
Abstract
In the Vågå study of headache epidemiology, a search was made also for cluster headache. Of the available 18-65-year-old dalesmen, 1838 (88.6%) could be examined personally (O.S.) – 51.3% females and 48.7% males. Based on current International Headache Society criteria, cluster headache seemed to be present in seven dalesmen, one female and six males (corresponding to a total prevalence of 381 per 100 000; 95% confidence interval (CI) 153-783 per 100 000). Except for the female gender, the female case was fairly typical. In one case, there were short-lasting bouts (‘minibouts’). It was felt that this also was a genuine case of cluster headache. If one excluded the latter case, there would be one female and five males [a prevalence of 106 per 100 000 for females, and 558 per 100 000 for males, giving a prevalence in the total population of 326 per 100 000 (95% CI 120-709 per 100 000)]. The confidence interval was considerable. This study therefore does not give a clear indication as to prevalence.
Introduction
Cluster headache (CH) is an important type of headache, but presumably a rare one. However, prevalence estimates in the literature vary greatly, possibly by two to three times (1). Various techniques have been used: direct methodology, questionnaires and scrutiny of health records in a circumscribed geographical area.
We searched specifically for CH in the Vågå headache epidemiology study. In the Vågå study, 1838 individuals were included (2, 3). CH is a predominantly male headache, with a male preponderance of around 84% (1). Given these premises – the limited number of participants and the fact that around 50% of the participants supposedly would be females – one could realistically not expect more than a single case or perhaps two of CH. However, the realities at the grassroots level proved to be somewhat different from these expectations.
Materials and methods
The target group in the Vågå study was 2065 18–65-year-old dalesmen. Of these, 1838 (88.6%) were personally examined on the basis of a questionnaire, the latter in its entirety administered by the principal investigator, O.S. (2). The details of this investigation have been described previously (2). Physical and a partial neurological examinations were carried out, including cranial nerves and face, neck, and cephalic structures. There were 942 females (51.3%) and 896 males (48.7%) (2), the mean age being 35.9 years.
The diagnostic criteria of the International Headache Society (IHS) (4) were adhered to. Since there are no clinically pathognomonic signs of CH, the presence of the combination of ‘five main criteria’, as outlined elsewhere (1), was also paid heed to. These criteria are: (i) unilaterality of headache (and lack of sideshift); (ii) male sex; (iii) clustering of attacks; (iv) localized, ipsilateral autonomic phenomena (lacrimation, etc.); (v) excruciatingly intense pain. One of these signs and symptoms may be lacking, without violating the diagnosis (e.g. CH in the female); even two of the five main criteria may probably be lacking [e.g. female sex + a chronic long-term pattern; cases like that have been described (5)]. In doubtful cases, other guidelines have also been used, like the IASP classification (6) and also Ekbom's guidelines (7).
When, in a doubtful case, the diagnosis of migraine without aura was considered, the IHS criteria for migraine (4) were adhered to.
