
Abstract
Background
Disability resulting from headache disorders is attributable in part to avoidant coping. Acceptance of pain connotes a willingness to experience pain in the service of life values, such that meaningful activities and goals are pursued despite pain. Acceptance facilitates positive health outcomes but has rarely been investigated in headache. Because headache disorders manifest differently than other forms of chronic pain, the present study sought to develop and validate a measure of acceptance of headache.
Methods
Forty-five candidate items were developed and, with input from an expert panel, reduced to 24 items. Five items were eliminated following administration to a development sample and exploratory factory analysis. Nineteen items were administered to a validation sample for confirmatory factory analysis and assessment of psychometric properties.
Results
Factor analysis produced a unidimensional six-item measure, the Headache Acceptance Questionnaire (HAQ). The HAQ evidenced good internal consistency, convergent validity with headache disability and related psychological constructs, and divergent validity with social desirability. The measure also distinguished between headache diagnostic groups.
Conclusions
Pending further validation in clinical settings, the HAQ may have utility in assessing psychological responses to headache symptoms, identifying targets of treatment for interventions that focus on reducing avoidance, and studying mechanisms of change.
Introduction
A substantial portion of disability associated with headache disorders appears attributable to psychological factors, in particular common psychiatric comorbidities (1) and various psychological responses to pain (2,3). Foremost among the psychological factors that have received recent attention are those germane to avoidance and acceptance.
Individuals with headache disorders frequently utilize avoidant coping strategies intended to alter the form or frequency of headache (4). Often this avoidance manifests as attempts to evade or escape from environmental stimuli or private experiences that may trigger or worsen headache attacks, such as suppressing negative thoughts and emotions. These coping strategies are collectively referred to as experiential avoidance (5) and reduce pain-related fear in the short term but over time exacerbate disability and psychiatric symptomatology (4,6). Such avoidance becomes maladaptive when it generalizes to stimuli unrelated to headache, restricts involvement in valued daily activities, or begets social isolation and depression.
A growing body of literature suggests a need to revisit the role of avoidance in headache disorders. Multiple experimental studies show sensitivity to headache triggers decreases as a function of exposure (see Martin and MacLeod (2009) (7) for a review), and behavioral interventions that seek to minimize avoidance hold considerable promise in headache. Specifically, behavioral treatments involving prolonged exposure to triggers have shown preliminary utility in reducing headache symptoms and medication consumption (8), and studies utilizing mindfulness or Acceptance and Commitment Therapy (ACT) have shown favorable impact on headache-related disability and affective symptoms (9,10). Though the existing studies are relatively small, they parallel a larger trend in chronic pain broadly, in which advances in theory and intervention are guided by a focus on functional improvement and acceptance of pain (11).
In contrast to avoidance, acceptance involves a willingness to experience aversive internal events in the service of broader values. Acceptance of pain thus connotes a willingness to experience pain as evidenced by deliberate engagement in valued activities regardless of pain (12). Acceptance of pain is associated with reductions in psychiatric symptomatology and disability, increased daily uptime, and improved work status (11,13). Among headache samples, pain acceptance accounts for substantial unique variance in migraine-related disability (14) and is inversely related to catastrophizing and pain-related interference with daily functioning (15).
Despite its established importance as a psychological process related to headache disorders, measures to assess acceptance of headache are lacking. The 20-item Chronic Pain Acceptance Questionnaire Scale (CPAQ) (13) is the most widely used measure of pain acceptance but was developed and validated among individuals with chronic musculoskeletal pain. As such, it does not capture unique aspects of headache diseases, in particular responses to interictal periods when pain is absent or avoidance of potential attack triggers, and its length precludes routine use in medical settings. Therefore, it is important to develop and validate a brief measure that assesses acceptance of head pain, which was the aim of the present study. We hypothesized that the resulting measure would assess a unidimensional construct, exhibit adequate concurrent and discriminant validity with established measures, and be meaningfully associated with relevant headache variables.
Methods
This study was conducted in three stages during 2017 and 2018: a) Development of candidate items; b) administration to a development sample to determine factor structure and facilitate scale refinement; c) administration to a broader validation sample for confirmatory factor analysis (CFA) and assessment of scale validity. Following the recommendation of Meyers, Gamst, and Guarino (16) and assuming a moderate effect size (f = 0.25), a power level of 0.80, and an alpha level of 0.05, a priori power analysis indicated a total sample size of 500 (across stages 2 and 3) was required for primary factor analytic techniques. This study was approved by the Institutional Review Board at the University of Mississippi, and all participants provided informed consent before participating.
