
Abstract
Background
Retinal migraine is an important differential diagnosis of recurrent transient monocular blindness accompanied by headache when other etiologies are excluded. Here, we report a case of orbital vasculitis which initially mimicked retinal migraine.
Case report
A 47-year-old woman had recurrent episodes of fully reversible transient monocular blindness accompanied by ipsilateral headache for 15 months. The patient’s neuroimaging and cardiac and ophthalmologic evaluations were normal. With a diagnosis of retinal migraine, her symptoms remitted in response to prophylactic treatment with topiramate and propranolol for 8 months. Three months after discontinuation of medications, transient monocular blindness recurred. High-resolution vessel wall magnetic resonance imaging revealed enhancement of the ipsilateral orbital vessels. Isolated orbital vasculitis was diagnosed. Complete remission of transient monocular blindness was achieved after steroid pulse therapy.
Discussion
Isolated orbital vasculitis should be considered in differential diagnosis of recurrent transient monocular blindness and ipsilateral headache. High-resolution vessel wall magnetic resonance imaging can be helpful for the diagnosis.
Keywords
Introduction
Transient monocular blindness (TMB), also called amaurosis fugax, can be caused by numerous disorders. Differential diagnosis includes vascular, ocular, and optic nerve disorders (1). Any vascular disease that can lead to impaired flow in the ophthalmic artery, central retinal artery, or posterior ciliary arteries, or congestion of the central retinal vein should be investigated. Preliminary workup for TMB should include complete ophthalmologic evaluation, vascular imaging of the anterior intracranial circulation arteries, and/or cardiac evaluation.
For young individuals who have no evidence of vascular or ophthalmologic diseases, retinal migraine is an important differential diagnosis. Retinal migraine is the most likely cause in young patients with recurrent stereotypical TMBs in association with ipsilateral headache, which have been recurring for a long period of time (2). Treatment response to migraine prophylactic agents can be a clue to suspect retinal migraine, when other etiologies are excluded (3). The International Classification of Headache Disorders (ICHD) includes detailed diagnostic criteria for retinal migraine (4). However, as emphasized in the ICHD, retinal migraine remains a diagnosis of exclusion (4). Furthermore, a substantial number of cases with permanent visual loss in patients with retinal migraine has been reported more frequently than cases of migrainous infarction in those with migraine with typical aura (3). Therefore, a thorough investigation of hidden etiologies should be performed before a diagnosis of retinal migraine is made.
Here we report a case of chronic recurrent TMB and ipsilateral headache which initially responded to migraine prophylactic agents but was finally diagnosed as isolated orbital vasculitis.
Case description
A 47-year-old woman began to have recurrent TMB in the left eye. Small patchy areas of blurred vision appeared and increased in number, progressing to total blindness of the left eye within less than a minute (Figure 1). Non-throbbing headache in the left temporal area accompanied the visual symptom. The patient reported phosphenes associated with TMB. Each TMB usually lasted for 1–5 minutes but sometimes continued for up to 20 minutes. Visual acuity and visual field returned to normal between attacks. TMBs occurred three to eight times every day. Other neurologic abnormalities such as motor weakness, sensory abnormality or dysarthria never accompanied TMB. Any of binocular visual, sensory, or language symptoms suggestive of typical migrainous aura were not present. Neither conjunctival injection nor lacrimation was present.
