
Abstract
Migraine is defined by attacks of headache with a specific length and associated symptoms such as photophobia, phonophobia and nausea. It is long recognized that migraine is more than just the attacks and that migraine should be understood as a cycling brain disorder with at least 4 phases: interictal, preictal, ictal and postictal. However, unlike the pain phase, the other phases are less well defined, which renders studies focusing on these phases susceptible to bias. We herewith review the available clinical, electrophysiological, and neuroimaging data and propose that the preictal phase should be defined as up to 48 hours before the headache attack and the postictal phase as up to 24 hours following the ictal phase. This would allow future studies to specifically investigate these migraine phases and to make study results more comparable.
Introduction
Migraine is defined by its periodicity and specific phases (1). During the interictal phase – the interval between two migraine attacks – patients are usually relatively symptom free. The transition between the interictal phase and the migraine attack is poorly understood. Functional imaging evidence suggests certain regional activation in the brain even before the headache starts (2,3). Therefore, when a migraine attack starts, it comprises three different phases: i) preictal – the time before the headache starts, when the patient may develop prodromes, including appetite changes, thirst, yawning, or others; ii) ictal – when the patient experiences headache, which lasts by definition 4–72 hours (4); iii) postictal – the time following the cessation of the headache, characterized by non-headache symptoms such as cognitive deficits, fatigue, and others (5). The definition of prodromes may be traced back to John Fordyce in 1758 in his De Hemicrania where he observed polyuria and mood changes before the headache (6). Over the last few years the understanding of a migraine attack has been improved. Accumulating evidence suggests the activation of the hypothalamus prior to the ictal phase (i.e. in the preictal phase) leading to hypersensitivity to incoming stimuli and subsequently the migraine attack (2,3). Even experimentally triggered migraine attacks seem to follow a similar chronological sequence of symptom development: First the prodromal symptoms, then the headache attack (7–9).
The term of prodrome was first mentioned in the International Classification of headache disorders, 2nd edition (ICHD-2) in 2004 (10). But only in the latest revision of the ICHD, 3rd edition (ICHD-3) in 2018 are the prodromes and postdromes defined as up to 48 hours before the onset of pain and 48 hours after the cessation of pain (4). This allows for interpretation, since any time between 0 and 48 hours is acceptable. If the preictal and postictal phases reflect the initiation and the termination of a migraine attack, we need an evidence-based approach to better define both phases. In this article, we will review clinical studies, physiological studies and functional imaging studies, to better delineate both phases and hopefully to answer the question, when a migraine attack starts, and when it ends.
Studies on preictal and postictal phases
Clinical studies
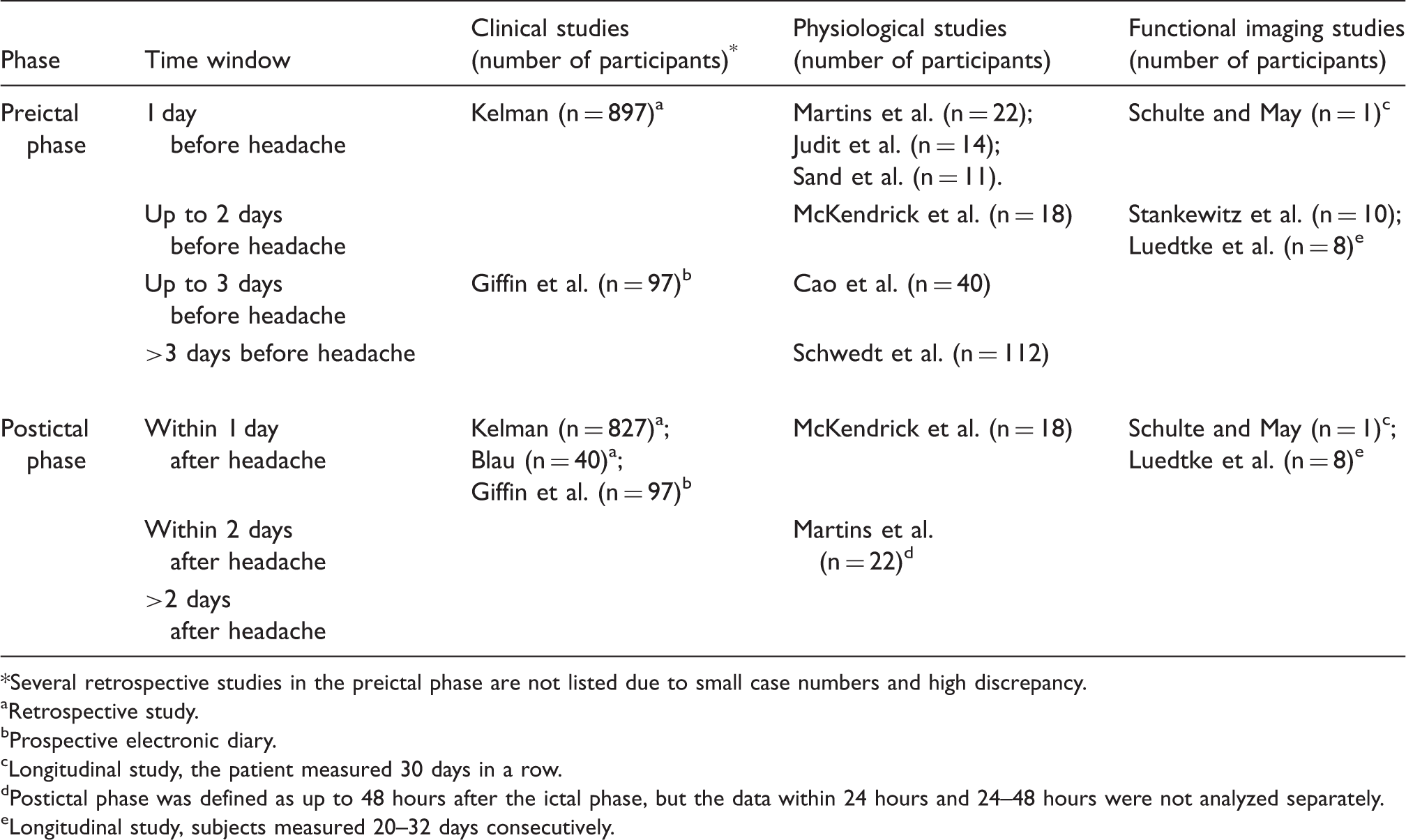