Stage 1: Item development
Scale development began with a large number of items to facilitate data reduction and to ensure a minimum of 10 participants per item for factor analysis (17–18). Items from existing measures of pain acceptance (CPAQ) and experiential avoidance (Acceptance and Action Questionnaire [AAQ-II]) (19) were adapted such that references to pain and negative emotions were replaced with “headache.” Novel items were generated to capture effortful behavioral engagement with precipitating and exacerbating factors of headache and common headache disorder symptoms besides pain. In total, 45 items reflecting willingness to experience headache, remain in the present moment while experiencing headache symptoms, and commitment to valued activities despite headache symptoms were generated. Items also probed individuals’ use of medications to control headache, activity engagement despite environmental sensitivities (e.g. phonophobia, photophobia) or premonitory symptoms (i.e. migraine aura), and responses to headache triggers and gastrointestinal symptoms. All candidate items were termed in the form of declarative statements with a Likert-type response format (1 = never true, 7 = always true).
The 45 candidate items were then distributed to an expert panel of five researchers internationally known in the fields of headache, chronic pain, and/or Acceptance and Commitment Therapy. These individuals were selected because they had worked on the development of existing pain acceptance/avoidance measures or had published psychometric papers relevant to headache acceptance/avoidance. They rated each item on a 0–10 scale in terms of how well it captured the construct of headache acceptance and provided detailed suggestions for improving content and readability of individual items.
Stage 2: Exploratory factor analysis and item refinement
Development sample, measures, and procedure
The development sample consisted of undergraduates at a southern US university who participated in exchange for course credit. As part of a larger battery of measures, they completed a computer-administered version of the Structured Diagnostic Interview for Headache (SDIH-3) (20), which assesses ICHD-3 diagnostic criteria (21) for various headache disorders. The participation announcement invited respondents who experienced any current pattern of headache attacks. Respondents meeting diagnostic criteria for migraine (allowing 2 hours’ minimum duration, as young adults often have otherwise prototypical attacks that do not last 4 hours) (22) or tension-type headache (TTH), those with “probable” migraine or TTH (e.g. meeting all diagnostic criteria except one), and those endorsing symptoms of medication overuse headache, headache subsequent to head injury, or a prior diagnosis of cluster headache were invited to complete the 24 candidate items remaining after stage 1 of development via Qualtrics (Provo, Utah). Five hundred and seventy-seven participants were screened initially, but 43.5% were removed for suspect effort (completing the items in >25% less time than the first author), not meeting inclusion criteria, or having incomplete data, for a final sample of 315 participants.
Statistical analyses
Initial psychometrics involved assessment of inter-item and item-total statistics. Exploratory factor analysis was conducted using principal component analysis (PCA), followed by principal axis factoring.
Stage 3: Scale validation
Validation sample
The validation sample was recruited via Amazon Turk Prime Marketplace, which affords quality data collection among diverse participant samples via crowdsourcing (23). Adults living in the United States who experienced headache were invited to participate in exchange for modest compensation ($0.25). As with the development sample, responses to the SDIH informed diagnostic classification and study inclusion. Three hundred and eighteen individuals completed validity measures described below via Qualtrics, and 33 (10.4%) were excluded for evidencing suspect effort, failing embedded attention checks within the survey, or withdrawing after providing informed consent. Notably, nine participants were excluded from further analyses due to missing data or no evidence of a clear headache diagnosis. The final sample of 276 thus adhered to Nunally’s recommendation (17) regarding the optimal ratio of participants to items.
Measures
In addition to the SDIH and 19 candidate items retained after Stage 2, the validation sample was administered measures to assess concurrent and discriminant validity.
Acceptance and Action Questionnaire-II
The AAQ-II (19) is a seven-item Likert-type measure that reflects respondents’ willingness to remain in contact with private experiences such as emotions, thoughts, and bodily sensations without attempting to alter or avoid them (i.e. experiential avoidance). Lower scores indicate greater acceptance of internal experiences, and high scores reflect experiential avoidance. The AAQ-II is internally consistent and has shown expected relations with measures of avoidant coping and emotional distress (19).
Pain Anxiety Symptoms Scale-Short Form 20
The 20-item Pain Anxiety Symptoms Scale- (PASS-20)24 is a Likert-type measure that assesses fear of pain in relation to persistent pain behaviors. Higher scores reflect greater fear of pain. The PASS-20 has exhibited good convergent and divergent validity (24).