(a) A summary of the clinical course in the present case. The lowest point represents normal vision, the highest point represents total blindness, and points between them represent partial visual field defect. Each peak represents a transient monocular blindness (TMB) attack, and the distance between the peaks represents the attack frequency. The frequency of TMBs decreased while the patient was on migraine prophylactic agents (propranolol and topiramate). TMBs recurred after heavy coffee drinking. A persistent visual field defect developed around the time of admission. After steroid pulse and aspirin treatment, TMB attacks ceased and the visual field defect partially improved. Illustrations depicting (b) the initial visual symptom, (c) the residual visual field defect after the heavy coffee drinking, (d) and the visual field defect 6 months after the steroid pulse.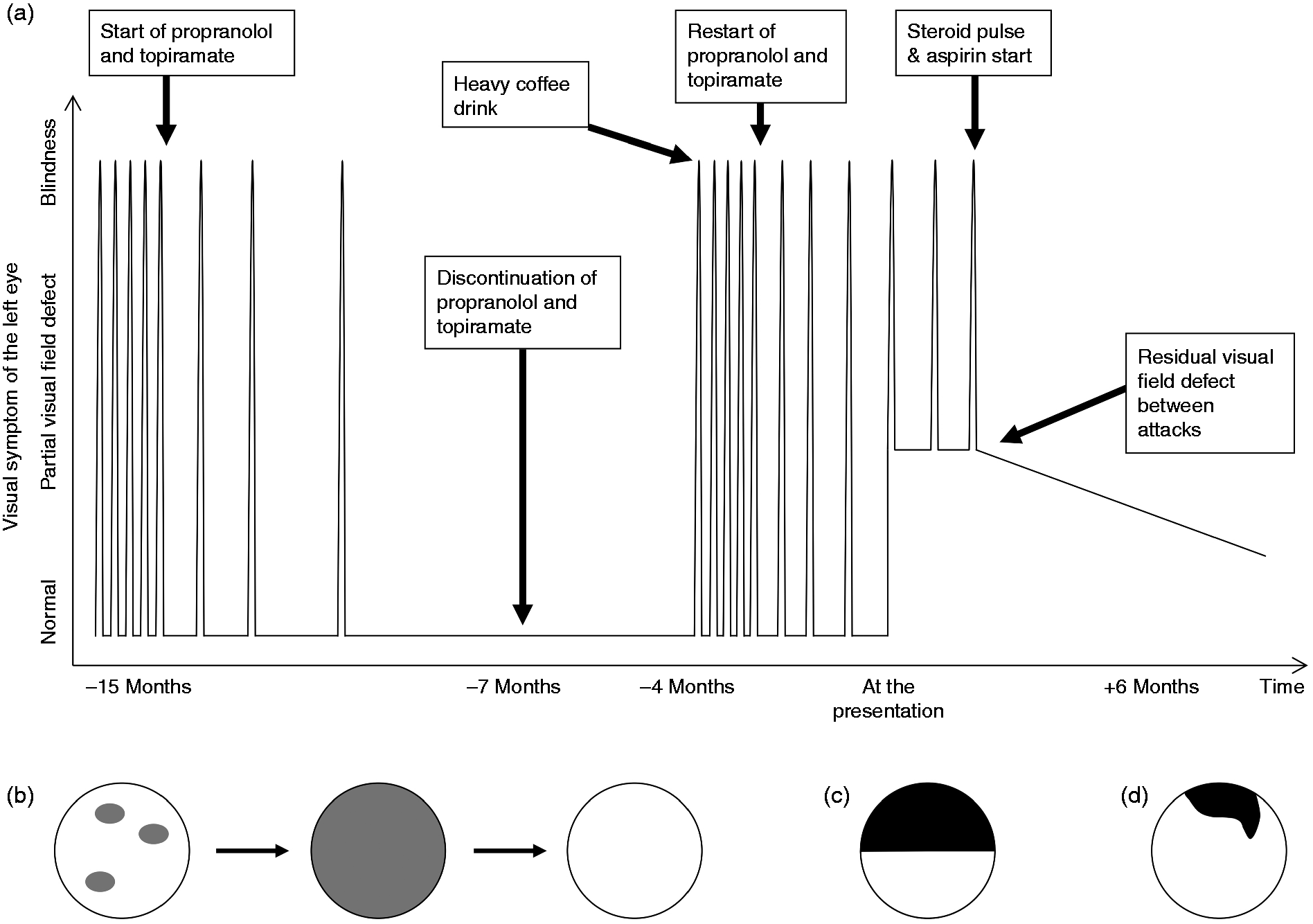
At first, the patient visited a local clinic. Neuroimaging and ophthalmologic and cardiac work-ups were normal. The patient was diagnosed with retinal migraine based on the International Classification of Headache Disorders, 3rd edition, beta version (5). Prophylactic treatment was started with propranolol and topiramate, after which the attack frequency decreased gradually. After achieving a complete remission, medications were maintained for 8 months. The medications were then tapered off. Three months after discontinuation, the patient drank 10 cups of coffee in a day on a coffee gourmet tour. TMBs of the left eye restarted on the same day as the heavy coffee drinking. The attacks then became as frequent as before the treatment. Propranolol and topiramate were started again, which led to a reduction in attack frequency. Four months later, however, the patient reported persistent visual blurring of the left eye between attacks. TMBs still occurred with an increasing frequency. She visited our hospital for a second opinion.