Several studies focused on the prodromal symptoms (previously known as premonitory symptoms) of migraine, but most were retrospective and thus susceptible to recall bias. As a result, the time window for the prodromal symptoms varied greatly among studies, from several hours to several days (11–14). One study by Giffin et al. in 2003 used a prospective electronic diary in which 97 patients documented prodromal symptoms up to 72 hours before the headache started. The symptoms successfully predicted subsequent migraine attacks in 72% of the entries (15). These authors used the same method to track postdromal symptoms and found that 97 (81%) of the 120 patients reported postdromal symptoms, and most of these symptoms (93%) returned to normal within 24 hours after the headache had subsided (16). Other studies on the postictal phase used a retrospective design and reported that the majority of symptoms disappeared within 24 hours after the headache had ended (17,18).
Physiological studies
Electroencephalogram Visual processing Evoked potentials Quantitative sensory testing Functional imaging studies Studies investigating the preictal and postictal phases of migraine. Several retrospective studies in the preictal phase are not listed due to small case numbers and high discrepancy. Retrospective study. Prospective electronic diary. Longitudinal study, the patient measured 30 days in a row. Postictal phase was defined as up to 48 hours after the ictal phase, but the data within 24 hours and 24–48 hours were not analyzed separately. Longitudinal study, subjects measured 20–32 days consecutively.
An electroencephalogram (EEG) study using an entropy-based analytical method showed an increased complexity during the preictal phase (up to 72 hours) compared to the interictal phase (19). Another study showed an EEG power difference in different frequency bands up to 24 hours before the migraine started; this difference lasted up to 48 hours after the resolution of the headache (20). It needs to be pointed out that it is not known whether entropy is indeed a good measure for migraine biology and the same applies to EEG power analysis.
One study examined the center surround suppression (CSS), an indirect measure of the visual cortical balance between excitatory and inhibitory neurons. They found that the CSS started to weaken 48 hours prior to the migraine headache and returned to baseline 24 hours after the ictal phase (21). Another study examined the after-image duration across different migraine phases and found an increased duration of the after-image during the ictal phase compared to the interictal phase. Of note, the after-image duration showed a trend towards elevation (in comparison to the interictal phase) starting 2 days before the headache and lasted up to 1 day after the headache stopped (22).
Evers et al. showed that the loss of cognitive habituation as measured by visually evoked event-related potentials (ERP) gradually increased from the interictal phase towards the migraine attack (23). However, the sample size was relatively small (n = 14), and the timing of examination scattered over a wide range from 1 to 26 days before the start of the headache. Therefore, no clear cut-off point can be concluded in this study (23). Another study on visual evoked potential (VEP) covered 1 day in the preictal phase and up to 2 days in the postictal phase. They found a significantly decreased habituation during the preictal phase, which normalized during the attack, and showed a trend towards elevation during the postictal phase (24). A study using laser-evoked potentials and targeting the pain pathway found, however, no difference across migraine phases (25).