Depression Anxiety Stress Scale-21
The Depression Anxiety Stress Scale (DASS-21) (25) is a 21-item four-point Likert-type measure composed of subscales reflecting the titular negative affective states. The overall score and subscales have demonstrated good reliability and good convergent and divergent validity (26).
Headache Impact Test
The Headache Impact Test (HIT-6) (27) is a six-item self-report measure of headache-related disability as manifested by activity impairment and impact on cognitive and emotional functioning. Total scores range from 36 to 78, with higher scores indicating greater impairment. The HIT-6 has demonstrated high internal consistency, good test-retest reliability, and the ability to differentiate headache impact across diagnostic groups.
Marlowe-Crowne Social Desirability Scale
The Marlowe-Crowne Social Desirability Scale (MCSD) (28) assesses purposeful presentation of socially desirable responses. The MCSD contains 33 true-false items that query involvement in acceptable but improbable behaviors, as well as common improper behaviors. The MCSD was used to assess discriminant validity in the present study.
Statistical analyses
Structural equation modeling (SEM) was used to conduct confirmatory factor analysis based on factor structure derived from the development stage. Concurrent and discriminant validity was assessed via correlations with measures presumed to reflect related (AAQ-II, CPAQ, PASS-20, DASS-21, HIT-6) and unrelated (MCSD) measures, respectively. ANOVA with post-hoc tests was used to assess group differences in headache acceptance as a function of diagnostic status.
Results
Stage 1: Item development
Based on feedback from the expert panel, eliminations and revisions yielded a pool of 24 retained items. Items judged to be poor exemplars of headache acceptance (i.e. four focused on beliefs about headache medication, M = 4.8/10; five conflating fear of pain with acceptance, M = 6.2/10) were deleted. Qualitative feedback informed the removal of nine additional items referencing migraine-specific symptoms (e.g. photo/phonophobia, nausea), because the panel voiced concern that they would not apply to individuals with other headache disorders, and three others for interpretability concerns (e.g. referencing changing or controlling negative thoughts).
A recurrent theme from the panel’s qualitative feedback was to ensure scale items referenced acceptance using behaviorally active terms connoting activity engagement. Retained items without a clear behavioral referent or prone to subjective interpretation were thus revised in accordance with the panel’s suggested language (e.g. “… have a fulfilling life” was changed to “… doing things that I enjoy”). The 24 retained and revised items were administered to the development sample.
Stage 2: Exploratory factor analysis and item refinement
Participants
The 315 participants in the development sample ranged in age from 18 to 36 years (M = 19.2 [SD = 1.3]) and were primarily female (75.6%). Sixty-nine percent of participants self-identified as Caucasian, 21% as Black/African American, 4.1% as Asian, 3% as Hispanic, and 2% as another racial/ethnic background. The most common headache disorder diagnoses were TTH (43% episodic TTH, 2% chronic TTH, 12% probable TTH) and migraine (10% episodic migraine; 2% chronic migraine; 4% probable migraine). Participants reported experiencing headache attacks 8.6 (1.3) days per month with an average intensity of 5.2 (1.6) on a 0–10 scale.
Factor structure
Preliminary analysis
Item-total statistics for 24 items.

Note: Values in bold denote items removed from further factor analytic evaluation due to alpha-if-item-deleted values greater than the final alpha value.
Principal component analysis and principal axis factoring
Cattell’s scree test (29) revealed three components above the elbow with eigenvalues greater than 1, which explained 53.5% of the variance. Component 1 yielded an eigenvalue of 8.05 (36.6% of variance), Component 2 of 2.31 (10.5% of variance), and Component 3 of 1.41 (6.4% of variance). Further investigation of these components suggested a two-factor solution, as Direct Oblimin rotation revealed that the first two components were highly correlated (r = 0.46), and the scree plot from parallel analysis also supported a two-component solution. Two items (items 13 and 20) exhibited low communality values (<0.4), indicating inadequate fit with other variables contained in the factor solution, and were thus removed.
An examination of the pattern matrix with the 20 remaining items, however, provided support against a two-component model, as multiple items loaded highly on both factors and both components were highly correlated (r = 0.44). Review of item content revealed a high likelihood that the indicator variability stemmed from method effects, such that all of the items loading on the first component were positively worded, and those comprising the second component were negatively worded. These observations suggested a need to explore a unidimensional factor solution, and principal axis factoring was executed to force a one-component factor solution.