Results
The CH criteria of the IHS were probably fulfilled in seven dalesmen, one female and six males (Table 1). This (
Symptomatology of cluster headache among the dalesmen
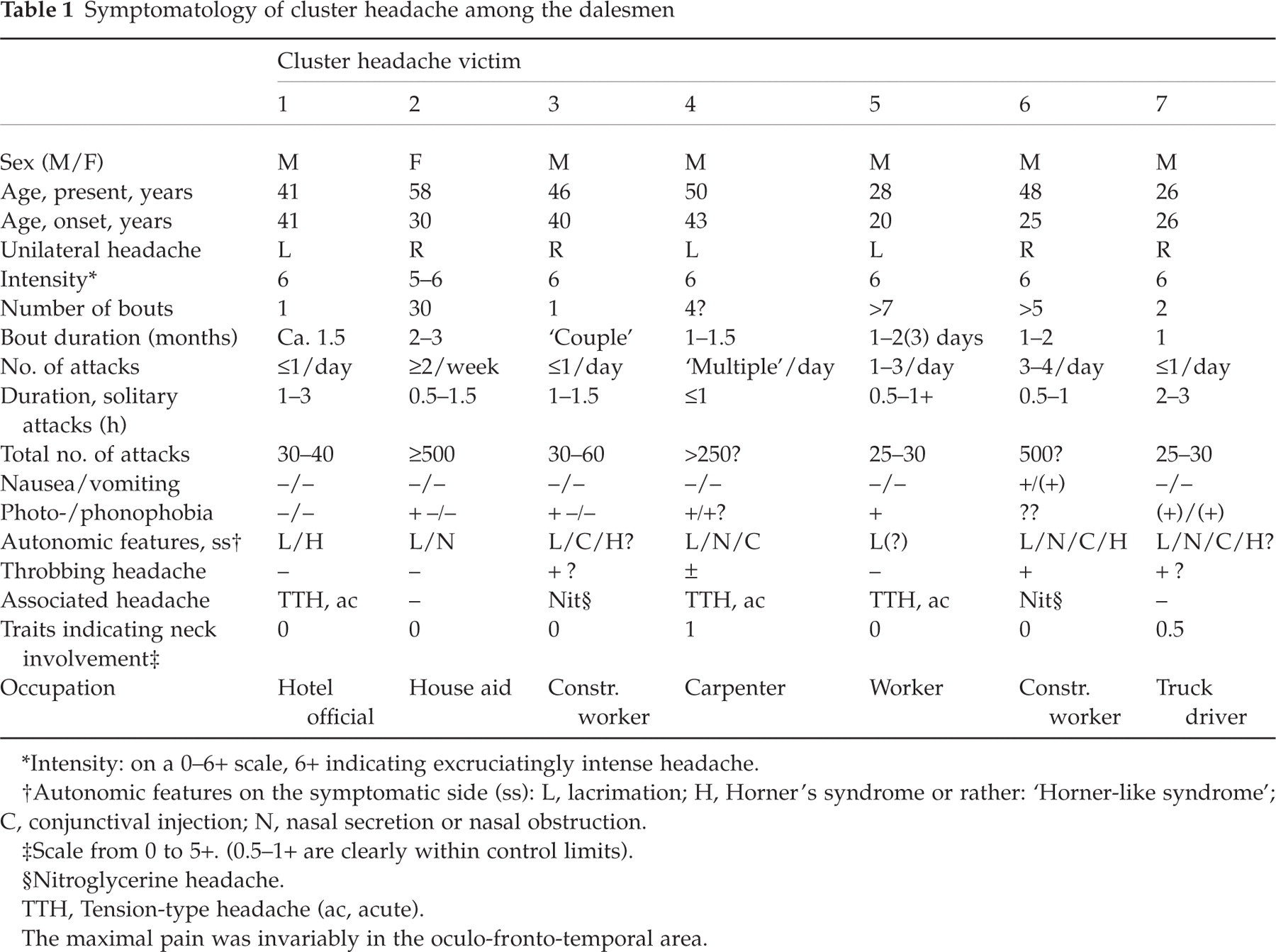
∗Intensity: on a 0–6+ scale, 6+ indicating excruciatingly intense headache.
†Autonomic features on the symptomatic side (ss): L, lacrimation; H, Horner's syndrome or rather: ‘Horner-like syndrome’; C, conjunctival injection; N, nasal secretion or nasal obstruction.
‡Scale from 0 to 5+. (0.5–1+ are clearly within control limits).
§Nitroglycerine headache.
TTH, Tension-type headache (ac, acute).
The maximal pain was invariably in the oculo-fronto-temporal area.
To the best of our knowledge, there was no relationship between the CH victims.
Cluster headache is rare in the female, and atypical features are not infrequently present in female CH victims. In the present female CH victim (no. 2, Table 1), a slightly atypical trait was that she preferred the sitting to the erect position during an attack (no pacing the floor, etc.). She was accordingly rated as having attacks of a 5–6+ intensity (on a 0–6+ scale of intensity). In Ekbom's series, close to 30% of the CH victims did sit during attacks (7). She had over the years had approximately 30 bouts of 2–3 months’ duration (Table 1). There were two or more attacks per week. An attack frequency of one attack every other day is allowed according to the IHS (4). According to various other sources, even less frequent attacks may occur periodically during the bout (1, 6): ‘two or more’ days between attacks. She was all in all rated as having a fairly typical CH (Table 2).

