
Abstract
The objectives of the present study were: (i) to estimate the prevalence of recurrent headaches in schoolchildren (ranging from 2nd to 5th degrees) in Mersin city of Turkey; (ii) to determine the sensitivity, specificity, positive predictive value and positive likelihood ratio of the diagnostic headache characteristics in children with migraine and tension-type headache (TTH) using neurologist's diagnosis as the gold standard. The stratified sample of study was composed of 5562 children. The prevalence of recurrent headache was 49.2% (2739 of 5562) and the prevalence of current headache was 31.3% (859 of 2739). TTH was more common than migraine (24.7% vs. 10.4%). The most sensitive headache characteristic for migraine was ‘severity of pain’ and the most sensitive definitive symptom was ‘duration of headache’ in children with TTH. International Headache Society-based symptom definition criteria are highly beneficial in diagnosis of childhood headache, if used together with detailed clinical assessment.
Keywords
Introduction
Headache is a common symptom in paediatric practice (1). There is a high incidence, prevalence, and individual and societal cost of headache disorders in children and adolescents (2). The reported prevalence of headache among schoolchildren varies greatly, from 5.9% to 82%, depending on the definition criteria (3–6). The vast majority of chronic headache is idiopathic in origin and is currently classified as migraine or muscle contraction (‘tension’) headaches (7). Migraine is the most common cause of chronic paroxysmal headaches in children (8). Also, migraine is one of the most common causes of headaches in children and adolescents resulting in missed school days and interfering with other daily activities (2, 9–11).
Childhood headache, especially migraine, has specific characteristics different from adult migraine. For example, abdominal pain is common, and the migraine attacks are often associated with nausea or vomiting. The duration of migraine is shorter in children (11–13). Tension-type headache (TTH) may be difficult to differentiate from migraine in children, as some of the symptoms overlap. International Headache Society (IHS) described the diagnostic criteria of episodic TTH as at least 10 previous headache episodes, with an average headache frequency of <15 days per month (180 days per year) for 6 months (3, 14). There are some epidemiological studies about the reliability of the IHS criteria for the diagnosis of TTH and the demographic characteristics of children with TTH (15–18).
While the development of the IHS criteria is a vital step forward in headache diagnosis, its contribution is in the area of criterion variance. The IHS does little to address the issues of information and interpretation variance. Diagnostic agreement among independent clinicians is often surprisingly poor, and in the field of headache has not been adequately studied (17). Headache diagnosis in children is based on an overall interpretation of clinical symptoms (8). Present and future work should focus on alternative case definitions based on behaviour rather than symptoms (i.e. going to a dark room, squinting, turning off the lights instead of photophobia). Exploring additional or alternative diagnostic features (e.g. pallor, abdominal pain, sensitivity to odours, menstrual exacerbation) may be helpful (14).
The objectives of the present study were (i) to estimate the prevalence of recurrent headaches in schoolchildren (ranging from 2nd to 5th degrees) in Mersin city of Turkey, (ii) to determine the sensitivity, specificity, positive predictive value and positive likelihood ratio of the diagnostic headache characteristics in children with migraine and TTH using neurologist's diagnosis as the gold standard.
Materials and methods
This study was conducted in Mersin located on the Mediterranean coast of Turkey. Its population is 759 785 and it is the 10th largest city in the country. Commercially it is an important harbour city and it is economically well developed. There are 60 170 schoolchildren aged 8–16 years.
Estimation of sample size
A school-based cross-sectional and selective (ranging from 2nd to 5th grades) study was performed. The migraine prevalence of schoolchildren was accepted as 10% (worst acceptable 9–11%). It was estimated that to reach a reliability of 99%, at least 5432 children should be included in the study in order to represent the sample universe.
