
Abstract
Migraine attacks are often preceded by premonitory symptoms. Prevalence rates of migraine patients reporting one or more premonitory symptoms show considerable variability and rates range between 12% and 79%. Sources of variability might be differences in study population or research design. Using a questionnaire, we retrospectively studied the prevalence of 12 predefined premonitory symptoms in a clinic-based population. Of 461 migraine patients, 374 (81%) responded. At least one premonitory symptom was reported by 86.9% and 71.1% reported two or more. The most frequently reported premonitory symptoms were fatigue (46.5%), phonophobia (36.4%) and yawning (35.8%). The mean number of premonitory symptoms per person was 3.2 (± 2.5). Women reported 3.3 premonitory symptoms compared with 2.5 symptoms in men (P = 0.01). Age, education, migraine subtype (with or without aura) and mean attack frequency had no effect on the mean number of symptoms per individual. In conclusion, premonitory symptoms are frequently reported by migraine patients. Sensitivity and specificity of premonitory symptoms for migraine need to be assessed using prospective methods.
Introduction
Migraine is a severe paroxysmal neurovascular disorder and considered a major cause of disability by the World Health Organization (1). The primary cause of a migraine attack is unknown but probably lies within the central nervous system (2). Prior to the start of the headache phase several non-headache symptoms (often called premonitory symptoms) are reported by migraine patients, such as changes in mood, behaviour and sensory perception (3). In a selected population migraine patients were able to predict an upcoming migraine attack well before the start of the headache phase (4). Prevalence rates of patients reporting one or more premonitory symptoms range between 12% (5) and 79% (6). One source of variability in prevalence rate might be differences in study population. In population-based studies rates range from 12% in migraine patients without aura to 18% in migraine patients with aura (5), whereas in clinic-based studies prevalence rates range from 33% (7, 8) to 79% (6). Other sources of variability might be differences in study design, such as preselection of patients or unclear definitions of premonitory symptoms.
In this study we assessed the prevalence of 12 frequently reported premonitory symptoms using a questionnaire in a large unselected clinic-based population and only symptoms preceding two or more out of three attacks were considered a premonitory symptom.
Methods
Migraine patients [diagnosed according to the criteria of the International Headache Society (IHS) (9)] from the Neurology out-patient clinic of the Leiden University Medical Centre received a questionnaire by mail. A reminder was send out to the patients who had not responded after 8 weeks.
The questionnaire addressed migraine characteristics, sociodemographic factors and possible premonitory symptoms. Migraine-related variables were: migraine subtype (migraine with or without aura according to the criteria of IHS (9)) and mean attack frequency per month in the last half-year. The following sociodemographic variables were included: age, sex and education in three categories: primary school or low vocational training, middle academic/vocational training, and higher academic/vocational training.
Twelve possible premonitory symptoms were included based on reports in the literature (3, 4, 8): concentration problems, depression, food craving, physical hyperactivity, irritability, nausea, phonophobia, fatigue, sleep problems, stressed feeling, stiff neck and yawning. For every possible premonitory symptom patients answered the question: ‘how often is a migraine attack preceded by this symptom?’. Answers were categorized as never, in < 1/3 of attacks, 1/3–2/3 of attacks or > 2/3 of attacks. Photophobia was not included in the questionnaire since co-occurrence of aura symptoms and visual hypersensitivity might introduce bias. The duration of the premonitory phase was not strictly defined. The local ethics committee had approved the study.
A symptoms was considered premonitory when it preceded at least 2/3 of migraine attacks. Prevalence of every premonitory symptom was calculated and presented as a percentage. The number of premonitory symptoms per individual was calculated and presented as mean (and SD). A difference in mean number of symptoms between subgroups was tested using the non-paired t-test (for sex and migraine subtype) or one-way
Results
The questionnaire was sent to 461 migraine patients; 374 (81%) responded. The characteristics of the study population are shown in Table 1. Forty-nine patients (13.1%) reported no premonitory symptoms, 86.9% of patients reported at least one symptom and 71.1% reported two or more (Fig. 1). The most frequently reported premonitory symptoms were fatigue (46.5%), phonophobia (36.4%) and yawning (35.8%) (Table 2). The mean number of premonitory symptoms reported per person was 3.2 (SD 2.5). Women reported a mean of 3.3 symptoms compared with a mean of 2.5 in men (P = 0.01). The effects of age, education, migraine subtype and mean attack frequency on the mean number of symptoms per individual were not statistically significant (Table 1). Of the migraine patients, 52% had migraine with aura (Table 1). No significant difference in premonitory symptoms was found between migraine subtypes (with and without aura) (Table 2).