Principal axis factoring
Factor extraction based on PAF evidenced satisfactory matrix factorability, as Kaiser-Meyer-Olkin (KMO) = 0.91, p < 0.001, and Bartlett’s Test of Sphericity was significant at χ2 (171) = 2749.94, p < 0.0001. Internal consistency was excellent (0.91), and an additional item (item 23) was identified for exclusion based on an alpha-if-deleted value greater than the overall alpha. With the exception of this excluded item, all factor loadings exceeded the desirable cut-off of 0.32 (30). The retained 19 items were administered to the validation sample for confirmatory factor analysis.
Stage 3: Confirmatory factor analysis
Validation sample
Validation sample demographics.
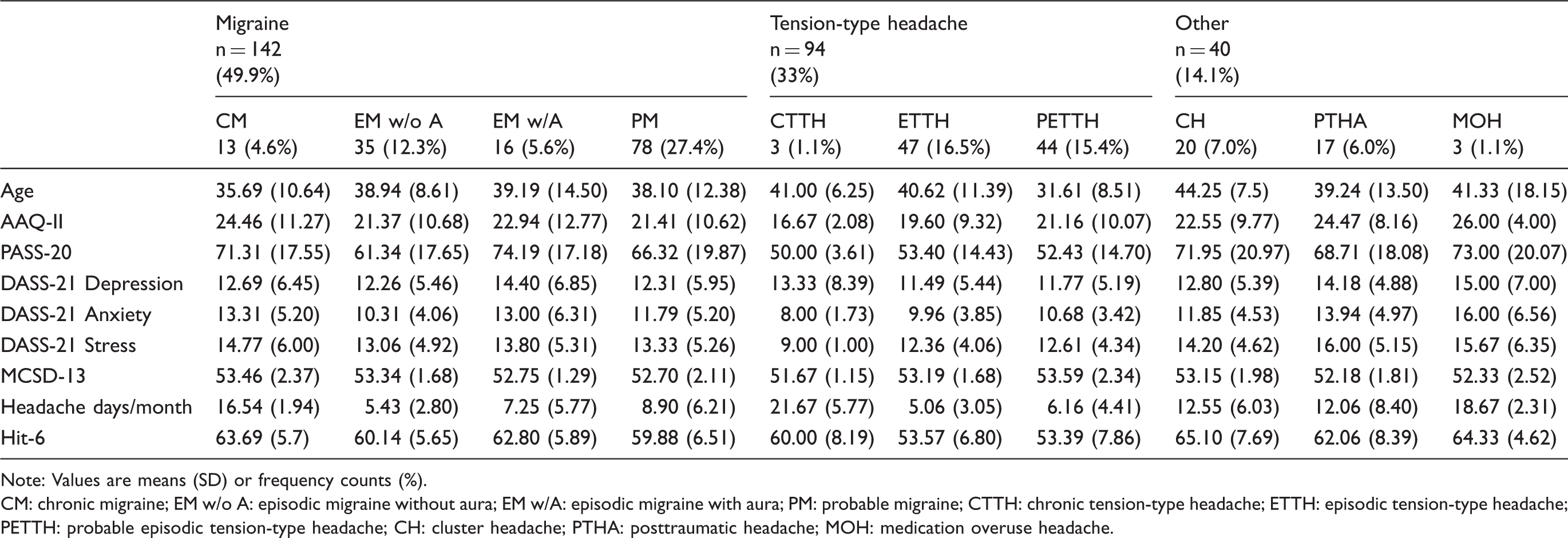
Note: Values are means (SD) or frequency counts (%).
CM: chronic migraine; EM w/o A: episodic migraine without aura; EM w/A: episodic migraine with aura; PM: probable migraine; CTTH: chronic tension-type headache; ETTH: episodic tension-type headache; PETTH: probable episodic tension-type headache; CH: cluster headache; PTHA: posttraumatic headache; MOH: medication overuse headache.