Selection of subjects
Multi-step, stratified, cluster sampling were used. In the first phase, all schools were classified into three groups according to their socio-economic levels. According to the severity of the classification 23 schools were selected randomly. In the second phase, classes were selected randomly according to the number of students in that particular school. The study population consisted of 5777 students from 23 schools out of 82 schools in the city. This sample represented 9.6% of all schoolchildren aged 8–16 years. The sample size randomization was made with EPI 6 INFO program. Randomization was also weighted according to gender and to each stratum (good, satisfactory, poor) of study population.
Study procedure
Before interviewing the students, a detailed structured questionnaire was submitted to parents and written informed consent was obtained. This form included the demographic features, headache history of the family, and the headache characteristics of the children. A neurologist or public health specialist also recorded the headache history of the children using a structured interview in classroom (a neurologist and public health doctor were matched for each classroom). The interview followed a structured two-part questionnaire. The aim of the first part was to determine the biological and socio-demographic variables, which potentially influence headache. The second part was structured to detect the presence of headache and its characteristics. Questions about the two most common types of headache (migraine and TTH) were designed in such a way as to make a diagnosis according to IHS criteria at predigit level. The observations of the teachers on the behaviour of the child with headache were also documented through an interview. Parent information, teachers’ observations and structured interviews were obtained from 5712 children. During the data quality control process 150 of them were excluded from the study because of missing or unreadable answers.
Diagnosis of headache
Five thousand five hundred and sixty-two children (96.2% of study sample) were evaluated by the same neurologist (A.Ö.) and final diagnosis was made according to IHS criteria, teacher observations, parent questionnaire and clinical assessment. The diagnosis of paediatric migraine was made using IHS-revised criteria (16) and of TTH with IHS criteria (17). According to the frequency of days with headache per month, headache was classified as episodic or chronic TTH. When the diagnosis of the type of headache could not be made definitely, it was classified as ‘unclassified headache’.
The aura is an inconsistent feature in childhood and less reliable heralding phenomenon than in adult migraineurs. According to study design, the presence of aura was not questioned and therefore a distinction between migraine with or without aura was not made.
The severity of headache was determined according to the response that was obtained to the following questions: ‘could you watch your favourite programme on TV during the headache?’, ‘Could you negotiate stairs during the headache?’ or ‘does playing aggravate your headache?’ Children were asked to mark out the location of their pain on the head figures shown in the questionnaires.
Validation of study procedure
In order to validate the study procedure, we performed a preliminary study with 110 children. All these children were evaluated with the same study procedure and the same neurologist, who had no knowledge of the other information about the child, examined children who reported recurrent or current headache. Afterwards, the ratios of sensitivity, specificity, positive predictive value (PPV) and positive likelihood ratio (PLR) were calculated using the neurologist diagnosis as a reference test. These ratios were 94.4%, 55.3% and 67.1%, respectively.
Statistical analysis
Student's t-test was used in order to compare the age of children, age of mother and father between the study groups. For testing the gender, and all other variables of children and parents between the migraine and TTH groups, χ2 test was performed. The education period of the mother and father was tested with Mann–Whitney U-test. Binary logistic regression analysis was used with forward LR variable selection method.
The sensitivity, specificity, PPV and PLR were calculated for each headache characteristic using predefined formulae and the neurologist diagnosis as the gold standard (Table 1). Sensitivity refers to the proportion of patients with these definitive symptoms who met the neurologist diagnosis. Specificity refers to the proportion of patients who did not have these definitive symptoms and who did not meet the neurologist diagnosis. PPV refers to the proportion of patients with the definitive features who actually had the disease. A PLR for headache is the odds of meeting the definitive features of migraine or TTH among those patients with a clinical diagnosis of migraine or TTH compared with the odds of meeting the definitive features of migraine or TTH among those patients without a clinical diagnosis of migraine or TTH. Solomon (18), and Maytal (12) used a similar approach in previous reports. The means were calculated with descriptive statistics. Two-tailed tests were used in this study. The tests were considered as significant at the 5% level.