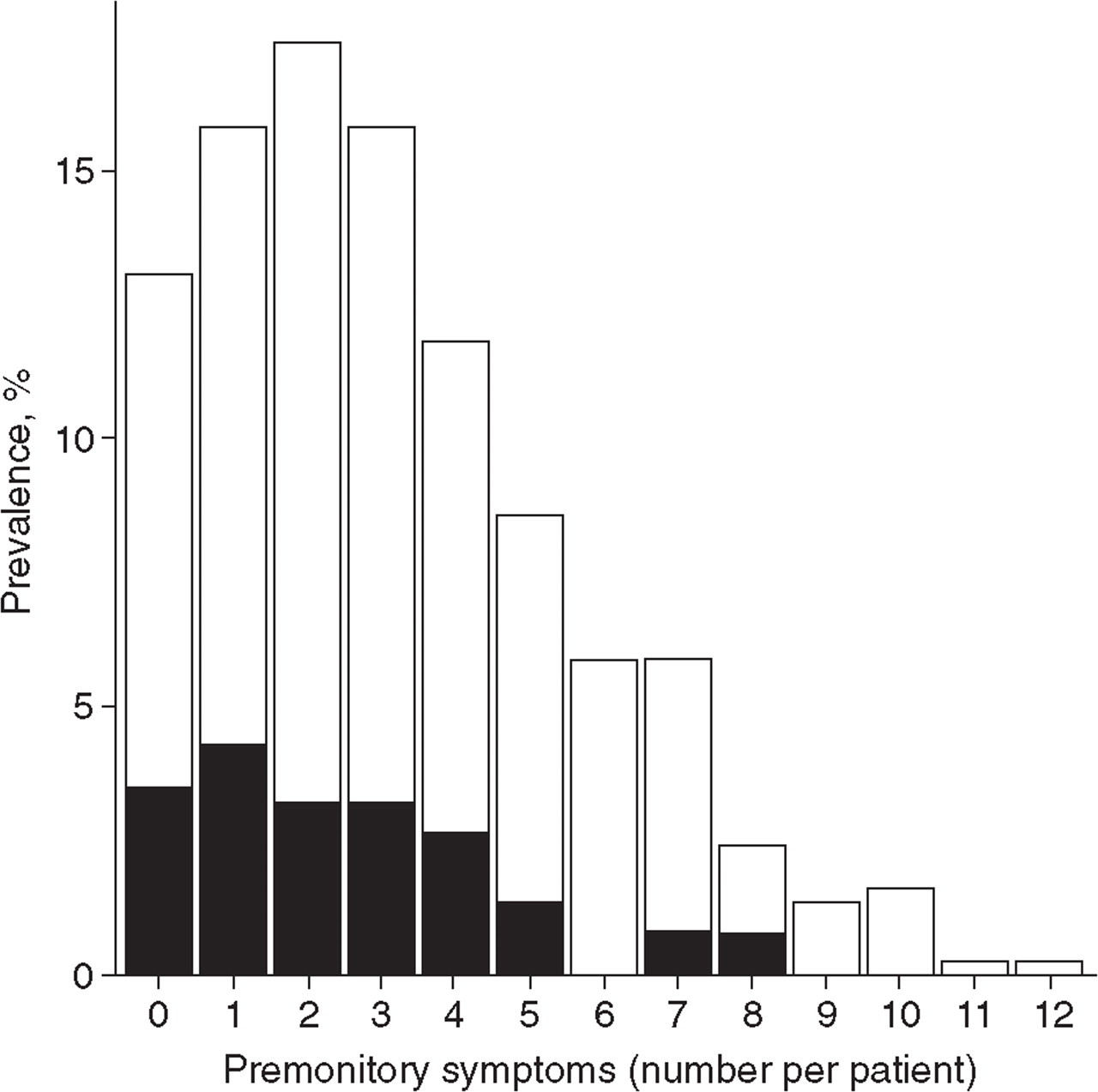
Number of premonitory symptoms per subject. ▪, Males; □, females.
