
Abstract
Background
Studies of musculoskeletal pain patients confirm that acceptance of pain and values-based action are strong predictors of pain-related disability and that interventions fostering “psychological flexibility” confer positive outcomes. However, data on these processes in migraine remain limited. This cross-sectional study examined relations between components of psychological flexibility and headache among treatment-seeking migraineurs.
Methods
A total of 103 adults (M age = 41.5 (11.9) years; 88.2% female) with ICHD-confirmed migraine (71.8% episodic, 28.2% chronic) across three clinics completed measures of psychological flexibility and headache-related disability. Hierarchical regressions quantified relations between acceptance/values-based action and headache variables after first controlling for pain severity and gender.
Results
Acceptance of pain and values-based action accounted for 10% of unique variance in headache severity (ΔR2 p = 0.006) and up to 20% in headache-related disability (ΔR2 ps = 0.02 and < 0.001) but were weakly related to headache frequency. Psychological flexibility was more strongly associated with MIDAS-measured disability than was headache severity or headache frequency. Significant effects were typically of medium-to-large size and driven primarily by values-based action.
Conclusions
Paralleling results from the broader chronic pain literature, pain acceptance and values-based action play significant roles in headache pain and disability. Further study of interventions targeting these processes may enhance existing treatments.
Keywords
Introduction
Migraine affects 12% of the population yearly (1) and is the third most common medical condition worldwide (2), resulting in substantial personal disability (1–3). A growing literature attests to the role of psychological factors in migraine. Psychiatric disorders such as major depression and anxiety disorders are commonly comorbid with migraine, and these conditions compound the negative impact of migraine; their presence is associated with a poorer treatment prognosis, increased disability, and lower satisfaction with medical care (3–5).
Most recently, interest in psychological factors relevant to headache has expanded beyond discrete disorders and into dimensional constructs such as fear of pain, maladaptive coping, and avoidance of headache triggers (6–8). These manifestations of experiential avoidance reflect an inability or unwillingness to experience aversive private experiences (e.g. bodily sensations, thoughts, emotions) (9). In chronic pain, avoidance is motivated by fear of pain and of pain-related impairment. Although effective in reducing immediate discomfort and accompanying negative affect, avoidance that is prolonged or unwarranted can foster hypersensitivity to pain stimuli, physical deconditioning, and social isolation (8,10). Acute pain paradigms link avoidance with reduced pain tolerance and poor coping (11,12), and clinic studies with chronic pain patients confirm that avoidance is negatively associated with successful adjustment to pain, independent of pain severity (13,14).
In contrast to the maladaptive response of avoidance, “psychological flexibility” denotes a willingness to experience internal events as they occur (acceptance) and engage in behaviors to achieve larger goals and values (values-based action), even in the presence of pain (14). Therapeutic interventions designed to foster psychological flexibility, principally acceptance and commitment therapy (ACT) (9), endeavor to improve functioning more than to reduce symptoms. These interventions have a rapidly-growing body of evidence for efficacy with patients with recurrent medical conditions such as diabetes (15) and epilepsy (16).
The efficacy of interventions fostering acceptance of pain and values-based action is particularly well-established in chronic pain, such that the American Psychological Association designated ACT as having “strong research support” for chronic pain based on results from numerous randomized controlled trials (17,18). Although most studies have focused on heterogeneous pain samples, recently these interventions have been evaluated in two small studies of chronic headache. In both, interventions emphasizing pain acceptance and values-based action yielded significant reductions in headache-related disability and affective symptoms compared to usual treatment (19,20). Despite these promising findings, the underlying constructs targeted by these interventions merit study among migraine sufferers. The purpose of the present study thus was to examine the roles of acceptance of pain and values-based action in migraine patients. We hypothesized that pain acceptance and values-based action would be inversely associated with migraine severity, frequency, and disability, even after controlling for relevant demographic variables and headache pain itself. A secondary aim was to explore relations between fear of pain and psychological flexibility.
Methods
Participants
From March 2011 to April 2013, migraine clinic patients were recruited from two neurology clinics and one family medicine clinic across three states in the southeastern United States. In accordance with International Classification of Headache Disorders, second edition (ICHD-II) diagnostic criteria in use when the study began, treating physicians confirmed diagnoses of episodic migraine (EM, with or without aura) or chronic migraine (CM) (21,22).
A priori power analysis was informed by effect sizes obtained in a prior study among general musculoskeletal pain patients, in which pain acceptance and values-based action accounted for 7–27% of incremental variance in functioning (23). Assuming a conservative effect size (f2 = 0.10), a power level of 0.80, and an alpha level of 0.05, 100 participants were required to support the primary analyses. A total of 103 clinic patients participated in the study. The mean age was 41.45 years (SD = 11.92) and ranged from 18 to 81. The majority identified as female (88.2%) and Caucasian (91.2%) and had completed some level of education beyond high school (79.4%).