Model specification
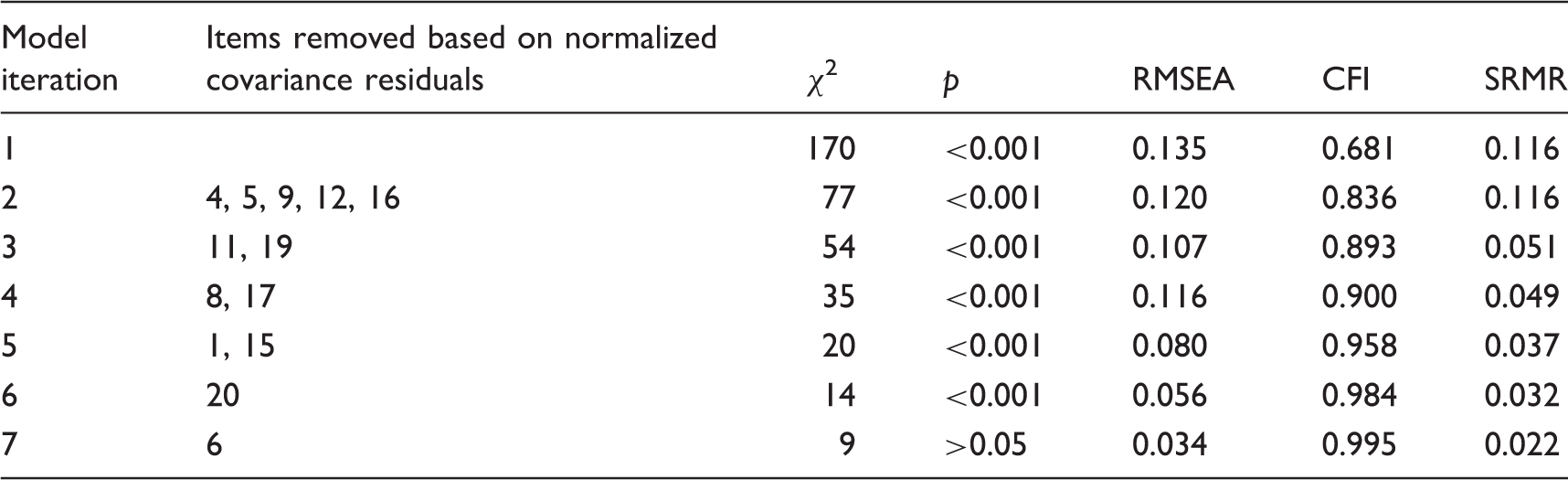
Confirmatory factor analysis (CFA) via STATA SEM was utilized to distinguish the best fitting model for a unidimensional factor solution. Recommended conservative guidelines (31) were adopted for determining model fit: Non-significant model chi-square (χ2), Root Mean Square Error of Approximation (RMSEA) <0.05, Comparative Fit Index (CFI) >0.95, and Standardized Root Mean Square Residual (SRMR) <0.08. The initial model with 19 items exhibited poor model fit: χ2(170) =1051.00, p < 0.0001; RMSEA = 0.135; CFI = 0.681; SRMR = 0.116. As these indices suggested some degree of content saturation/redundancy, an iterative process of removing items with normalized covariance residuals ≥2 was undertaken (32). All indices reflected satisfactory fit after six additional iterations that removed 13 items (see Table 3): χ2(9) = 12.020, p > 0.05; RMSEA = 0.034; CFI = 0.995; and SRMR =0.02 (see Figure 1). The final six-item model accounted for a significant proportion of the variance explained (R2 = 82%, p < 0.001) and evidenced good internal consistency (α = 0.82). The mean score was 28.37 (6.95) across all participants.
Confirmatory factor analysis model with one-factor solution showing (from left to right) the residuals, items, and factor loadings. Summary of confirmatory factor analysis results.
Validity
As predicted, total scores on the measure exhibited a strong negative correlation with measures of headache-related disability (r = −0.63, p < 0.01) and fear of pain (r = −0.59, p < 0.01), such that individuals endorsing greater acceptance of headache reported lower disability and fear of pain. Additionally, the scale exhibited smaller but significant correlations with experiential avoidance (AAQ-II: r = −0.21, p < 0.01) and negative emotions (DASS-21: r = −0.29, p < 0.01). Discriminant validity was evident via a nonsignificant relationship with social desirability (MCSD: r = 0.08, p = 0.118).
Mean HAQ total scores by diagnostic group (SD).

Individuals with variants of tension-type headache (TTH) reported significantly higher (p < 0.05) headache acceptance than individuals with migraine (CM, EM with and without aura, PM) and those reporting symptoms of cluster headache (CH), post-traumatic headache (PTHA), or medication overuse headache (MOH).
Discussion
Headache Acceptance Questionnaire (HAQ).

Scoring: Items 1–5 are reverse scored in order to obtain a total headache acceptance score. Total scores range from 6 to 42, with higher scores indicating greater acceptance of headache.