Migraine and sociodemographic properties of all interviewed patients

Prevalence of premonitory symptoms

Prevalence is the percentage of patients of the total population (or subgroup) reporting a certain symptoms.
MoA, Migraine without aura; MA, migraine with aura.
The co-occurrence of symptoms is presented in Table 3. Depression and irritability showed the strongest correlation, followed by depression and concentration problems and depression and a stressed feeling.
Co-occurrence of premonitory symptoms: Spearman’s rank correlation coefficient matrix
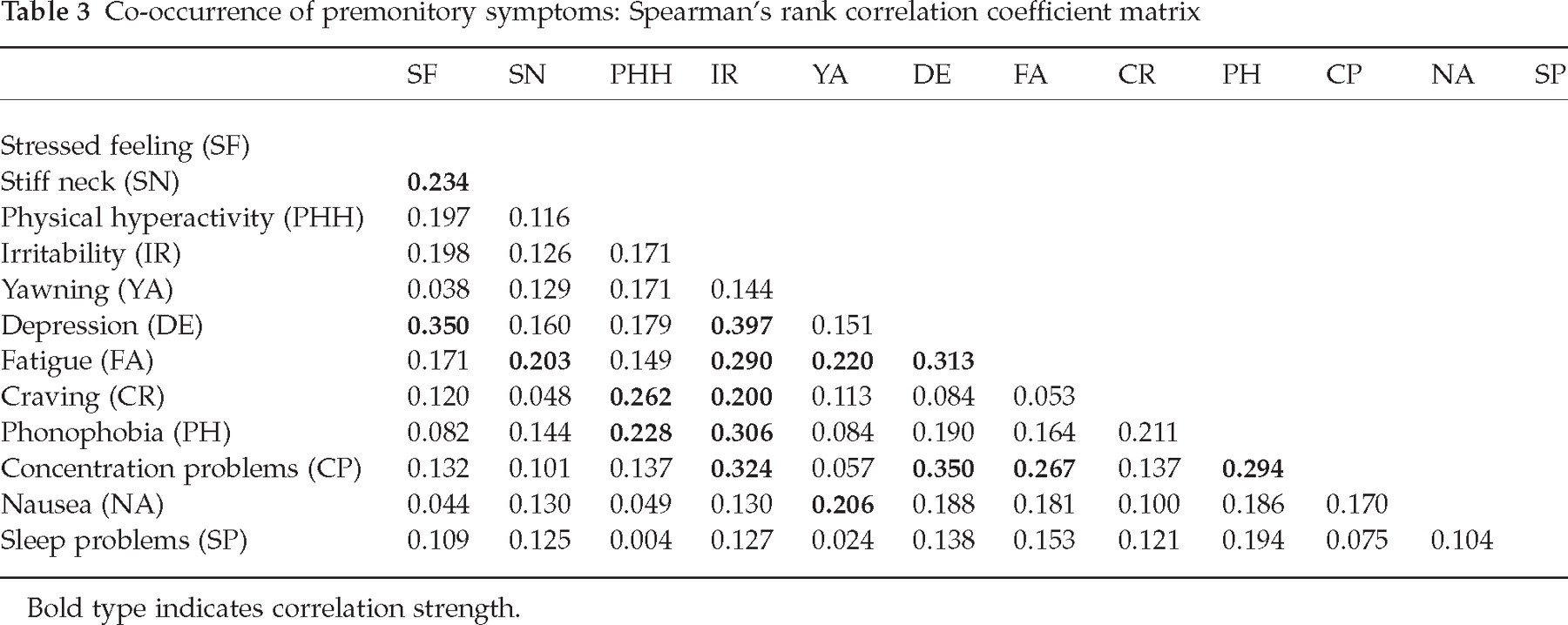
Bold type indicates correlation strength.