Dalesman no. 5 had a slightly atypical picture: the one-sided attacks (Table 1) were extremely severe (‘ròte ilt’, in the local dialect), and he had the feeling that on the symptomatic side, the eye was about to be squeezed out of its socket. But he had rather short-lasting cycles: 1–2 day (possibly 3 day) long cluster periods, with one to three attacks per day. This can fit with ‘minibouts’ (8). As regards localized, ipsilateral autonomic features, he probably had lacrimation, possibly conjunctival injection, but no nasal obstruction/rhinorrhoea. In spite of these slightly atypical traits, we have chosen to include him. However, we have calculated prevalence figures both with and without case 5.
There was still another dalesman with a borderline picture of CH, but we have chosen to set him apart (not included in Tables 1 and 2 or in the various calculations). Due to the diagnostic difficulties, some details will be given. A 42-year-old male worker had during 16–18 years had> 250 attacks (conservative estimate) of purely right-sided, extremely severe, oculo-frontal headache attacks of 2–4 h duration. The attacks were pressing in character, and there was no nausea or vomiting. What made this picture atypical was the lack of cluster phenomenon and autonomic phenomena; in other words, two typical features were missing.
There was one or less attack per week. The temporal pattern could possibly be that of a chronic CH, as outlined by the IHS (4). The lack of autonomic features was also problematic. According to the IHS, autonomic features must be present. Ekbom (7) states that attacks ‘might be’ associated with localized autonomic symptoms and signs. In other words, the presence of autonomic phenomena would, according to him, not be compulsory. Nor is the IASP (6) categorical about the presence of autonomic phenomena, stating that they are ‘usually’ present. In some CH victim series [for details see (1)], the percentage of CH victims that lack such phenomena is low. Even in ‘minibouts’, there is usually lacrimation (8).
A possible differential diagnostic alternative in this case would be migraine without aura (4). However, the following features tell rather clearly against migraine: a severity leading to restlessness, and, in spite of that, lack of nausea/vomiting, and lack of a throbbing quality of the pain. The duration of the solitary attacks is possibly more consistent with CH than with migraine: the temporal requirements of the IHS migraine criteria are not explicitly fulfilled in this case. This case should be rated as a borderline and not as a definite case of CH. We have therefore chosen not to include this case, even though, according to the five-criteria scheme (see Materials and methods) it would probably be permissible that two criteria are lacking, in this case: clustering of attacks and autonomic phenomena (1).
In the group as such, however, the clinical picture of CH, as stipulated by the IHS, seemed easily recognizable at the grassroots level. The intensity was generally excruciating. The attacks were probably not milder in these cases than in the traditional specialist-practice clientele. As shown in Table 2, all five main clinical features (1) were present in five cases, and probably in six. The average number of features was approx. 4.8, of a maximum of 5. In spite of the fact that CH had lasted for a number of years in four of them, there seemed to have been a total of more than five bouts in only two of them. Case 5 is not included in the latter assessment, because of the special temporal pattern. The total number of bouts in our series (Table 1) corresponded to the total number of bouts given by Sutherland and Eadie (9), in a University Hospital-based study, e.g. four or less bouts in 57% in the present series, vs. 66% of the cluster headache victims in their series, with case 5 also excluded in this context. Some uncertainty is of course linked to these figures, because of the limited number of bouts.
In spite of the fact that the mean duration of CH was approx. 11 years (range < 1 year to 28 years), only in one (of the seven + the one dubious case) had a CH diagnosis ever been made. In the exceptional dalesman, the diagnosis had been established in another parish where he worked at the time, by a young intern. A total of five of seven dalesmen had, in spite of a considerable number of attacks, never consulted a physician about their ailment. As one of them said: ‘The attack lasts such a short time when it comes that there is probably little to be done about it. And I know that it disappears – spontaneously’.
It is also noteworthy that symptoms and signs indicating cervical abnormalities (Table 1) were not present to a conspicuous extent.