Sensitivity, specificity, positive predictive value, and positive likelihood ratio for the definitive features of migraine or tension-type headache (TTH) using the neurologist diagnosis as the gold standard
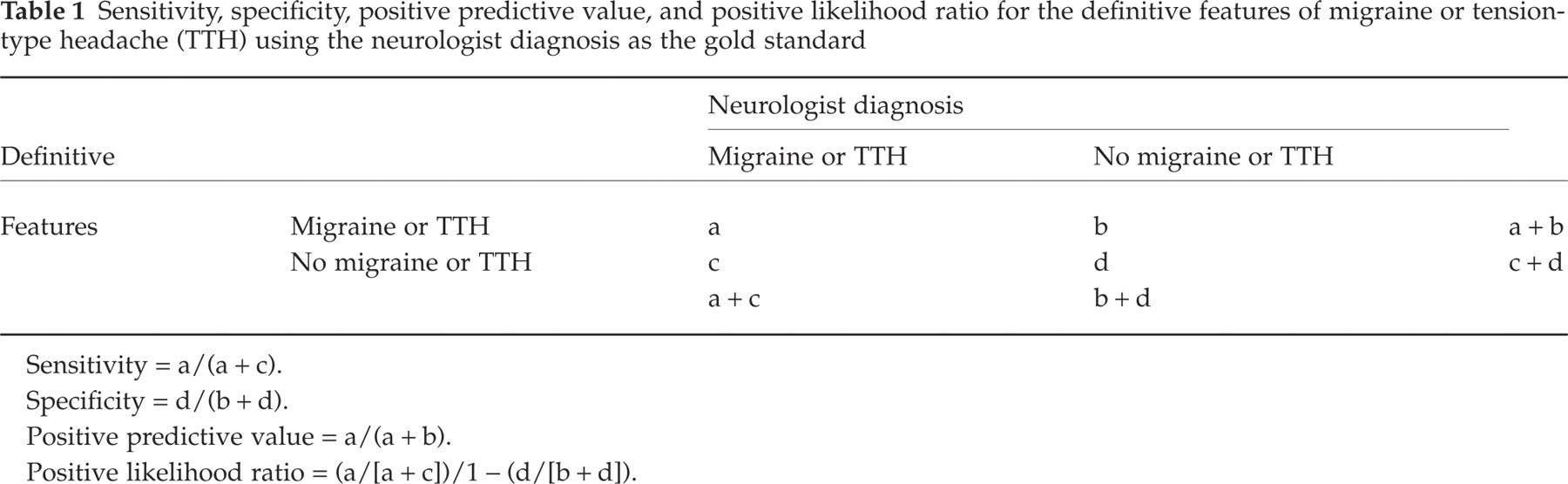
Sensitivity = a/(a + c).
Specificity = d/(b + d).
Positive predictive value = a/(a + b).
Positive likelihood ratio = (a/[a + c])/1 − (d/[b + d]).
Results
Among our final sample of 5562 children, 1949 (35.1%) received the clinical diagnosis of either migraine or TTH. The migraine group consisted of 576 (10.4%) children, of whom 303 (52.6%) were girls and 273 (47.4%) were boys, with their mean age at the time of the study being 10.03 ± 1.36 years. There were 1373 children (24.7%) with TTH. One thousand two hundred and ninety-one (94.1%) had episodic TTH (666 female (51.6%), 625 male (48.4%)) and their average age was 10.1 ± 1.3 years. Eighty-two children (5.9%) had chronic TTH (51 female (62.2%), 31 male (37.8%)) and the average age was 10.04 ± 1.32 years. There was no significant difference for gender between the migraine and TTH groups, or for either of the TTH groups (see Table 2).
The demographic characteristics of migraine and tension-type headache (TTH) children

NS, Not statistically significant difference (P > 0.05).
Figures represented as mean ± SD.
Demographic characteristics
There were significant differences between the groups, for variables such as having a father with headache, and parents being separated (widowed or divorced) or one of them being dead. On the other hand, there were no significant differences between the migraine and TTH groups for the other variables (e.g. being the first child of the family, occupation of the parents, smoking of the parents, and income of the family) (see Table 2).