The patient had treated hypertension and dyslipidemia and uterine myomas. General physical examination was unremarkable. Between TMB attacks, best corrected visual acuities (BCVA) were 20/20 in both eyes, pupillary constriction to light was normal, and there was no relative afferent pupillary defect. The bedside fundal examination was normal. During a TMB attack, her BCVA of the left eye decreased to counting fingers at 10 cm and the direct pupillary reflex of the left eye was impaired, while the indirect light reflex was normal. There was a relative afferent pupillary defect in the left eye. Because the TMB resolved during the ophthalmologic examination, a fundal examination could not be performed during the attack.
Routine blood tests were normal, including erythrocyte sedimentation rate and C-reactive protein (7 mm/hr and 0.03 mg/dL respectively). Results of ophthalmologic laboratory tests performed between attacks are as follows: Static perimetry revealed a superior half scotoma in the left eye. There was also an inferotemporal scotoma in both eyes (Figure 2(a)), possibly related to tilted discs that were demonstrated later by fundus photography (6). Color vison, assessed by Hardy-Rand-Rittler test, was 0/10 in the left eye and 10/10 in the right eye. The intraocular pressure was normal at 17 mmHg in the right eye and 16 mmHg in the left eye. The vitreous was quiet. The fundus photography revealed occlusion of the left inferotemporal retinal artery, dilated and tortuous retinal veins, and absence of macular edema in the left eye. It also revealed a tilted disc in both eyes. Spectral-domain OCT (Spectralis; Heidelberg Engineering GmbH, Heidelberg, Germany) (optical coherence tomography) revealed that there was focal thinning of the inferotemporal inner retinal layers in the left eye. Fluorescein angiography (FAG) of the left eye showed an occlusion of the inferotemporal retinal artery (Figure 2(b)), and late phase images showed mild leakage that was attributable to the occlusion.
(a) Initial Humphrey visual field test revealed a superior half scotoma of the left eye and an inferotemporal scotoma in both eyes. (b) Fluorescein angiography of the left eye showed an occlusion of the inferotemporal retinal artery (arrow). (c) Post-treatment visual field test demonstrated an improvement of the superior half scotoma at 6 months after the steroid pulse therapy.
Magnetic resonance angiography (MRA) showed no stenosis or abnormalities in any of the intracranial and extracranial vessels and aortic arch. High-resolution vessel wall MRI of the head was performed. Gadolinium-enhanced T1 black blood image (7) showed enhancement of the left orbital vessels of small caliber and the posterior episclera (Figure 3(a)–(c)). There was no abnormal signal intensity or enhancement of the ipsilateral temporal artery and the optic chiasm in the high-resolution MRIs of the cranial vessels and orbit, respectively. Workups for cardiogenic embolic sources including routine electrocardiography and telemonitoring for 24 hours were unremarkable. Transthoracic echocardiography only showed a suspicious tiny atrial septal defect without hemodynamic significance. Laboratory tests for systemic vasculitides, infection, or autoimmune disorders including the rheumatoid factor, lupus anticoagulant, rapid plasma reagin, anti-nuclear antibody, anti-neutrophil cytoplasmic antibody, antibodies against beta2-glycoprotein I, cardiolipin, or double-strand deoxyribonucleic acid, were negative. With a diagnosis of isolated orbital vasculitis, steroid pulse therapy was started with intravenous methylprednisolone 500 mg per day for three consecutive days. Aspirin 100 mg per day was started at the same time and was maintained thereafter. After the steroid pulse dosage, oral prednisolone of 60 mg/day was given for 7 days and tapered by 10 mg/day per week. TMB did not recur after the steroid pulse dose was given. Follow-up ophthalmological examinations performed at 6 months after steroid pulse therapy revealed an improvement of the visual field defect (Figure 2(c)). Follow-up MRI performed around the same time showed an improvement of the previous lesions (Figure 3(d)).