As hypothesized, final HAQ items reflect a single factor structure that endeavors to assess acceptance of headache as operationalized by willingness to experience pain via engagement in valued activities despite headache symptoms. Item content reflects behavioral manifestations of activity engagement both in anticipation of headache (three items) and when headache is present (three items). Attention to activity engagement in anticipation of pain is particularly germane to headache disorders, insofar as virtually all the major headache disorders manifest via episodic attacks and can be triggered by internal or external stimuli. The shared loading of these different items underscores the importance of trigger avoidance within (low) headache acceptance and provides further validation for the trigger-avoidance model of headache (7).
Evidence for initial validity of the HAQ was promising. Among a broad sample of adults with a variety of headache presentations, headache acceptance scores had strong inverse associations with headache-related disability and fear of pain, replicating and extending prior studies on general pain acceptance among individuals with migraine (14–15). Individuals with TTH reported greater headache acceptance than those with more severe and disabling forms of headache (e.g. migraine, cluster, post-traumatic), further supporting the construct validity of the scale. The relatively weaker relationship between headache acceptance and AAQ-II scores supports the notion that the HAQ assesses a construct related to, but somewhat distinct from, general experiential avoidance and psychological distress. The lack of a relationship between HAQ scores and social desirability not only provides evidence for discriminant validity but suggests that this new measure may not be particularly susceptible to attempts to present oneself in an overly positive light.
Future studies continuing validation efforts using treatment-seeking samples from headache clinics and further exploring differential utility of the HAQ versus existing measures of headache-related disability are needed. Although the correlation between HAQ and HIT-6 scores was moderate (r = −0.63), it was not at a level suggestive of multicollinearity. Pain acceptance is a psychological mechanism through which disability is affected, as shown in a recent mediation analysis of disability and psychiatric symptomatology (33). Nevertheless, additional studies comparing predictive utility of headache acceptance and disability would be valuable, given that both constructs involve activity engagement. Another promising area for future research is to explore relations between this measure and the Headache Triggers Sensitivity and Avoidance Questionnaire (HTSAQ) (34), which assesses potency, sensitivity, and avoidance of 24 common headache triggers. The observation of a significant inverse relationship between these measures would provide further evidence of convergent validity and validity of the underlying theoretical construct.
To the extent that the HAQ measures a change process fundamental to contemporary behavioral headache interventions, this new measure may prove valuable for various clinical purposes. Coupled with attention to unique aspects of headache, the brevity and readability (Flesch-Kincaid Grade Level (35) = 7.5) of the scale lend it well to administration within routine practice settings. Pending further investigation, treatment outcome research may reveal that HAQ scores may be utilized to identify individuals most likely to respond positively to ACT or exposure-based interventions and as a means for assessing both treatment outcome and underlying mechanisms of change.
Strengths of this study include utilization of three distinct phases for scale development and validation, assessment of headache profiles using a structured diagnostic interview, and inclusion of two different headache samples. Despite these strengths, limitations exist. The current study utilized convenience sampling of undergraduate students and an online sample obtained through Amazon Turk. Though not representative of treatment-seeking individuals, participants’ monthly headache frequency and disability reflected considerable impact of headache. Young adults were chosen because of their high prevalence of headache disorders and presumed low rates of confounding variables such as many years of medication overuse. Further, multiple studies have established the utility and reliability of samples gathered via MTurk (23). However, both samples were disproportionately female, Caucasian, and well-educated, and future work should attempt to validate the HAQ and its factor structure using more diverse treatment-seeking samples. A second limitation is that cluster and posttraumatic headache were each assessed via a single screener question (i.e. “Have you ever been diagnosed with cluster headaches” and “Did this headache develop shortly after a head injury or head trauma?”), which likely contributed to higher-than-expected rates of these conditions. Caution is thus warranted when applying these findings to these less common primary and secondary headache disorders. Pending further research, however, the present effort provides a novel instrument to assess acceptance of headache that may prove promising in both clinical and research settings, advancing both the science of headache medicine and the utility of behavioral interventions.
Article highlights
Headache acceptance is a distinct psychological construct that is meaningfully associated with variables of prognostic importance. The six-item Headache Acceptance Questionnaire (HAQ) assesses acceptance of headache and displayed promising initial psychometric properties, including convergent validity with measures of disability and related constructs, divergent validity with a measure of social desirability, and the ability to distinguish between diagnostic groups. Acceptance of headache warrants attention in clinical contexts as it may be a target for reducing headache disease-related disability and studying treatment outcomes and mechanisms of change.
Footnotes
Author note
This research was the doctoral dissertation of the first author.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: TAS has served as consultant for Alder. The other authors report no conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.