Discussion
Some early estimates of CH prevalence were in essence comparisons between the frequency of migraine and CH in specialist/hospital practice [e.g. (10); for summary of the early evidence, see (1)]. A factor of great uncertainty in this context is the fact that migraineurs rarely seek medical advice. On the other hand, it was believed at the time that practically every one with the intense pain of CH would seek medical advice. In line with this type of reasoning, methods based on the relative frequency in hospital/specialist practice could be suspected to give too high frequencies rather than too low ones for CH. These early estimates for CH were, nevertheless, comparatively low (1). These estimates are not included in Table 3.
Prevalence of cluster headache

Previous and present studies. Mainly direct or indirect/direct methodology.
∗I, Indirect methodology; D, direct methodology.
†Actually: incidence (9.8 per 100 000). Prevalence, provided survival ≥ 15 years, 147 per 100 000 [according to (13)].
‡Control study of 1314 inhabitants > 7 years old.
§Values in parentheses: adjusted for age and sex (see text).
¶Or: 50, since one of the two did not fulfil the International Headache Society criteria.
∗∗95% confidence interval: 153–783 per 100 000; 326 per 100 000 if case 5 is excluded (see text), with confidence interval 120–709 per 100 000.
The present study and the prevalence figures of (11) differ significantly:
Another method was in the frame of University Hospital practice to identify the number of CH victims in a given catchment area [e.g. (9)]. If the belief that every CH victim would seek medical or hospital advice were true, this method could have been profitable. However, in all probability this is not a valid assumption, as also shown in the present study.
In recent years, CH has been specifically and systematically searched for in some population studies (11, 12) by indirect, or a mixture of indirect/direct methodologies (Table 3). There is a rather marked variation (13) between the highest and lowest prevalence values (Table 3) (a factor of 3 or more). This factor is probably too large to be due to chance only: differences in methodology almost certainly have contributed to the results obtained.
The highest prevalence up to now has probably been observed in 18-year-old men in Sweden: 90 per 100 000 (14). This prevalence concerns only 18-year-old men. Extrapolation from data at 18 years of age to the general population will naturally be loaded with pitfalls. At that period of life, probably only between 1/4 and 1/5 (5) of prospective CH victims have had their first attack: the mean age of onset is around 31.5 years (1). Thus, in Manzoni and co-workers’ study, 22% were ≤ 20 years at onset (5). There is, moreover, a male preponderance of approx. 84% in cluster headache (1). Given these perspectives, adapted prevalence values for both sexes combined could be around 240 per 100 000. The figures will be different if based on Ekbom's data: 29.5% of the CH victims (7) were ≤ 19 years old at onset. This would correspond to a prevalence of around 180 per 100 000. In these rough estimates, the age of onset for both sexes combined has been used. There may obviously be differences between sexes in this respect. The calculated prevalences presented here are, moreover, based on age of onset at ≤ 20 and ≤ 19 years, respectively (5, 7), and not ≤ 18 years. For this reason also, the prevalences could be slightly higher than stipulated.
D’Alessandro and co-workers (11) have made a valuable search for CH in the Republic of San Marino, i.e. within a defined, circumscribed population, scrutinizing the files of hospital neurological, ear/nose/throat, and eye disease services. Furthermore, all inhabitants received a letter/formular with relevant questions and, on top of that, 1314 inhabitants,> 7 years old, selected at random, were used as controls for the collection method. This sounds in many ways a watertight procedure. Still, they found a relatively low prevalence (Table 3). The prevalences in their study, i.e. 15 in a population of 21 792, and the one in our study differ significantly (
In two good-sized population studies comparable to the present one, i.e. the Porto and Copenhagen studies (16, 17), applying direct methodology, a prevalence of 100 per 100 000 was found (Table 3).
A population study has even been carried out among rural Africans (18): 15 500 ≥ 20 years of age. The primary contact appears to have been made by trained ‘enumerators’. In this study the methodological problems were probably considerable: a totally different culture/environment; appreciable linguistic problems; moreover, the study was carried out by proxies, apparently largely with scanty training for this extremely difficult task. The result: a probable prevalence of 30 per 100 000. Although there may be a lower prevalence among Africans than Europeans, this low prevalence probably cannot be explained on that basis only.