Nature of headache
The headache characteristics of both groups are summarized in Table 3. The mean duration of headache attacks was significantly longer in children with migraine than in children with TTH (P = 0.000, t =−3.09). On the other hand, the frequency of headache was higher in children with TTH (P = 0.003, t =−3.34). Some of the diagnostic features of headache such as severe pain, throbbing quality, unilateral pain, occurrence of the concurrent symptoms of nausea, vomiting, and phonophobia were significantly different between the groups (Table 3). It is of interest that the symptoms of phonophobia and photophobia, concurrent with headache, were more frequent in children with TTH. A total of 904 children complained of travel sickness, 295 of whom (53.2%) suffered from migraine and 609 from TTH (46.8%). The difference was statistically significant (χ2 = 6.26, d.f. = 1, P = 0.01). The ratios of analgesic consumption for both of the headache groups were fairly high (67.5% vs. 64%).
The headache characteristics of migraine and tension-type headache (TTH) children
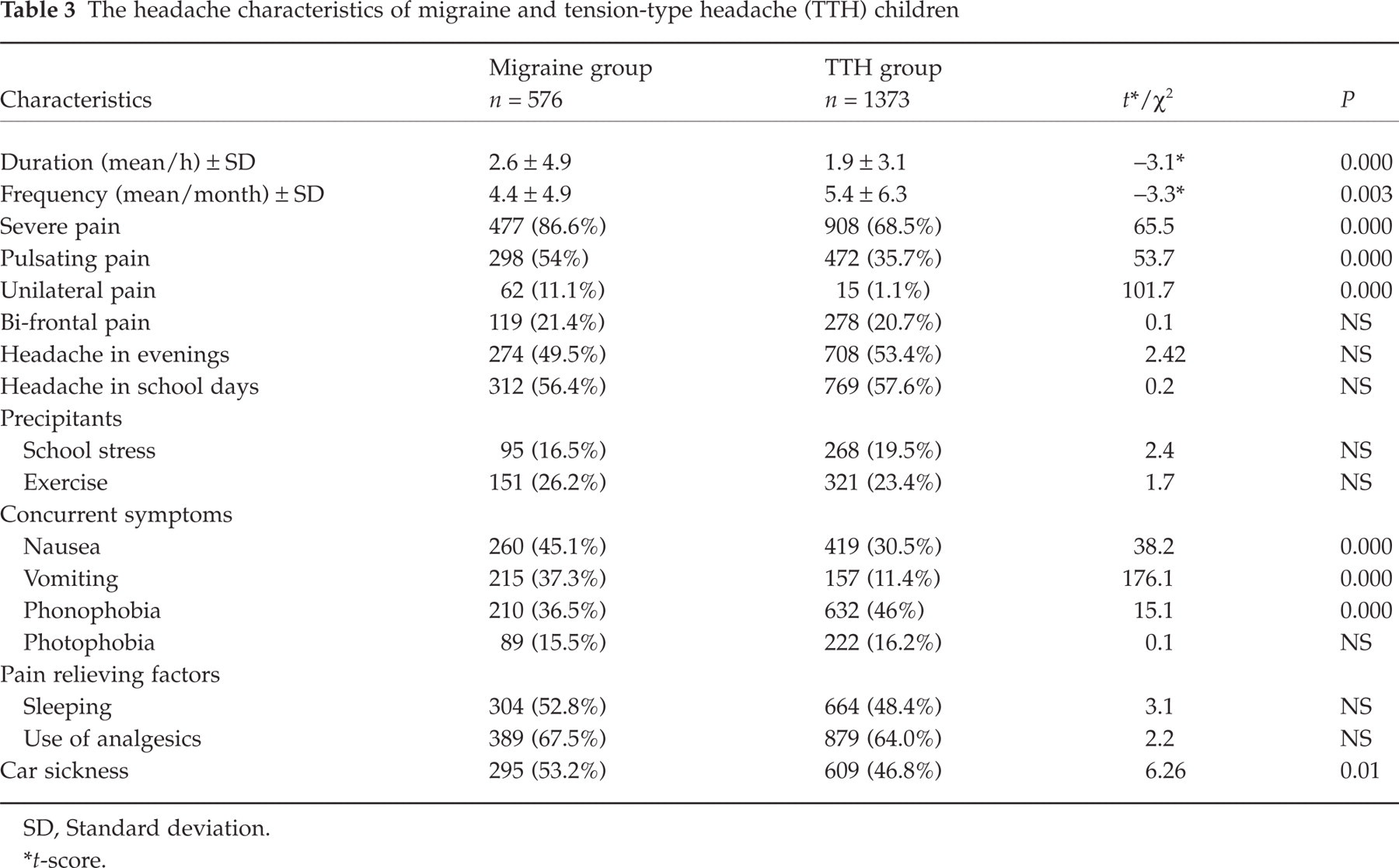
SD, Standard deviation.
