
Abstract
Background
In literature, osmophobia is reported as a specific migrainous symptom with a prevalence of up to 95%. Despite the International Classification of Headache Disorders 2nd edition proposal of including osmophobia among accompanying symptoms, it was no longer mentioned in the ICHD 3rd edition.
Methods
We conducted a prospective study on 193 patients suffering from migraine without aura, migraine with aura, episodic tension-type headache or a combination of these. After a retrospective interview, each patient was asked to describe in detail osmophobia, when present, in the following four headache attacks.
Results
In all, 45.7% of migraine without aura attacks were associated with osmophobia, 67.2% of migraineurs reported osmophobia in at least a quarter of the attacks. No episodic tension-type headache attack was associated with osmophobia. It was associated with photophobia or phonophobia in 4.3% of migraine without aura attacks, and it was the only accompanying symptom in 4.7% of migraine without aura attacks. The inclusion of osmophobia in the ICHD-3 diagnostic criteria would enable a 9.0% increased diagnostic sensitivity.
Conclusion
Osmophobia is a specific clinical marker of migraine, easy to ascertain and able to disentangle the sometimes challenging differential diagnosis between migraine without aura and episodic tension-type headache. We recommend its inclusion among the diagnostic criteria for migraine as it increases sensitivity, showing absolute specificity.
Introduction
Scientific literature that analyse osmophobia in the differential diagnosis between migraine and episodic tension type headache.
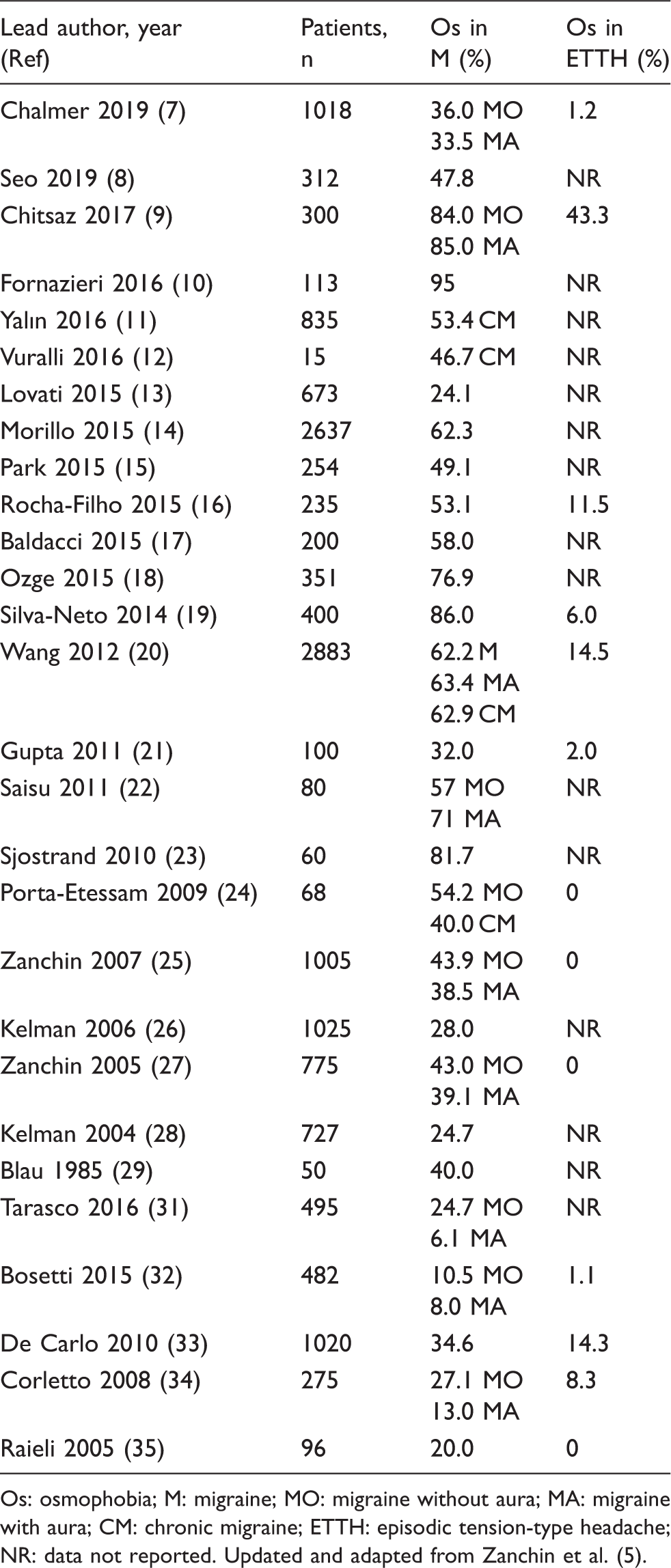
Os: osmophobia; M: migraine; MO: migraine without aura; MA: migraine with aura; CM: chronic migraine; ETTH: episodic tension-type headache; NR: data not reported. Updated and adapted from Zanchin et al. (5).