A solitary study of CH incidence was carried out in the Olmstead county in the USA (12). D’Alessandro
The present study shows a high prevalence, probably corresponding with that in the Swedish study (14). A remarkable finding in the Swedish study was the low consultation rate: only four of nine CH victims had sought professional aid, in spite of an average duration of approximately 6 years. At the time, it was discussed in headache circles whether this could be due to a relative ‘mildness’ of CH early in life. This does not seem to be the case, since the Swedish observation is substantiated in the present study, where only two out of seven adult CH victims had consulted a physician. D’Alessandro and co-workers (11) pointed out all the false-positive cases with their type of screening system. The present investigation shows the opposite tendency, that seems to be even more important in this context: the failure of such CH victims to consult their physician.
The latter finding probably has an important bearing on methodology in CH epidemiology studies: scrutiny of clinical records will probably not accomplish the purpose; nor will a screening by non-adequately trained personnel (since the headache has not been considered important enough to consult a physician, why would it be important enough to mention, in a questionnaire or in passing, to a strange interviewer?). The response during such a search may be negative, unless the matter is pursued in a penetrating, almost aggressive way. Emphasis is usually placed on intensity as a hallmark of CH diagnosis. An introductory question which is as important is probably: pain location. A unilateral headache, without shift of side, and with pain maximum fronto-ocularly gives a hint that one may be faced with CH.
A further factor that may increase the tendency to forgetfulness/denial concerning CH-like symptomatology is that there are long remissions. Thus, long remissions, relative mildness, and relative brevity of attacks may be factors that make many CH victims fall through the net, with indirect methodology. Even for an extreme headache on the intensity scale, like CH, there are probably no indirect methods, no shortcuts; only direct, time-consuming methods will be reliable. Indeed, none of the present CH victims would have presented at a survey of records at the county hospital departments of eye diseases, ear-nose-throat diseases, and neurology. Nor in the parish Health Centre records would any cases have been found. The one with a CH diagnosis had his record in a neighbouring Health Centre.
In the present study, the confidence interval is considerable. The study does not therefore provide a clear indication as to CH prevalence. All in all, the prevalence of CH may seem to be higher than indicated by the early investigations. What is dismaying, almost frightening, in the present study is the low consultation rate among dalesmen who suffer from CH, at least in this part of the world. This may lead to erroneously low prevalence values. The low consultation rate does not seem to depend upon an entirely different clinical picture (in particular, not a more mild one) at the grassroots level.
The clinical picture, in fact, seemed similar in most respects to well-known, regular hospital/specialist practice CH: age of onset, male preponderance, etc. (Table 4). In all of them, the painful area was the oculo-fronto-temporal area, with a fixed unilaterality. Possibly, the attack frequency within a bout (or cluster cycle) might be somewhat low (1). In one of the cases, the most typical cluster pattern was not present, in that there seemed to be ‘minibouts’ (8). We have previously proposed that ‘minibouts’ in the occasional case may last 1–2 days only (1, 8).
Cluster headache picture at grassroots level

∗If one prefers to exclude case 5.
†‘Minibouts’ (8) in one cluster headache victim.
‡Including cases with uncertain information and cases of rarely occurring photophobia: 78%.
At the time of study, two CH victims tried parenteral triptans for the attacks, with excellent effects in both. The following observation has a bearing on the severity: two of the CH victims – both construction workers – had experienced nitroglycerine headache many times (Table 1). The CH was similar to the nitroglycerine headache, and at least as intense.
In conclusion, cluster headache in the well-known form from hospital practice seems to be more prevalent than hitherto generally believed. In spite of the intensity of the pain in CH, there does not seem to be a methodological shortcut, through indirect methods, to obtain fast results as for prevalence. The only navigable route to reproducible estimates in this field is probably through well-planned, well-executed, and truly time-consuming direct methods.
Footnotes
Acknowledgements
We are indebted to GlaxoSmithKline of Norway, Pharmacia & Upjohn, and the Alf Harborg Foundation, Department of Neurology, St Olavs. Hospital, Trondheim, Trondheim University Hospital, for generous support during the various phases of the investigation. The authors are also grateful to the personnel at the Vågå Health Centre at Vågåmo for their aid. Last, but not least, we thank the inhabitants of the Vågå commune for their collaboration.