Measures
The Chronic Pain Acceptance Questionnaire (CPAQ)
The CPAQ is a 20-item Likert-style measure that assesses acceptance of pain specifically (24). Respondents rate each item on a 0 (never true) to 6 (always true) scale. Nine items are reverse-scored, and responses are summed for a total score (range: 0–120) and into two subscale scores established through factor analysis: Activity Engagement and Pain Willingness, as acceptance of pain involves both engaging in activities despite pain and being willing to endure pain (24). Examples of statements assessing Activity Engagement include “There are many activities I do when I feel pain” and “When my pain increases, I can still take care of my responsibilities.” Examples of items assessing Pain Willingness include “I need to concentrate on getting rid of my pain” and “I would gladly sacrifice important things in my life to control this pain better” (Pain Willingness items are negatively keyed and reverse-scored). The present study used the CPAQ total score, which ranges from 0 to 120; higher scores indicate greater acceptance of pain.
The Chronic Pain Values Inventory (CPVI)
The CPVI is a 12-item self-report measure designed to assess one's success at living according to personal values while also living with chronic pain (25). Respondents rate each of six values domains (family, intimate relations, friends, work, health, and growth/learning) on a 0 to 5 scale in terms of the importance of that value (0 = not at all important; 5 = extremely important) and their success in living according to that value (0 = not at all successful; 5 = extremely successful). Item responses are summed and then averaged to yield two subscale scores for Importance and Success, each of which ranges from 0 to 5. The CPVI has good reliability as well as both convergent and divergent validity (22,25). The Success subscale typically is used as a measure of values-based action (22) and was used as such for the present study.
Migraine-related disability
Because they quantify disability in different ways and over different recall periods, both the Migraine Disability Assessment Scale (MIDAS) (26) and the Headache Impact Test (HIT-6) (27) were used as measures of headache-related disability. The MIDAS quantifies days in which headache limited functioning at work/school, home, and in family/leisure activities during the past three months. Total scores range from 0 to 270, with higher scores indicating greater impairment; scores >20 are indicative of severe headache-related disability. The MIDAS is the most frequently used measure of headache-related disability and has established reliability and validity (26,28). The HIT-6 is a six-item Likert-type measure that sums ratings of functional impairment, pain severity, and the emotional/cognitive impact of headache over the past four weeks. The total score ranges from 36 to 78, with higher scores indicative of greater impairment; scores > 55 are indicative of “substantial” impact of headache on functioning. The HIT-6 has demonstrated good reliability and convergent validity with other measures of headache-related disability (27,28).
Pain Anxiety Symptoms Scale, Brief Version (PASS-20)
The PASS-20 is a reliable and valid 20-item Likert-type self-report measure that assesses fear of pain (29). Items are rated on a 0 (never) to 5 (always) scale and summed to yield an overall score that ranges from 0 to 100; higher scores indicate greater fear of pain.
General Health Questionnaire (GHQ-12)
The GHQ-12 is a Likert-type measure of general mental health (30). Respondents are asked to rate the prevalence of 12 emotional experiences “over past few weeks” using a 0–3 scale. Responses are summed to create a total score that ranges from 0 to 36, with higher scores indicating poorer mental health. The GHQ-12 has been used in numerous settings with a variety of populations and has been shown to be both reliable and valid (31).
Procedure
Participants were recruited during scheduled appointments and through mailed letters from their physicians' offices. Participation was offered in paper format at the clinics and via an online link to the measures in electronic form. Sixty-four participants completed the paper version of the survey, and 39 completed the measures online. Headache diagnosis was confirmed by the treating physician at each clinic in adherence with ICHD criteria.
Standard protocol approvals, registrations, and patient consents
This study received full ethics approval from the institutional review board at the University of Mississippi. Patients completing the measures in paper format did so in the waiting room of the respective clinic and provided written informed consent; those completing the measures online provided informed consent via digital signature.
Statistical analyses
Associations between variables were assessed using Pearson bivariate correlations to assess for multicollinearity. As the CPAQ and CPVI have not been frequently used with headache patients, we calculated basic psychometric properties of these scales. Main hypotheses were tested using a series of hierarchical multiple linear regressions for each criterion variable: headache severity, headache frequency, reported number of pain-related medical visits within the past six months, and headache-related disability (MIDAS and HIT-6). Headache severity and relevant covariates were entered into the first block of each model (except when severity was the criterion variable). The second block added the components of psychological flexibility entered simultaneously (CPAQ and CPVI scores), to determine the unique variance accounted for by these variables independent of headache pain and relevant covariates.