∗ t-score.
Validity of headache features
To explore the specific results of the migraine and TTH group, we examined the sensitivity, specificity, PPV and PLR of each diagnostic feature of both groups, using the neurologist diagnosis as the gold standard (Table 4). When examining headache duration, we found that by decreasing headache duration to 1 h from 2 h when diagnosing migraine, the sensitivity increased over two-fold (41.8% vs. 84.1%), with the specificity being 27.9%. As shown in Table 4, severe pain (86.6%), consumption of analgesics for headache (67.5%) and pulsating/throbbing pain (55.2%) were the most sensitive headache characteristics for migraine, whereas unilateral pain (98.6%), vomiting (86.1%) and photophobia (81.9%) accompanying headache were the most specific ones. Unilateral pain had the highest PPV (74.6%) and PLR (8.12) in children with migraine when the neurologist diagnosis was accepted as the gold standard.
Sensitivity, specificity, positive predictive value (PPV) and positive likelihood ratio (PLR) of headache characteristics in children with migraine using the neurologist diagnosis as the gold standard

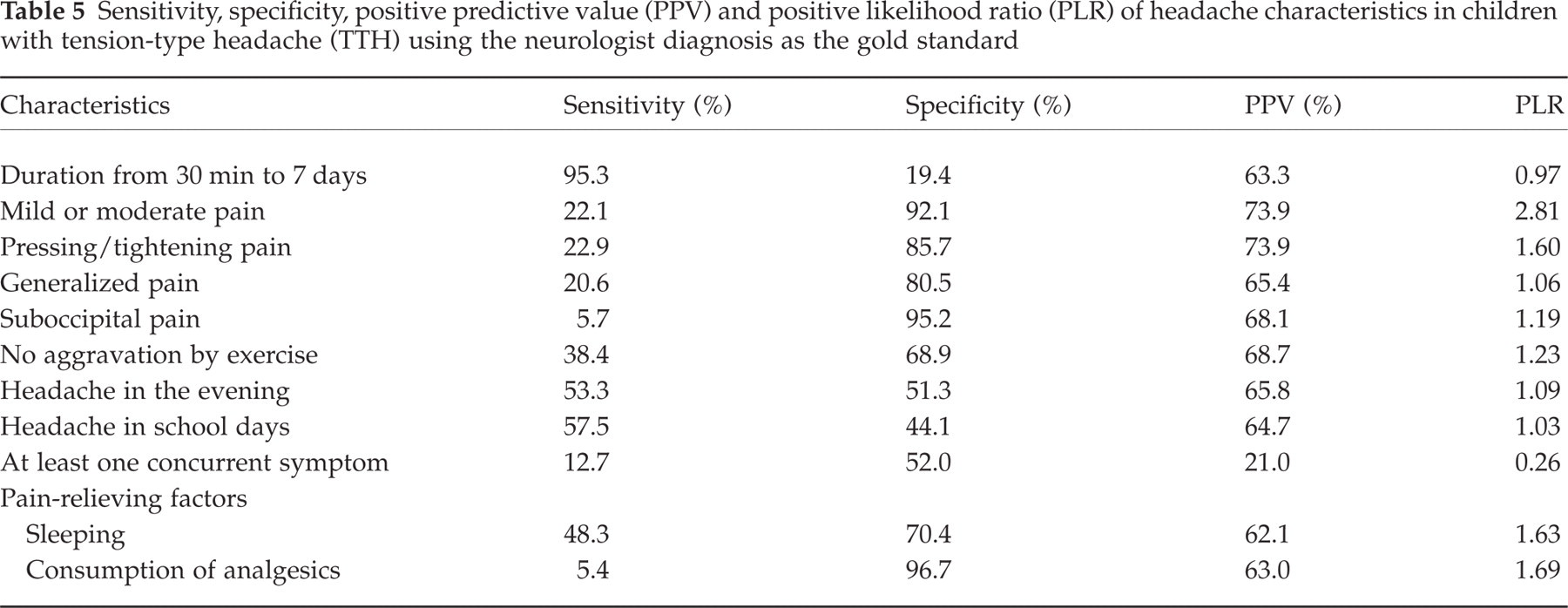
The headache duration is the most sensitive criterion (95.3%) for TTH, with 19.4% specificity and 63.3% PPV. As summarized in Table 5, the diagnostic criteria for TTH have a low sensitivity but high specificity, using neurologist diagnosis as the gold standard. The other sensitive diagnostic criteria were headache only in school days (57.5%), and going to sleep for relief of the headache (48.3%). However, the criteria with a high specificity ratio were: suboccipital localization of pain (95.2%), and a pressing or tightening quality of pain (85.7%). Mild or moderate pain was the most predictive one (73.9%) and had the highest positive likelihood ratio (2.81) in children with TTH.
