magnetic resonance angiography (MRA) showed focal irregular stenosis of the right M1 segment (arrow). (c) T1-weighted high-resolution magnetic resonance imaging (HRMRI) revealed a high signal in an intramural hematoma (arrow), with the narrowed true lumen located in front of an intramural hematoma. Radiographic images of Patient 2 ((d), (e), (f)). (d) Axial FLAIR imaging revealed multiple infarctions in the right MCA territory and basal ganglia. (e) MRA revealed severe stenosis at the mid-portion of the M1 segment (arrow). (f) T1-weighted HRMRI showed a crescent-shaped intramural hematoma (arrow), intimal flap (arrowhead), and a double lumen.

Representative transcranial Doppler spectra with a velocity and intensity scale. The mean blood flow velocity measured in Patient 1 was 94 cm/s and 115 cm/s with the patient positioned in the right decubitus lying position and supine position, respectively. The mean blood flow velocity measured in Patient 2 was 190 cm/s and 207 cm/s in the right decubitus lying position and supine position, respectively.
Case 2
A previously healthy 31-year-old man with a history of cigarette smoking and heavy alcohol consumption presented to the emergency department with left-sided hemiparesis and headache in November 2019. He had no history of trauma, hypertension, dyslipidemia, diabetes, or other lifestyle-related diseases. On admission, blood pressure was 177/86 mmHg, pulse was 86 beats per minute, body temperature was 36.0°C, and respiratory rate was 16 breaths per minute. He displayed serious neurological symptoms, assessed as a National Institutes of Health Stroke Scale (NIHSS) score of 8. The headache was a pulsatile pain in the right parietal and temporal lobe when lying in the right decubitus position. Pain was significantly relieved or disappeared in the supine position or when lying in the left decubitus position. Brain MRI (DWI, fluid-attenuated inversion recovery, T2) showed multiple infarction in the right MCA territory and basal ganglia. Contrast-enhanced MRA showed severe stenosis at the mid-portion of the M1 segment of the right MCA. HRMRI was performed to evaluate the MCA lesion. Scans were performed as per the HRMRI protocol at our institution, as described above. Proton-density sequences showed the presence of an intimal flap with an eccentric tapered pseudolumen in the MCA, and a crescent-shaped intramural hematoma was observed on T1-weighted images. Intimal flap and pseudolumen were also revealed on MRA source imaging in the stenotic right MCA. TCD was subsequently performed. When lying in the right decubitus position, the right MCA velocity was elevated compared to that in the supine position, and the headache simultaneously aggravated (Figure 2). The patient was prescribed 75 mg clopidogrel and 100 mg aspirin daily, and the headache completely disappeared within 1 week after symptom onset. Following 3 months of continuous antiplatelet treatment, the headache did not recur and neurological examination showed improvement, with an NIHSS score of 2 and modified Rankin Scale score of 2. Follow-up HRMRI performed after 3 months of treatment showed no additional infarctions and an improvement in the intimal flap but still exhibited stenosis and intramural hematoma. Antiplatelet agent treatment was, therefore, continued.
Discussion
Symptoms of arterial dissection, in the descending order of frequency, are headache (44.3%), convulsions (6.6%), nausea/vomiting (4.9%), and tinnitus (1.6%) and absence of any neurological deficits associated with stroke was reported in 19.7% of patients (3). According to the International Classification of Headache Disorders 3rd edition, beta version (ICHD-3 beta), the headache pattern caused by intracranial artery dissection manifests as an acute or thunderclap headache, with the pain appearing unilaterally on the side of the lesion (4).
The patient presented to our hospital complaining of headache with or without neurological symptoms; the headache was characteristic of a postural change headache that occurs only when lying on the side ipsilateral to the region of the dissected vessels. Lying lateral (lateral decubitus) to the ipsilateral region of the detached blood vessels means lying in the direction of gravity, which may be related to changes in the volume and velocity of blood flow due to the effects of gravity. In previous studies, changes in cerebral blood flow were susceptible to the effects of gravity. Blood volumes decreased significantly when the direction of blood flow relative to the direction of gravity was reversed or the effect of gravity was increased (5,6). Thus, when the blood flow is opposite to gravity, the volume and velocity of cerebral blood flow decrease, and when it is parallel with gravity, these increase. Therefore, when the dissected blood vessels are aligned in the same direction as gravity, rising cerebral blood flow increases the cerebral perfusion pressure, which temporarily dilates the cerebrovascular vessels and exacerbates pain in the dissected vessels (7). Although headache is a common feature occurring during dissection, little is known about the phenotype and long-term outcomes of headaches associated with vascular dissection (8). Headaches or neck pains can be caused by direct tearing of the blood vessel walls. Arteries have many nerves surrounding them, and stimulating the vessel wall can initiate a cascade of events, including pro-inflammatory neurotransmitter release at the nerve endings surrounding the blood vessels (8). There is controversy over the direct causes of headaches resulting from arterial dissection and causes of vascular headaches in general.
Our study has some limitations. Our reports include only two patients with intracranial artery dissection and represent cases rarely encountered in the clinic. Therefore, generalizing our results may be challenging. Previous studies on headaches caused by dissection analyzed neurological signs and symptoms and the location and intensity of headache (4,8,9), however this important case study showed that headaches attributed to intracranial artery dissection may be characterized by triggering or relief dependent on specific posture.
We described two patients with sudden-onset headache occurring only when lying in the lateral decubitus position in the side ipsilateral with MCA dissection. We recommend additional imaging studies, such as HRMRI, to evaluate vascular dissection as a cause of postural headache.
Patient consent
Written informed patient consent was obtained.
Clinical implications
Middle cerebral artery dissection may induce sudden onset of headache only when lying in the lateral decubitus position. Additional imaging studies in consideration of intracranial artery dissection as a cause of positional headache are needed. When the dissected vessels are aligned in the same direction as gravity, rising cerebral blood flow may dilate the vessels and exacerbate pain.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Sang-Hun Lee was supported by the Seoul R&D program (BT190099) funded by the Seoul Business Agency (SBA, Korea).