As a result, the Canadian and Italian Societies for the Study of Headaches proposed Os as an additional criterion of M diagnosis (37–38). In 2004, the International Classification of Headache Disorders 2nd edition (ICHD-2) proposed a modified version of criterion D for MO diagnosis in the Appendix (A1.1 criterion D. During headache at least two of the following: 1) nausea; 2) vomiting; 3) photophobia; 4) phonophobia; 5) osmophobia) (39). In the following 2013 ICHD-3 beta criteria, Os was deprived of any diagnostic value and considered a mere accompanying symptom (40); eventually, discomfort from smells completely disappeared from ICHD-3, without any explanation (1).
The main goal of this study was to analyse Os in M versus ETTH adult patients, controlling the recall bias through a prospective survey. Our aims were: (i) to ascertain the prevalence of Os in MO, MA and ETTH; (ii) to characterise the clinical features of Os; (iii) to evaluate the diagnostic usefulness of Os in the differential diagnosis between MO and ETTH, in terms of sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV); (iv) to explore the diagnostic gain of a revised set of criteria including Os.
Materials and methods
We performed a prospective clinical study on a series of patients referred to our Headache Centre from December 2013 to June 2014, with diagnoses of primary headaches fulfilling the ICHD-3 beta criteria. We focused on patients suffering from episodic M, divided into MO and MA, and ETTH, including people with more than one type of primary headache (MO and ETTH, MA and ETTH, MO and MA). Patients were consecutively recruited among subjects who came for the first time to our Headache Centre. Exclusion criteria included: age <16 years; CM; recent onset of headache (<6 months prior to study inclusion); a previously established olfactory dysfunction due to neurological disorders (e.g. Parkinson's disease, Alzheimer's dementia, epilepsy, stroke); head trauma, and chronic rhinosinusitis. For each patient, we recorded a thorough medical history through a semi-structured questionnaire. A general and neurological examination, laboratory and/or instrumental exams excluded secondary causes of the headache. Once the diagnosis had been achieved, we performed a semi-structured interview to evaluate retrospectively the presence of Os during headache (patients with more than one type of primary headache were excluded from the retrospective questionnaire) and its features. The frequency of Os; the time of Os occurrence in the individual headache history; the time of Os manifestation in relation to the pain phase, the duration of Os with respect to the headache attack and the types of smells that were referred as unbearable were inquired about and recorded. We asked the patient how often an olfactory stimulus triggered the attack, and the specific smell responsible. In the second phase of our study, all the patients received a prospective semi-structured questionnaire, independent of the reported experience of Os. Through this form, we invited the patients to describe in detail the four forthcoming headache attacks, focusing on headache pattern, associated symptoms, and Os features. A physician in our group clearly explained to the patient the content and the purpose of the questionnaire and the meaning of the symptom Os, defining it as an unbearable perception, during a migraine attack, of smells that are non-aversive or even pleasant outside the attack. We asked our patients to fill in the questionnaire within the same day as the headache attack, in order to minimise recall bias. All patients had given written informed consent to the scientific use of their clinically acquired anonymous data. We analysed the association of Os with other accompanying symptoms, in order to verify the diagnostic gain of different proposed versions of ICHD criterion D for diagnosis of M. We referred to the appendix of ICHD-2, “at least two of the following: (1) nausea; (2) vomiting; (3) photophobia; (4) phonophobia; (5) osmophobia” (39); the suggested revision by Wang et al., “Nausea and/or vomiting or two among osmophobia, photophobia, or phonophobia” (20), or the suggestion from Silva-Neto et al., “at least one of the following: (a) nausea and/or vomiting; (b) photophobia and phonophobia; and (c) osmophobia” (41).
Statistical analysis was performed using Pearson χ2 test and analysis of variance (ANOVA). McNemar χ2 test was used for comparisons in dependent samples, while t-test was used to compare means in independent samples. The level of statistical significance was set at p <0.05. In addition, sensitivity, specificity, positive and negative predictive values and odds ratio were calculated for each different accompanying symptom.
Results
Study population. Number of patients, attacks, age and sex differences according to different diagnosis of primary headaches.

MO: migraine without aura; MA: migraine with aura; ETTH: episodic tension-type headache.
Os emerged as a very common symptom among migraineurs. With regard to the prospective data, 45.7% of all the attacks reported by MO patients were associated with Os (234/512). The percentage was the same among MA patients (45%, 9/20) and among MA plus MO patients (46.4%, 13/28). Above all, none of the 124 ETTH attacks was accompanied by Os, while among MO plus ETTH patients Os exclusively occurred in headache with typical migrainous features (Figure 1). In MO patients, Os showed a sensitivity of 45.7% and a specificity of 100%, a positive predictive value of 100% and a negative predictive value of 30.9% (Table 3).
Prevalence of osmophobia + attacks (on the left) and osmophobia + patients (on the right), in primary headaches. Data refer to prospective questionnaire. Diagnosis of migraine: sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and odds ratio (OR) of each accompanying symptom (according to criterion D of ICHD-3) and of every couple of symptoms, including Os. Data obtained through a comparison between patients with migraine without aura and those with episodic tension-type headache.