Discussion
The proportion of migraine patients reporting premonitory symptoms was high: 86.9% of patients reported at least one symptom. This high prevalence rate is comparable to one previous clinic-based study, where the rate was 79% (6), but in contrast to two other studies, where rates were about 33% (7, 8). Variability in rates might be explained by differences in study design such as preselection of patients (6) or differences in symptoms that are included in the questionnaire (8). Furthermore, the study of Amery (6) was conducted before the introduction of the IHS migraine criteria. Another source of variability might be the studied population. For example, prevalence rates in population-based studies have shown to be as low as 12% (5). It may be that patients identified in a population-based setting are not informed about premonitory symptoms in migraine and therefore are less aware of these symptoms. Fatigue was the most common premonitory symptom and the order of reported symptoms is comparable to a previous study in a selected population (4). In our study the percentage of patients presenting with aura was high. Patients with aura are more likely to consult a neurologist than those without aura and this difference might be increased due to the fact that all patients in the Netherlands see their general practioner first in case of complaints. However, no significant differences in premonitory symptoms were seen between migraine subtypes.
Females reported more premonitory symptoms than males. An overlap between premonitory symptoms and premenstrual syndrome may explain this difference (10). Furthermore, more females reported craving and nausea as premonitory symptoms compared with males. This is an interesting finding, since craving for chocolate and sweets is more common in females than in males (11). Nausea is also more frequently reported in females than in males in acute myocardial infarction (12) and after anaesthesia (13). The physiological basis for this gender difference is not clear. Besides gender differences, co-occurrence of premonitory symptoms within one subject was studied. The strongest associations were found between depression and symptoms such as irritability, concentration problems and fatigue. Co-occurrence of these mood symptoms might not be a coincidence, since they are all part of the DSM IV criteria for dysthymic disorder and major depression (14).
There might also be an overlap between premonitory symptoms and trigger factors in migraine. A migraine trigger is any factor that on exposure or withdrawal leads to the development of a migraine attack, whereas premonitory symptoms are a consequence of an ongoing attack. For example, mental stress (either the acute episode or the relief period after an acute episode) is often considered a trigger factor in retrospective questionnaires. However, it is unclear whether migraine attacks can be triggered in an experimental provocation study (15). So, it could be that mental stress triggers a migraine attack or that patients perceive more mental stress because they are in the premonitory phase of a migraine attack. Future prospective diary studies or experimental studies are needed to address this question.
This study, as well as other retrospective studies assessing premonitory symptoms in migraine, has some limitations. First, the list of possible premonitory symptoms is based on previous studies (3, 4, 8) and may seem somewhat arbitrary. To be complete, a study should include a full exploration of all possible symptoms associated with a migraine attack. Second, non-responders may have introduced some bias. However, the response rate was 81% and there were no differences in age, sex or migraine subtype between responders and non-responders (data not shown). Third, when should a symptom be classified as a premonitory symptom? We excluded photophobia as a premonitory symptom, but it could be argued that phonophobia and nausea are actually part of the headache phase and therefore not premonitory symptoms. Furthermore, in this study we considered symptoms as premonitory if two-thirds of attacks were preceded by this particular symptom. In order to assess the sensitivity and specificity of individual premonitory symptoms for migraine attacks, possible premonitory symptoms and migraine attacks need preferably to be studied prospectively (4, 16). Also, the temporal relationship between possible premonitory symptoms, aura and the occurrence of headache needs to be assessed in a prospective design.
In conclusion, premonitory symptoms are frequently reported by migraine patients. Sensitivity and specificity of premonitory symptoms for migraine need to be assessed using prospective methods.
Footnotes
Acknowledgements
This study was supported by the Netherlands Organization for Scientific Research (grant 940-38-029).