Results
Sample characteristics
Of the 103 patients, 55 (53.4%) met diagnostic criteria for EM without aura, 19 (18.4%) for EM with aura, and 29 (28.2%) for chronic migraine (CM). Mean headache frequency and proportion of patients with various migraine diagnoses did not differ significantly across the three clinic recruitment sites. Mean headache severity was 6.85 (SD = 1.82), and mean headache frequency was 25.60 days (24.47) during the last three months, or 8.53 days per month. The mean HIT-6 score was 63.28 (SD = 6.16), and the mean MIDAS score was 36.86 (43.33), both indicative of a substantial level of disability among these treatment-seeking migraineurs.
Scale properties
As expected, pain acceptance and values-based action were significantly negatively correlated with both measures of headache disability (MIDAS: –0.35 and –0.47; HIT-6: –0.27 and –0.38, respectively; all ps < 0.01) and with fear of pain (–0.28, p < 0.01; –0.22, p = 0.03). CPVI scores, but not CPAQ scores, were strongly associated with general psychological distress (–0.45, p < 0.001). The MIDAS and HIT-6 were correlated with each other (r = 0.52, p < 0.001), as were the measures of psychological flexibility (r = 0.34, p = 0.001), but multicollinearity was not of concern as none exceeded r = 0.60.
The CPAQ mean total score was 61.05 (17.46), and mean scores on individual items ranged from 2.07 (1.78) to 3.88 (1.68). Internal consistency for the 20-item CPAQ as quantified by Cronbach's alpha was 0.84. The mean total score of the CPVI Success subscale, which averages the six individual item scores, was 3.29 (1.05), and mean scores on individual items ranged from 2.87 (1.34) to 3.87 (1.16). Internal consistency for the six-item Success subscale of the CPVI was 0.90 (Cronbach's alpha).
Means for the CPAQ and CPVI scores did not differ by race/ethnicity or migraine diagnosis, but gender differences in pain acceptance on the CPAQ and headache severity were observed. Specifically, females reported less acceptance of pain (M = 59.47 (17.49) vs. 71.25 (14.12), p = 0.028) and higher mean headache severity (M = 7.06 (1.72) vs. 5.50 (1.98), p = 0.005) than males. Thus, gender and headache severity were included as covariates in Block 1 of the subsequent regression models.
Regression models
Pain severity, pain frequency, and pain-related medical visits
Hierarchical multiple regression analyses of psychological flexibility variables in relation to headache-related functioning.
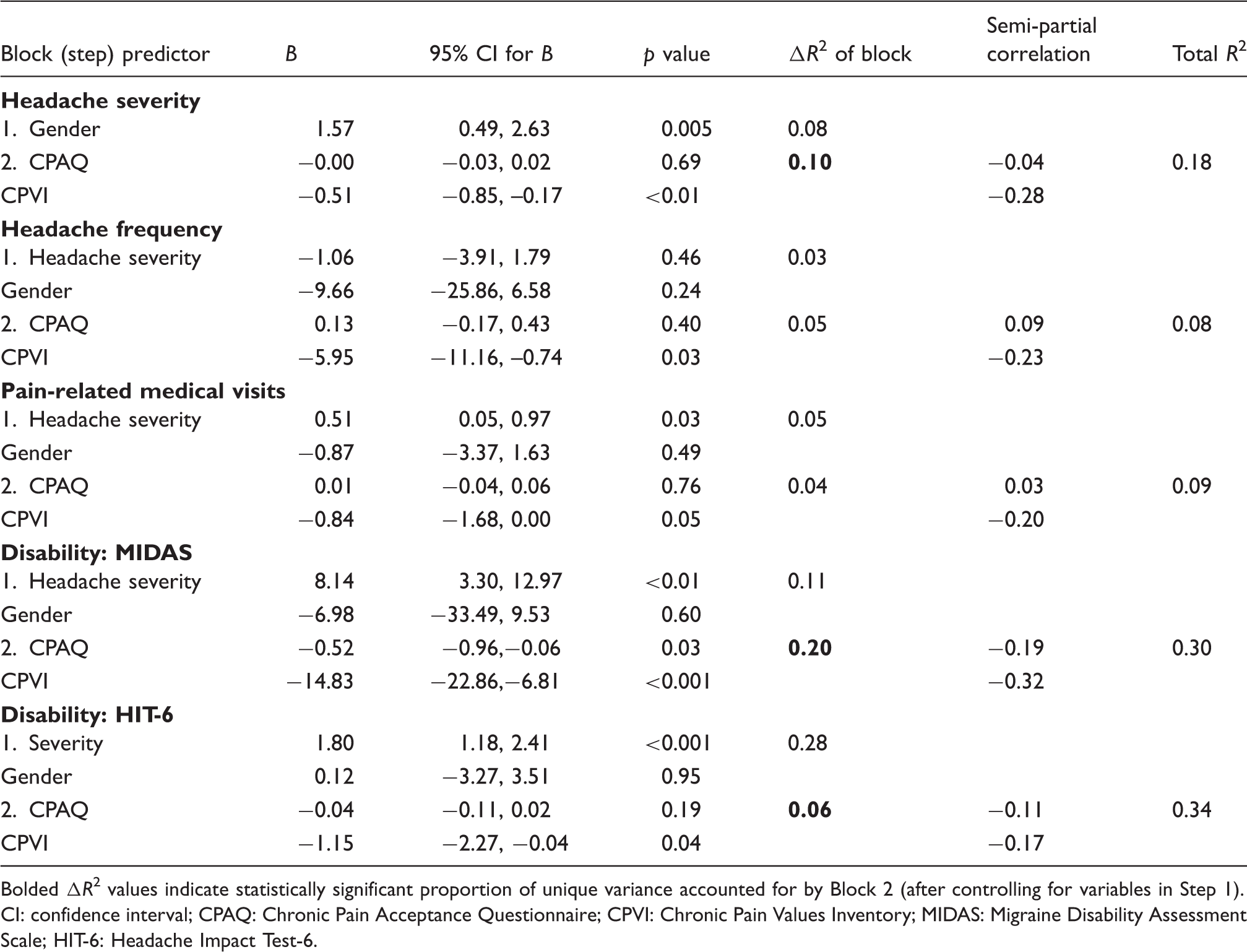
Bolded ΔR2 values indicate statistically significant proportion of unique variance accounted for by Block 2 (after controlling for variables in Step 1). CI: confidence interval; CPAQ: Chronic Pain Acceptance Questionnaire; CPVI: Chronic Pain Values Inventory; MIDAS: Migraine Disability Assessment Scale; HIT-6: Headache Impact Test-6.
Headache-related disability
In the first disability regression, MIDAS scores served as the criterion variable. The addition of psychological flexibility scores provided a unique increase in R2 of 20% (p < 0.001), indicating that together the CPVI and CPAQ scores contributed substantially and uniquely to MIDAS scores. As with the relative contributions of the headache severity regression, CPVI scores accounted for considerably more variance than CPAQ scores (10.18 vs. 3.76%). In the second disability analysis using the HIT-6, psychological flexibility provided a significant but smaller change in R2 of 0.06 (p = 0.020). CPVI scores contributed a significant 3% of the variance in HIT-6 scores when other variables were held constant, while CPAQ scores contributed only 1.3%.
