
Abstract
Introduction
Headache is an extremely prevalent disorder with a lifetime prevalence of 90–99%. However, a small fraction of people never experiences a headache. Research on people without headache could uncover protective factors in headache, but to our knowledge no study on headache-free individuals has been published. We aim to estimate the prevalence of headache-free individuals among Danish blood donors, and to describe the socio-demographics and health factors of headache-free participants.
Materials and methods
In all, 38,557 healthy volunteers were recruited as part of the Danish Blood Donor Study. Headache-free participants were identified based on the question “Have you ever experienced a headache of any kind?”. Utilising the Danish registries and self-reported questionnaires, we analysed socio-demographic and lifestyle factors using logistic regression adjusted for age and sex.
Results
The prevalence of headache-free individuals was 4.1% (n = 1362) with a female-male ratio of 1:2.2. To be headache free was significantly associated with an employment status as a student, a low level of income and a regular alcohol consumption.
Discussion
The prevalence of headache-free individuals was comparable to population-wide studies of headache. To be headache free was not associated with a high socio-economic status. Further studies on people without headache will hopefully reveal protective factors in headache, and this novel approach might be useful in other very prevalent disorders.
Introduction
Headache is an extremely common illness that in population surveys has a lifetime prevalence of 90–99% (1–4). Tension-type headache is the second most prevalent disorder in the world followed by migraine, which ranks as the third most prevalent disorder (5). Migraine has a lifetime prevalence of 16–25% and tension-type headache has a lifetime prevalence of 78–89% in the Danish population (2,6,7). Despite these high prevalences, there might be persons who will never encounter a headache.
People who are free from headache could be resistant to ever getting a headache. In infectious diseases, there is a long tradition of research in individuals resistant or immune to a specific illness. In 1796, Edward Jenner developed the first ever vaccine based on the observation that milkmaidens were resistant to smallpox infection (8,9). More recent is the development of the HIV-1 anti-viral drug Maraviroc, following the discovery of resistance to HIV-1 infection in individuals homozygous for CCR5 Δ32 (10,11). To our knowledge, this paper is the first to examine people who have never had a headache and research on people who are headache free could reveal protective factors in headaches.
Using the nationwide public health study, the Danish Blood Donor Study (DBDS), we identified participants that had never experienced a headache – so-called headache-free individuals. The aim was to estimate the prevalence of headache-free individuals among Danish blood donors and to describe the socio-demographics and health factors of headache-free participants compared to non-headache-free participants in the DBDS.
Materials and methods
Study population
This case-cohort study was conducted from November 2015 to March 2018. Voluntary participants were recruited as part of the Danish Blood Donor Study (DBDS). The DBDS is described in detail elsewhere (12). In short, it is a scientific study based on the voluntary participation of more than 100,000 blood donors (12). It is an ongoing multicentre, public health study and biobank. Recurrent donors age 18 to 67 years were invited to participate in the present study in the DBDS (13). After giving oral and written informed consent, donors answered a digital tablet-based questionnaire at the time of inclusion (14). In this case-cohort study, we included 38,557 Danish blood donors from the DBDS who had answered a questionnaire containing the question “Have you ever experienced a headache of any kind?”.
After exclusions, the resulting study population was 32,975 individuals, see Figure 1.

Flow chart of the study.
Exclusions
We excluded 5582 individuals: 5,327 individuals were excluded due to missing answers to the question, “Have you ever experienced a headache of any kind?” and we subsequently excluded 120 individuals who had positively answered the question, “Have you ever had a migraine?” or “Have you ever had visual disturbances with a duration of 5–60 minutes followed by a headache?” and negatively answered the question “Have you ever experienced a headache of any kind?”. One hundred and thirty-five individuals were excluded due to missing information on age and gender. The excluded individuals were slightly younger (median age: 38 years, IQR = 28–50 years) when compared to the study population (median age: 42 years, IQR = 31–52 years) (Wilcoxon test, p-value < 0.0001). The excluded individuals did not differ in sex distribution when compared to the study population (chi-squared test, p-value 0.15).
Ethics statement
The study was approved by the Danish Data Protection Agency (2007–58-0015) and the Ethical Committee of Central Denmark (M-20090237).
The digital questionnaire
From the DBDS digital questionnaire, we extracted self-reported information on BMI (calculated by recall information on height and weight at the time of inclusion), alcohol consumption (never/seldom, monthly, weekly or daily), smoking status (total pack years of cigarettes, pipe, cigar and cheroot) and self-reported physical and mental health from the Short Form-12 (SF-12) questionnaire (15). The SF-12 is a 12-item questionnaire that is used to measure self-reported health-related quality of life. Through the SF-12, it is possible to calculate a physical component score (PCS) and a mental component score (MCS) where the 12 items are weighted and added to a constant (16). A higher SF-12 score indicates a better health-related quality of life.