High-resolution magnetic resonance image findings. ((a), (b)) Axial and (c) coronal gadolinium-enhanced T1 black-blood images showed long-segment vascular enhancements (arrows) in the left (a) proximal and (b) distal orbit. (d) Follow-up image at 6 months after the steroid pulse therapy showed an improvement of the previous vascular enhancements.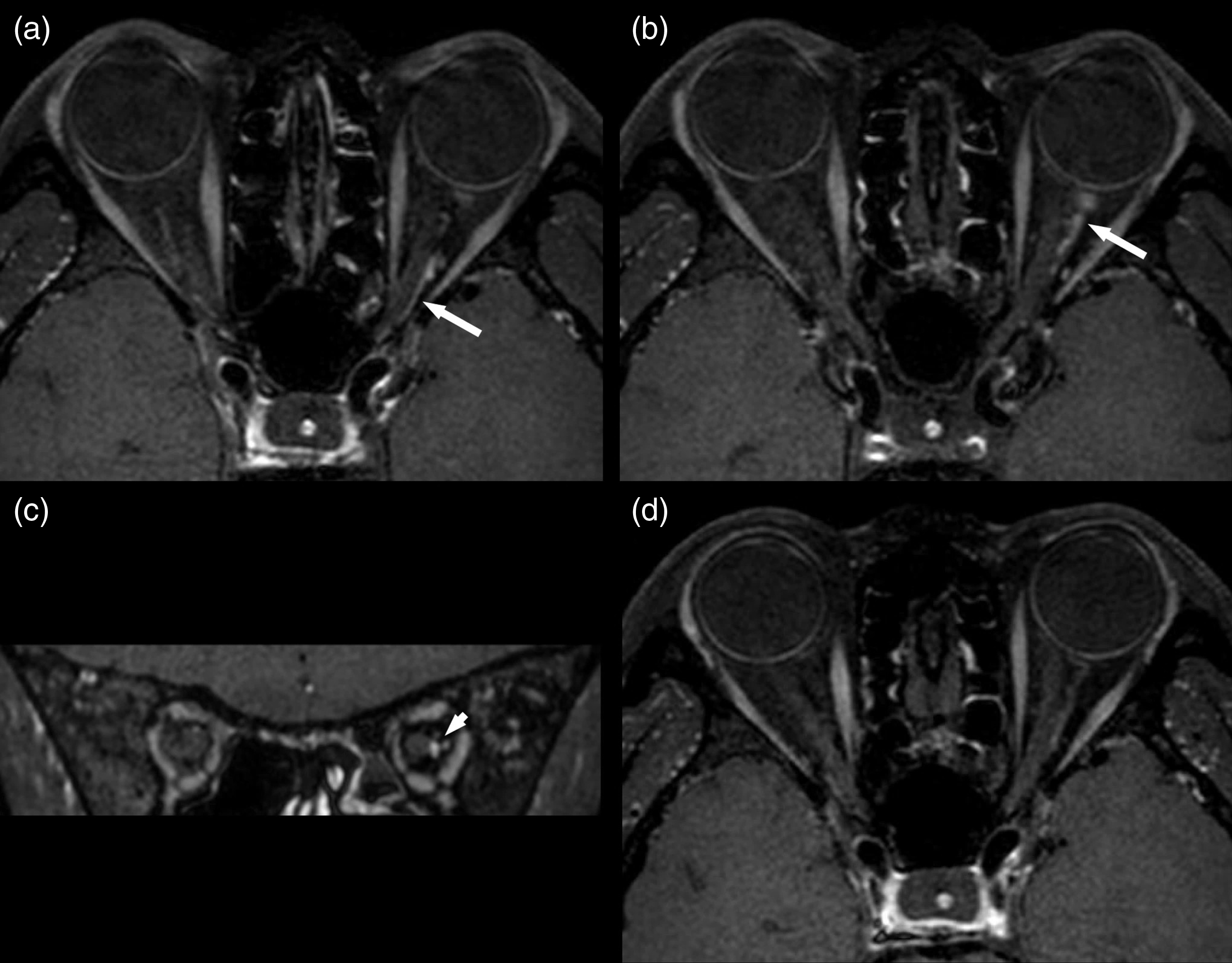
Discussion
In this case report, we describe a patient who had symptoms leading to the suspicion of retinal migraine, and who showed an apparently good treatment response to migraine prophylactic agents, but who finally developed persistent visual disturbance after many months. An advanced neuroimaging technique might be helpful in detecting a hidden secondary cause in a clinical setting suggestive of retinal migraine. In most cases of TMB, ischemia is the leading mechanism (1). Anatomically, disease of the aortic arch (8), the ipsilateral internal carotid artery (9), and the ophthalmic artery and its orbital branches (9,10) can be causes of TMB. However, conventional neuroimaging only visualizes the vessel lumens of medium- and large-sized arteries (7). High-resolution vessel wall MRI provides information on the vascular wall and better-quality identification of arteries with smaller diameters (7). With this technique, we were able to diagnose orbital vasculitis, a rare cause of TMB, in a patient whose symptoms mimicked retinal migraine.