In one study using quantitative sensory test (QST), the authors found a decrease in heat pain threshold (HPT) during the preictal phase (up to 24 hours) (26). Another study found a positive association between HPT and the time until the next migraine attack, insofar as the HPT gradually descended toward the migraine attack beginning 7 days before the ictal phase. Of note, most patients (19/29) in this study were examined within 48 hours toward the next attack (27).
One functional imaging study examined patients during the preictal phase, defined by 12–48 hours before the head pain onset, and demonstrated a trend toward a higher activation of the spinal trigeminal nucleus compared to the ictal phase (2). A truly longitudinal study showed an activation of the hypothalamus up to 24 hours before the head pain started (3). The same study also showed an activation of the visual cortex during the first 24 hours of the postictal phase compared to the ictal phase (3). The results of these studies are summarized in Table 1.
Studies on experimentally provoked prodromes
Provoked attacks, as well as spontaneous attacks, can present with typical prodromes followed by head pain. Twelve out of 15 patients (80%) with typical migraine prodromes during spontaneous attacks developed similar prodromal symptoms after glyceryl trinitrate (GTN) infusion (7). These triggered prodromal symptoms developed approximately 1 hour after the GTN infusion, followed by the onset of headache approximately 1.5 hours later (2.5 hours after the infusion) (7). The same group reported that within an individual, the triggered prodromal symptoms are usually similar to the symptoms in spontaneous attacks (28). Another study using calcitonin gene-related peptide (CGRP) or pituitary adenylate cyclase-activating peptide-38 (PACAP38) only triggered prodromal symptoms in a minority of patients (2 of 25 patients) (8). Contrary to the spontaneous attacks (12), the preictal phase (prodromes without headache) in the provoked attacks was usually shorter (1 hour after trigger), but the time sequence (first prodrome, then headache) remained unchanged (7,8).
Migraine aura: A specific phase in migraine?
Blau proposed in 1980 that migraine aura is somewhat different from the other prodromes. In his original description, migraine aura stands for a phase which lasts for 15–30 minutes, immediately after the prodromal phase and right before the ictal phase (11). This idea has been widely adapted with certain variations (1). We did not include migraine aura as a separate phase for the following reasons: i) migraine with aura only accounts for approximately one-third of migraine patients (29); ii) even for migraine with aura patients, a majority of their migraine attacks are without aura. These patients actually have both migraine with and without aura (30); iii) migraine aura without headache is not rare; iv) aura does not necessarily develop “before” the headache, in some patients it accompanies the headache or may even start after the headache phase.
Limitations and required future studies
Most of the studies we reviewed represent only snapshots of different migraine phases. Longitudinal studies are needed to better understand the phasic transition of migraine. The issue of a typical prodrome followed by no headache was not covered by this narrative review. The biological meaning of these phenomena and whether they should be regarded as a (failed) migraine attack should be further discussed. It remains unknown how large the inter-personal or even the inter-attack difference of the preictal/postictal phase can be. One clear-cut definition (e.g. 48 hours) might not apply to all patients/attacks. Patients during the preictal phase usually receive no intervention. However, the effect of medication or intervention during the ictal phase may continue into the postictal phase, hence influencing the length of the postictal phase and/or possibly contributing to or affecting the symptomatology during the postictal phase. This needs to be taken into consideration in future studies.
Redefining the migraine phases
The preictal phase
Because of the different study designs, the inter-study difference remains large. The current definition of the preictal phase (up to 48 hours) in the ICHD-3 still applies to most of the studies reviewed. Although in a subset of patients or migraine attacks, the preictal phase might be longer; that is, up to 72 hours, the current definition of the preictal phase in the ICHD-3 should suffice.
The postictal phase
Studies, specifically physiological or functional imaging studies, focusing on this phase are scarce. Most studies showed that the postictal phase ended within 24 hours after the headaches had subsided. We therefore propose a renewed definition of the postictal phase which is up to 24 hours after the end of the ictal phase.
Summary
Even though the headache remains the key feature during the migraine attack, a migraine attack comprises a wider spectrum of symptoms and should encompass the preictal, ictal, and postictal phases. A clearer definition of the migraine phases is the first step towards a consensus regarding when a migraine starts and when it ends. A clearly defined time window allows for future studies to better explore the pathophysiological mechanism of migraine on a common ground.
Article highlights
The definition of the preictal and postictal phase varies between studies. Based on the clinical, physiological, and imaging evidence, the current definition of the preictal phase, up to 48 hours before the head pain onset, is sufficient. Based on the aforementioned evidence, we propose a renewed definition of the postictal phase, which lasts up to 24 hours after the end of the ictal phase; that is, the headache phase.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.