Population registers
In Denmark, all individuals are identified through 10-digit Civil Registration System numbers, which have been assigned since 1968. Through the Civil Registration System numbers, we identified the participants from the nationwide database Statistics Denmark. We extracted information from the years 2015 and 2016 from Statistics Denmark on sex, age, level of urbanisation (<60, 60–200, 200–1000, 1000–2000, >2000 persons per square kilometre), educational level (primary or lower secondary education, high school, short-length education, middle-length education or higher long-term education), working status (working, retired, unemployed or studying) and level of income (low, low-middle, middle, high-middle and high expressed in DKK as <200,000 DKK/year, 200,000 to <400,000 DKK/year, 400,000 to <600,000 DKK/year, 600,000 to <800,000 DKK/year and >800,000 DKK/year). The conversion rate for DKK is approximately 100 DKK = USD14.87 = €13.38.
With the Danish 10-digit Civil Registration System numbers, we identified the participants in the National Patient Register and the Register of Medicinal Products to extract data on numbers of contacts with a hospital, numbers of admissions, time of admission and number of prescriptions of medicinal products. The National Patient Register contains information on all patients in public and private somatic and psychiatric hospitals in Denmark over the time period 1994–2015. The Register of Medicinal Products contains information on all sales of human and veterinary medicinal products in Denmark over the time period 1995–2016. We did not include prescriptions for headache-specific drugs, triptans and ergotamine, based on ATC codes. We did not include admissions or hospital contacts with a diagnosis of ICD10 chapter G43, G44 or R50 in our grouped comparisons.
Statistical analysis
The study population was described using counts and percentages for categorical variables, mean and standard deviation (SD) for normally distributed data and median and interquartile range (IQR) for non-normally distributed data. Differences in distributions between participants were analysed using chi-squared test or Mann-Whitney/Wilcoxon test. Logistic regression was used to analyse for association to headache resistance, adjusted for age and sex. The outcome was described with odds ratios (OR) and 95% confidence intervals (95% CI). We tested the assumptions of our adjusted logistic models by use of the Hosmer and Lemeshow goodness of fit test, which did not reject our model for either men, women or both. We only included complete cases in our adjusted logistic model. Missing information is presented in Table 1. A p-value < 0.01 was considered statistically significant.
Missing data in the study population.

Counts and proportion of missing data in each variable. BMI: body mass index; MCS: mental component score of the SF-12; PCS: physical component score of the SF-12.
Statistical analysis was performed using computer software Stata/MP 14.2, StataCorp, College Station, TX.
Results
The study population consisted of 32,975 participants (median age: 42 years, IQR = 31–52) from the DBDS. We found a total of 1362 headache-free cases (female-male ratio: 1:2.2) and 31,613 non-headache-free controls (female-male ratio: 1:1.1). The prevalence of headache-free individuals in our sample was 4.1%. There was a significant difference in age and sex distribution between cases and controls (Wilcoxon test for age p < 0.001 and chi-squared test for sex p < 0.001).
Socio-demographic characteristics of the study population are presented in Table 2.
Characteristics of the study population (n = 32,975).

BMI: body mass index; IQR: interquartile range; MCS: mental component score of the SF-12; n: numbers; PCS: physical component score of the SF-12; SD: standard deviation.
Conversion: 100 DKK = USD14.87 = €13.38.
Male sex was positively associated with being headache free with OR = 1.96 (95% CI: 1.75–2.20), see Table 3. Headache-free participants were older than controls, but when corrected for sex the OR for age was only 1.01 (95% CI: 1.01–1.02).
Multivariable logistic regression analysis.