To our best knowledge, this is the first report of an isolated orbital vasculitis with robust neuroimaging evidence in a patient with recurrent TMBs and ipsilateral headache. The diagnosis of orbital vasculitis is supported by the abnormal vascular enhancement and its resolution after corticosteroid therapy. Vascular enhancements can be found not only in vasculitis, but also in conditions such as atherosclerosis, arterial dissection (11), and even an embolic occlusion (12). However, a strong concentric enhancement is most suggestive of vasculitis (13,14). In addition, the stereotypic recurrent TMBs without a stroke or TIA in other vascular territories are not compatible with the manifestation of embolism from large vessels or cardiac sources. Inflammation of an arterial wall can lead to damage of the endothelium, an important barrier for the vascular homeostasis (15). We postulated that endothelial dysfunction was an important mechanism underlying the clinical manifestation. First, endothelial dysfunction results in a predisposition to thrombosis (16). This can lead to microembolism, which may have contributed to the recurrent TMBs. The branch retinal arterial occlusion observed in our case might be a result of a larger embolus produced by the same mechanism. Second, endothelial dysfunction can result in impairment of reactive vasodilation in response to hypoxia (17). Luminal stenosis caused by the vessel wall inflammation, in combination with impaired reactive vasodilation, could efficiently produce hemodynamic insufficiency and lead to the recurrent TMBs. This can also predispose patients to vasospasm (18,19). Taken together, thromboembolism, vasodilatory dysfunction, and vasospasm can be possible mechanisms of the retinal migraine-like symptoms in our patient.
In a recent case of ophthalmic artery vasculitis diagnosed by high-resolution MRI, the lumen and thickened vascular wall was clearly visualized (20). In our case, on the other hand, the lumen was not visualized within the enhancing vascular segment, probably because the caliber was smaller than the ophthalmic artery. Considering that the involved vessel must be upstream of the branch retinal artery, we supposed that the involved vessel might be the central retinal artery rather than the ophthalmic artery. Indeed, occlusion of the central retinal artery can result in a relative afferent pupillary defect, which was present in our case, by making a large retinal defect (21).
Giant cell arteritis was unlikely because of young age at onset, normal level of erythrocyte sedimentation rate and C-reactive protein, and absence of abnormal signal intensity or enhancement of the temporal artery in high-resolution vessel wall MRI. Response to migraine prophylactic agents could be explained in part by the antiplatelet effect of propranolol (22). However, there is a concern about using propranolol because it may cause a paradoxical vasoconstriction (23). Symptom aggravation after intake of a large amount of coffee could be explained by the vasoconstrictive effect of caffeine, which could have aggravated the presumed narrowing of the already inflamed orbital arteries (24).
Clinical implications
Retinal migraine is an important differential diagnosis in patients with recurrent transient monocular blindness (TMB) and headache, but it is still a diagnosis of exclusion. Orbital vasculitis can be a potential cause of recurrent TMBs and ipsilateral headache. High-resolution vessel wall magnetic resonance imaging can be helpful for the differential diagnosis of TMBs.
Consent
Written informed consent was obtained from the patient for the review of her records for this publication.
Footnotes
Authors’ contributions
Ji-Hyung Park contributed to examination and management of the patient, study conception, study design, drafting of the manuscript, and analysis of data. Mi Ji Lee contributed to examination and management of the patient, study conception, study design, drafting of the manuscript, analysis of data, and critical revision of the manuscript for intellectual content. Chin-Sang Chung contributed to examination and management of the patient, study conception, study design, and critical revision of the manuscript for intellectual content. Kyung-Ah Park contributed to the analysis and interpretation of data and revision of the manuscript. Jihoon Cha contributed to the analysis and interpretation of data. Sung Tae Kim contributed to the analysis and interpretation of data.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.