Acceptance of pain and values-based action and fear of pain
As an exploratory aim, relations between psychological flexibility and fear of pain were quantified. Despite significant negative correlations between the measures of psychological flexibility and PASS-20 scores, CPAQ and CPVI scores did not account for unique incremental variance in fear of pain after controlling for gender, headache severity, and disability (ΔR2 = 3%).
Sensitivity analyses
In order to determine whether the observed relations between psychological flexibility and headache disability were attributable instead to general psychological distress, the previous disability regressions were re-run to also include the GHQ-12 scores as covariates in Block 1. Psychological flexibility remained uniquely associated with migraine-related disability as measured by the MIDAS, accounting for 12% of incremental variance (p = 0.001). CPVI scores contributed a significant 7% of the variance when other variables were held constant, while CPAQ scores did not contribute significantly.
Discussion
The current study evaluated the constructs of pain acceptance and values-based action, two components of psychological flexibility, in the context of headache-related outcomes among treatment-seeking migraineurs. Consistent with prior findings from musculoskeletal pain studies (14,17,24), psychological flexibility was associated with improved patient functioning independent of headache severity and gender differences.
Inverse relationships were found between the measures of psychological flexibility and migraine severity, disability, and pain-related anxiety, such that greater acceptance of pain and engagement in valued activities was associated with lower impact of headache. Psychological flexibility was most strongly associated with migraine-related disability, showing a medium-to-large effect on MIDAS scores (20% of variance) after controlling for pain severity and gender differences. Sensitivity analyses confirmed that this effect was not attributable to general psychological distress. Notably, pain acceptance and values-based action accounted for more variance in MIDAS scores after controlling for covariates than did headache frequency or severity before any covariate adjustments (19% and 11%, respectively). These findings further underscore the importance of avoidance (low psychological flexibility) in headache, particularly in headache-related disability, but do so more broadly than has the fear-avoidance model of pain (10). That is, the psychological flexibility model encompasses broader patterns of experiential avoidance (vs. situational avoidance) and incorporates psychological processes beyond fear of pain specifically (e.g. values-based action, mindfulness) (32). As such, the present findings build on a growing body of literature suggesting that psychological responses to pain may be more disabling than pain itself (13,14,17,33).