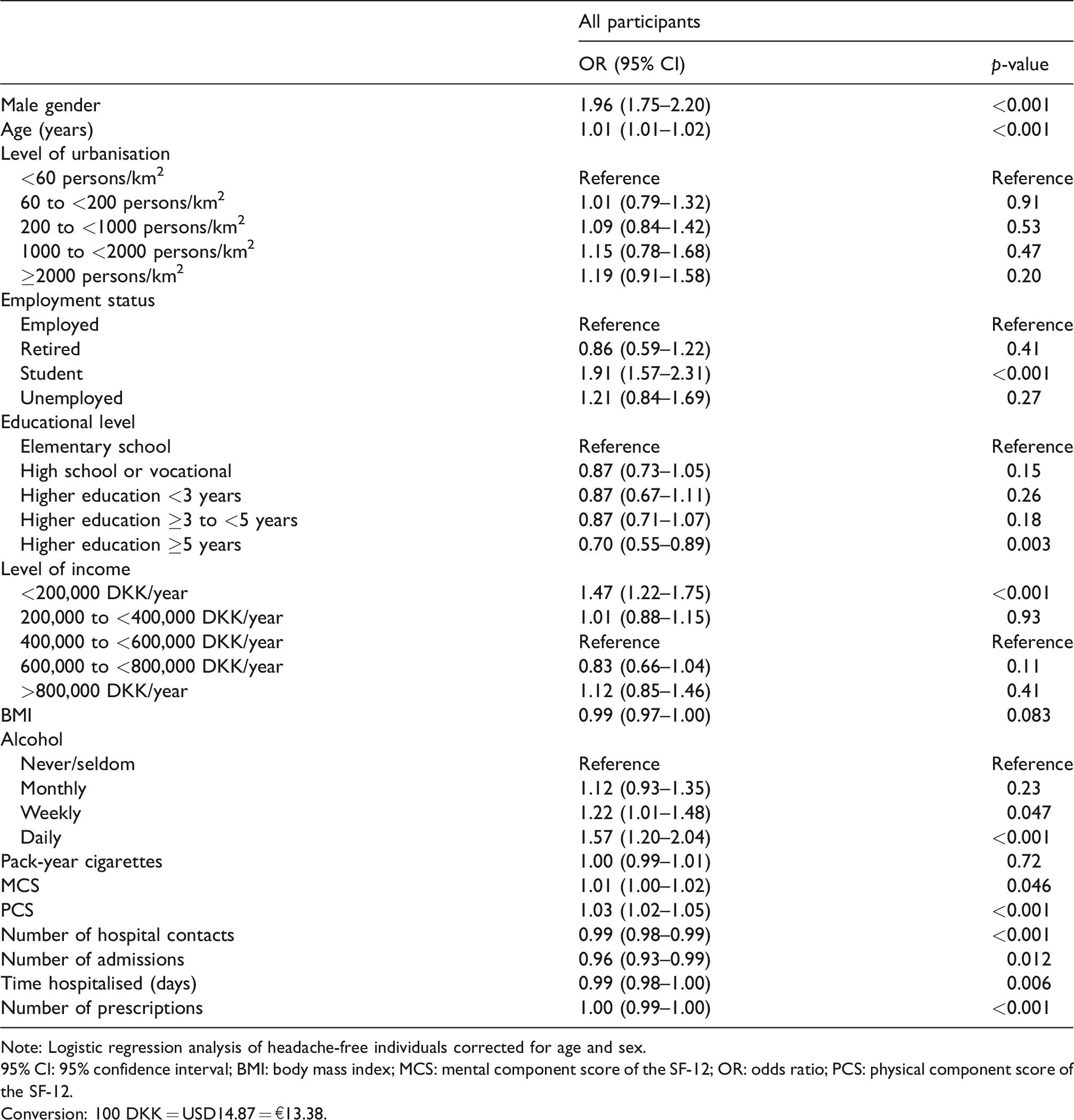
Note: Logistic regression analysis of headache-free individuals corrected for age and sex.
95% CI: 95% confidence interval; BMI: body mass index; MCS: mental component score of the SF-12; OR: odds ratio; PCS: physical component score of the SF-12.
Conversion: 100 DKK = USD14.87 = €13.38.
In the multivariate regression analysis of socio-demographic register data, corrected for age and sex, to be headache free was positively associated with an employment status as a student OR =1.91 (95% CI: 1.57–2.31) and the lowest level of income, below 200,000 DKK/year with OR = 1.47 (95% CI: 1.22–1.75). A high level of education of five or more years was negatively associated with being headache free, with an OR = 0.70 (0.55–0.89).
Self-reported lifestyle measures showed that headache-free participants had a more regular pattern of alcohol consumption (beer, wine or spirits) than controls, with more headache-free participants reporting a daily consumption, OR = 1.57 (95% CI: 1.20–2.04). Headache-free participants had a slightly higher self-perceived physical health as measured by PCS than controls with OR = 1.03 (95% CI: 1.02–1.05).
Data from the national registers on health showed that headache-free participants had slightly fewer prescriptions than controls, OR = 0.996 (95% CI: 0.995–0.998) and headache–free participants had slightly fewer contacts with a hospital, OR = 0.99 (95% CI: 0.98–0.99). Even though we did not find any difference in numbers of admissions, participants without headache spent slightly less time hospitalised when they were admitted OR = 0.99 (95% CI: 0.98–1.00).