Sensitivity, specificity, positive predictive value (PPV) and positive likelihood ratio (PLR) of headache characteristics in children with tension-type headache (TTH) using the neurologist diagnosis as the gold standard
Logistic regression analysis revealed that pulsating quality of headache (ExpB: 4.21), aggravation with walking stairs (ExpB: 1.45), not being able to watch television during headache attacks (ExpB: 3.73), having nausea (ExpB: 2.46) or vomiting (ExpB: 7.16) associated with headache attacks and unilateral location of headache (ExpB: 22.62) had significant effects on migraine of schoolchildren. On the other hand, headache frequency (ExpB: 1.05) and recent minor head trauma (ExpB: 1.68) had an important effect on TTH attacks of schoolchildren.
Discussion
The results of the current study indicate that TTH (70.4%) was more frequent than migraine (29.6%) among schoolchildren with headache. Additionally, age, duration of the pain, quality of pain, occurrence of concurrent symptoms, and having travel sickness were closely associated with the type of headache. Also, when the diagnosis was made according to the neurologist's impression, the duration of pain was found to be the most sensitive and the quality of pain the most specific headache characteristics for children who were diagnosed as having either TTH or migraine.
In their comparative study Rasmussen et al. (19) concluded that questionnaires were a weak instrument and preferred the clinical interview for diagnosis. In the current study, although family information was obtained with a questionnaire, a physician obtained headache characteristics of the children through a structured questionnaire that was followed by an interview, and these data were supported by the information obtained from the teacher's observation on the behaviour of the children. To our knowledge, this study design has not been used in the previous reports.