Psychological flexibility was uniquely associated with disability also when measured by the HIT-6, though the relationship was not as strong as with the MIDAS, possibly because of differences in response formats of the two disability measures. The MIDAS quantifies days of impairment from headache, while the HIT-6 primarily measures the affective and cognitive impact of headache using a Likert-type scale. We included both measures in light of data suggesting that using both with treatment-seeking headache patients provides a more comprehensive picture of disability than either measure alone (28). Psychological flexibility and headache severity shared a significant inverse relationship. However, psychological flexibility did not exhibit a similar relationship with migraine frequency or number of pain-related medical visits, suggesting that psychological flexibility is most strongly associated with pain perception and impairment. This finding is also consistent with the theoretical tenets of ACT, which prioritizes improvements in functioning above symptom (pain) reduction (9).
Examination of the squared semipartial correlation coefficients showed that the significant effects were driven by values-based behavior more than pain acceptance. The predominant role of values-based action across these three clinic samples underscores that values-based action is not only distinct from pain acceptance (25), but that these two constructs differentially account for unique variance in the domains of disability and quality of life (14,17,23,34). To this end, treatments fostering both pain acceptance and values-based action may hold promise for migraine patients, and the efficacy of these interventions for chronic musculoskeletal pain is already very well established (17,18).
In light of the present findings and empirical challenges to the longstanding clinical advice to avoid headache triggers (8), an alternative approach of promoting psychological flexibility may have far-reaching clinical implications that are yet fully realized in migraine. Two small trials have shown promise for interventions principally targeting psychological flexibility as applied to chronic headache sufferers (19,20), and the present study provides additional impetus for pursuing further research on this construct within migraine specifically.
Strengths of the present study include strong external validity as treatment-seeking patients were recruited both from general practice and neurology clinics across three states, adherence to ICHD diagnostic criteria, and a large sample size dictated by a priori power analysis. Despite the contributions of the current study to understanding the role of psychological flexibility within migraine, limitations exist. First, the cross-sectional design does not lend itself to inferences of causality. Possibly reductions in migraine-related disability increase pain acceptance and values-based action, but that notion is not supported by results from prospective (23) studies and clinical trials (16,19,20). Longitudinal studies and assessment of treatment mediators may further establish temporal relations between psychological flexibility and headache. A second limitation is that the measures of pain acceptance (CPAQ) and values-based action (CPVI) are frequently used in musculoskeletal pain studies but are rather uncommon in headache research. Important differences often manifest between musculoskeletal and headache pain patients, such as differential expectations for improvement and more constant pain vs. episodic attacks characteristic of migraine. No headache-specific measures of pain acceptance or valued action exist, however, and our selection of these measures was informed in part by a recent study suggesting they are viable among headache samples (35). The migraine patients in the present study and the Dindo et al. study (35) obtained similar scores on both the CPAQ and CPVI as musculoskeletal pain patients presenting to primary care settings (14). In conjunction with the included reliability analyses, both measures appear psychometrically sound for further use in headache. As interest in psychological flexibility grows among headache researchers and practitioners, developing headache-specific measures of these and other processes of psychological flexibility may prove useful.
Other valuable future directions include longitudinal studies assessing psychological flexibility processes as potential mediators of long-term headache outcomes and as resilience factors that may reduce one's likelihood of headache progression or chronification. From a treatment perspective, needed are larger trials of ACT for migraine using active control groups and follow-up periods of long duration. To the extent that interventions targeting psychological flexibility prove efficacious and complement established pharmacologic and behavioral migraine interventions, their integration may yield added clinical benefit.
Article highlights
Acceptance of pain and values-based action were strongly associated with headache frequency and disability. These components of psychological flexibility accounted for more unique variance (after controlling for covariates) in disability on the Migraine Disability Assessment Scale (MIDAS) than did headache severity or frequency prior to any covariate adjustment. These findings confirm the importance of these processes in headache and the relevance of the psychological flexibility model to headache, and may inform future treatment advances.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest
Dr Smitherman serves as an editorial board member of Headache and receives research support from Merck. The other authors have nothing to declare.