There was no association between being headache free and level of urbanisation, BMI, self-perceived mental health or smoking status in our multivariable regression analysis corrected for age and sex.
Discussion
We report for the first time the prevalence and socio-demographic characteristics of persons who have never encountered headache. The prevalence of headache-free individuals was 4.1% among Danish blood donors. The prevalence of headache-free individuals is compatible with previous epidemiological studies on lifetime prevalence of headache (1–4). Our study population of Danish blood donors might be influenced by selection bias, so that it is not completely representative of the whole Danish population. Nevertheless, in 1991 Rasmussen et al. conducted a population study on headache in the Danish general population (2). Of the 735 participants who were interviewed about headache, 31 participants (4.2%) reported not having had a headache (17). Although the numbers of people without headache were small, the prevalence is in line with our results.
Danish blood donors are healthier than the general population (18,19). However, Hansen et al. found a prevalence of migraine of 24.2% among the Danish blood donors (20). This prevalence is comparable with previously epidemiological studies of migraine prevalence in the general population (2,21–23). Therefore, the prevalence of headache-free individuals in our sample is not expected to be influenced by a lower migraine prevalence among healthy blood donors. We did not include participants with an age of 68 years or older and as some primary headaches, like hypnic headache and nummular headache, together with many secondary headache disorders, typically occur after 50 years of age, we might underestimate lifetime prevalence of headache in our sample (24–26). In addition, as our data on headache is based on self-reported questionnaires, we might overestimate the prevalence of headache-free individuals due to memory bias of the participants.
Several clinical and epidemiological studies have shown that women experience more pain than men (27). Many clinical pain conditions like fibromyalgia or reflex sympathetic dystrophy, as well as most types of headache, have a higher prevalence in females compared with males (27–31). In accordance, there was a lower prevalence of headache-free individuals among women than men. As there are slightly more males in our study population compared to the entire Danish population, this could indicate a slight selection bias affecting the gender difference. Still, our results suggest that men are more than twofold as likely to be headache free.
Previous studies have shown that headache prevalence increases as socioeconomic status decreases (32,33). This pattern is common to many diseases and a higher socioeconomic status is thought to be protective of headache (34–42). We found no indication that being headache free is more prevalent in persons with higher socioeconomic status, high income, higher level of education or employment status. On the contrary, the prevalence of people without headache was lower among blood donors with a higher education of 5 years or more. There are two primary hypotheses for the impact of socioeconomic status on health (33): The social selection hypothesis, that a disabling disease causes a decline in social status because an individual may underperform in studies and work, and the social causation hypothesis, that a low socioeconomic status is a stressor that increases the risk of disease (33). The reason that being headache free is not affected by socioeconomic status might indicate that freedom from headache is not a strong advantage in life, and therefore does not heighten an individual’s performance. It may also, or alternatively, imply that being headache free is primarily caused by genetic factors and is not much affected by environmental factors. However, the interpretation must be cautious, as the prevalence of blood donors of low socioeconomic status is lower in our sample than in the general Danish population (13).
The statistically significant differences between headache-free participants and non-headache-free participants in health factors as well as in self-perceived physical health were numerically small and have no clinical importance. However, as blood donors are healthier than the general population, the trend towards headache-free individuals being healthier and not only unaffected by headache might be bigger in the general population (18,19). The difference in health between headache-free participants and controls was not driven by differences in lifestyle factors. There was no difference in smoking status or BMI between the groups. Headache-free participants reported more regular alcohol consumption than controls. We speculate that this is because alcohol often induces migraine attacks and that participants with migraine or other types of headaches therefore drink less than participants who are headache free.
In this study we found a prevalence of headache-free individuals of 4.1%. Being headache free was more prevalent in males, with a female-male ratio of 1:2.2. Freedom from headache was not associated with a high socio-economic status. On the contrary, headache-free individuals had a low level of income, an employment status as a student and regular alcohol consumption.
We are the first to describe a cohort of persons who have never had a headache. We hope that further research on headache-free individuals might reveal protective factors in headache. We intend in the future to conduct a range of pathophysiological and genetic studies on this cohort of headache-free individuals. By further developing the concept we hope to create a methodology that can be applied to other extremely prevalent disorders.
Article highlights
The prevalence of persons who have never had a headache was 4.1% in our sample. The female-male ratio of headache-free individuals was 1:2.2. Headache-free individuals were more likely to have a low level of income, an employment status as a student and regular alcohol consumption.
Footnotes
Acknowledgements
We wish to express a special thanks to the staff of the Danish blood banks, whose continued inclusion of blood donors into the DBDS makes this research possible.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by The Independent Research Fund Denmark 9039-00067B and Candy Foundation (CEHEAD).