In a study of 7-year-old Finnish schoolchildren, the prevalence of headache was reported to be 37%, which increased to 69% by 14 years of age (20). Our headache prevalence was 49.2%. In a population-based epidemiological study, Metsahonkala and Sillanpaa (13) reported that 36.6% of children aged 8–9 years had headache attacks that interfered with their daily activities during the previous 6 months, but the rate of paroxysmal headache was reported to be 6.1% in that study population. In our study, 10.4% (576/5562) of the children had IHS criteria consistent with migraine and 24.7% (1373/5562) with TTH. To our knowledge, little attention has been given to the prevalence of TTH among children and adolescents, since most epidemiological studies classify headaches as migraine or not (10, 21). The prevalence of TTH was higher in our study population (schoolchildren aged 8–12 years) and consisted of 70.4% of all children with primary paroxysmal headaches. This rate is in accordance with some other reports (10, 19, 22). Most of the children with TTH revealed the characteristics of episodic TTH (94%). Contrary to other reports (9, 23) headache was more common in girls in both of our study groups. This difference may be explained by the design of our study, which was aimed to study both migraine and TTH, whereas most of the epidemiological studies relating to childhood headache are designed to study the prevalence and characteristics of migraine. On the other hand, as our study was not aimed to evaluate the age-dependent variance of headache, we have not looked at the relationship between age and gender for all age groups.
During migraine attacks, half of the affected children cry, 69% report pain intensity to be severe, and 96% withdraw from activities of daily living (5). However, we favoured accepting pain as ‘severe’ when children reported they stopped watching their favourite TV programme during their headache. The response was double-checked by the information obtained from the parents and teacher, and only the matched responses were taken into consideration by the neurologist.
As recommended by Maytal et al.'s report (12), we assessed the sensitivity and specificity of headache characteristics on the IHS-based diagnosis of migraine and TTH with a school-based setting. Over the last three decades, several definitions of paediatric migraine have been proposed (2, 12, 14, 24). Using clinical diagnosis as the gold standard, the most sensitive headache characteristic was the severity of pain (86.6%) in children with migraine and the duration of headache (95.3%) in children with TTH.
In children and adolescents, migraine tends to be of shorter duration. The duration of pain was reported to be <2 h in 11–81% and <1 h in 8–25% in several studies (12, 17, 25–27). In the majority of children (82%)>8 years of age the attacks were reported to last <24 h (25). However, the mean duration of headache was found to be significantly longer in children with migraine (the average duration was 2.6 h, ranging from 1 h to 48 h) than in children with TTH (the average duration was 1.9 h, ranging from 30 min to 72 h) in our study. Based on our findings and prior reports (12, 17, 25, 27) we also support the suggestion of decreasing the criterion on the minimal duration of pain to 1 h for migraine headaches in children. Winner et al. (17) reported that the sensitivity of IHS criteria can be increased from 50% to 73% when the duration of pain is decreased to a minimum of 1 h in children under the age of 12 years. Similarly, Metsahonkala (13) reported that when duration was omitted as a criterion (minimum 1 h), the prevalence increased from 2.7% to 3.5% (a 25.9% increase). In the current study, when the duration of headache was decreased to 1 h, the sensitivity of headache duration increased from 41.8% to 84.1% with the 27.9% specificity, and the PPV of 29.6 in children with migraine.
Unilateral pain has been challenged as a diagnostic criterion because it is more characteristic of adult migraine than of paediatric migraine (4, 17, 26, 27). Metsahonkala and Sillanpaa reported unilateral pain in 67% of their children with migraine (13), but Gallai et al. found that this rate was 41.5% in children diagnosed by IHS criteria (26). Maytal et al. (12) found that unilateral pain had a sensitivity of 34% and a specificity of 86% using clinical diagnosis as the gold standard. Among our children with migraine only 11.1% had unilateral pain, with the sensitivity being 11.1%, specificity 98.6%, with a high PPV for migraine (74.6%) and also a high PLR (8, 12). On the other hand, only 1.1% of children with TTH had unilateral pain. Although we found that the unilateral pain was not a common finding in children with migraine, overall our results are in accordance with the conclusion of Maytal et al., who suggest that unilateral pain should remain a migraine-defining feature in children (12).
Pain intensity and quality are sometimes difficult to ascertain in paediatric patients. Mortimer et al. (25) reported that headache was described as throbbing in 86% of children with migraine aged 8–11 years. Additionally, 28% of these children reported bi-frontal headache. In a series of studies, throbbing or pulsating pain had a sensitivity of 36–86% (4, 12, 13, 26, 28). These ratios were 53.9% and 63.2% for sensitivity and specificity, respectively, in our children with migraine. Likewise, pressing or tightening pain has a low sensitivity (22.7%) but a high specificity (94.7%) and PPV (79.4%) in children with TTH. Also, the sensitivity of moderate to severe intensity in migraine ranged from 57.8% to 97.1% in various studies (12, 26). Mortimer et al. (25) reported that 44% of those children aged 8–11 years cried with pain during an attack and all of them had lost time from school due to migraine. In our study, 86.6% of children with migraine and 68.5% of children with TTH had severe pain, resulting in lost time from school or daily activities. However, most headache specialists accepted the concept that primary headache is a spectrum, where migraine is at one extreme and pure TTH is at the other, with most patients having both at times. Another opinion is they are both the same disease; when it is mild it is TTH, and when its gets bad it is migraine (15). It is a limitation of this study that it could not identify the overlap headache disorders (TTH and migraine). The tendency to sleep after attacks was lower in our group (52.7% in the migraine group and 48.3% in the TTH group) compared with Mortimer et al.'s report (81% of children with migraine) (25). Children with TTH also more frequently (23.6%) reported tenderness in the occipital muscle insertion than children with migraine. Aromaa et al. also reported such an observation previously (3).
Reports of concurrent nausea and vomiting in childhood migraine have varied, ranging from 65.5% to 92% (24, 25). A population-based study reported that the ratios for nausea, vomiting, photophobia, phonophobia and dizziness were 92%, 67%, 84%, 75% and 44%, respectively (25). Occurrence of these headache characteristics had good sensitivity (12, 13, 29). Winner et al. (17) noted that if photophobia or phonophobia, rather than photophobia and phonophobia, were used, sensitivity improved, especially in the subset <12 years of age. Seshia et al. (29) found that in children with headaches, 30% could not describe the quality of their pain and 16% could not report on photophobia and phonophobia. Based on our findings, the most prominent symptoms were nausea (45.1%) in children with migraine and phonophobia (46%) in children with TTH. We conclude that for the IHS-based diagnosis of migraine, nausea and vomiting have poor sensitivity and high specificity in this model. However, having at least one associated symptom has poor sensitivity and specificity for the IHS-based diagnosis of TTH in schoolchildren.
It is unclear whether subjects with migraine are more prone to have travel sickness. Some reports have found a high incidence (e.g. 49.1%) of travel sickness in subjects with migraine (14, 25, 30), while others have not (31). Our prevalences on travel sickness were 53.2% for migraine and 46.8% for TTH, in accordance with earlier reports (24, 25).
Mortimer et al. (25) reported that a migraine precipitant could be identified in 44.4% of the children aged 8–11 years. In contrast to younger age groups (<7 years), stress was a precipitant in 13.9% of the older age group. In children> 8 years, tiredness (8.3%), exercise (2.8%), noise (2.8%), glaring light (2.8%), missing a meal (2.8%), and studying (2.8%) were all reported as migraine precipitants. In our study, school stress and exercise were evaluated as headache precipitants. School stress was found to be a precipitant for migraine in 16.5% and for TTH in 19.5%, and exercises triggered attacks in children at higher rates.
Conclusions from this study are: (i) the prevalence of recurrent headache was 49.2% (2739/5562) and the prevalence of current headache was 31.3% (859/2739) in our study sample; (ii) TTH is more common than migraine (24.7% vs. 10.4%); (iii) the most sensitive headache characteristic for migraine is ‘severity of pain’; (iv) the most sensitive definitive symptom is ‘duration of headache’ in children with TTH; (v) IHS-based symptom definition criteria are highly beneficial in diagnosis of childhood headache, if used together with detailed clinical assessment.