Interesting data derive from the analysis of the set of four consecutive attacks described by each patient. In all, 67.2% (86/128) of MO patients reported Os in at least one of the four attacks; 60% (3/5) of MA patients reported Os, as well as 6/7 (85.7%) of patients with MO plus MA. The mean duration of attacks with Os was 12.3 ± 17.3 hours, while the attacks without Os lasted 6.6 ± 8.3 hours (p <0.000001). Os usually started together with the onset of the pain phase or during its course, and it ended before or together with the end of headache (see Tables 4 and 5 for detailed data). Regarding annoying smells, perfumes were reported in 69.2% (162/234) of MO attacks, followed by cigarette and/or cigar smoke (56.4%, 132/234) and by food (56.0%, 131/234). Other smells were reported in 24.4% (57/234) of MO attacks (Figure 2). A subgroup of patients experiencing Os during headache reported migrainous attacks triggered by smells (9.3% of attacks with Os).
Categories of smells reported as annoying during migraine without aura attacks, according to our prospective analysis. Data in percentages, with respect to the osmophobia + attacks. Onset of osmophobia with respect to the pain phase. Data refer to prospective analysis on patients with MO or MA. MO: migraine without aura; MA: migraine with aura. End of osmophobia with respect to the end of the pain phase. Data refer to prospective analysis on patients with MO or MA. MO: migraine without aura; MA: migraine with aura.


Focusing on patients with MO (512 attacks), we compared the pain pattern of Os-associated headaches (n = 234) to one of the attacks without Os (n = 278). MO attacks with Os were characterised by a throbbing headache in 59.4% (139/234), severe intensity in 53.8% (126/234), unilateral pain in 83.8% (196/234) and aggravation by routine physical activity in 82.1% (192/234) of cases. MO attacks without Os were reported as throbbing in 40.7% (113/278), severe in intensity only in 29.1% (81/278), unilateral in 65.1% (181/278), and aggravated by physical activity in 72.3% (201/278) of attacks (Figure 3).
Comparison between migraine without aura attacks with osmophobia (Os) and migraine without aura attacks without osmophobia in the prospective analysis, as regards clinical features.
Considering the 86 patients who reported Os in at least two of the four attacks (69 MO, three MA, nine MO + ETTH, one MA + ETTH and three MO + MA), we found a strong stereotypy as regard to the combination of odours perceived as unbearable: 34% (29/86) reported the same association of odours twice, 20% (17/86) reported it in 3/4 attacks, 17% (15/86) described the same annoying smells during all the attacks included in the prospective questionnaire.
The data from the retrospective questionnaire refer to a lower number of patients (n = 154) (patients with more than one type of primary headache were excluded and data regarding 10 patients were lacking or incomplete). Os was an intrinsic feature of migrainous headache: it was present from the beginning of the patient's headache history in 84.2% (64/76) of MO patients). Os was present in at least five of 10 attacks in 76.3% (58/76) of patients with MO (Figure 4). These data confirm a previous retrospective study (25).
Frequency of osmophobia recurrence over 10 migraine without aura (MO) attacks (10/10; from 5 to 9 out of 10; less than 5 times out of 10), according to retrospective interview. Comparison with the previous data of our group (25). Data in percentages.
Considering criterion D of ICHD-3, we analysed only patients with pure MO or ETTH, excluding MA (because of few data) and patients with more than one primary headache, in order to have more homogeneous data. Among MO attacks, nausea showed a sensitivity of 43.2% and a specificity of 87.9%, both lower than those regarding Os. The positive predictive value (PPV) for nausea was 93.6%, while its negative predictive value (NPV) was 27.3%. Compared with nausea, photophobia had higher sensitivity (63.1%), specificity (88.6%), PPV (95.9%) and NPV (36.6%), similarly to phonophobia. All these symptoms revealed a statistically significant difference in their distribution between MO and ETTH, as confirmed by the values of their odds ratio (OR) in this analysis (Table 3). The logistic regression used to verify these results in a multivariate analysis confirmed the association of nausea (p = 0.002), photophobia (p <0.001) and phonophobia (p <0.001) with MO, unlike vomiting (p = 0.77). Furthermore, we assessed sensitivity, specificity, PPV, NPV and OR of the different couples of accompanying symptoms. As vomiting usually accompanies nausea, the sensitivity of the couple nausea-vomiting remains low (45.7%). Nausea-photophobia showed a higher sensitivity (74.4%) but a lower specificity (78.7%), similarly to the couple nausea-phonophobia. Instead, the association nausea-Os gains in sensitivity (64.3%), with a high specificity (87.9%) and high PPV (95.6%). The associations photophobia-Os and phonophobia-Os show a better sensitivity (74.8% and 74.2% respectively) together with a high specificity (88.6% and 87.1% respectively) and a very high PPV (96.5% and 96.0% respectively), representing the best available diagnostic accuracy. As McNemar χ2 test confirmed, the inclusion of Os among accompanying symptoms significantly improves the diagnosis of MO versus ETTH (p <0.0001) (Table 3).
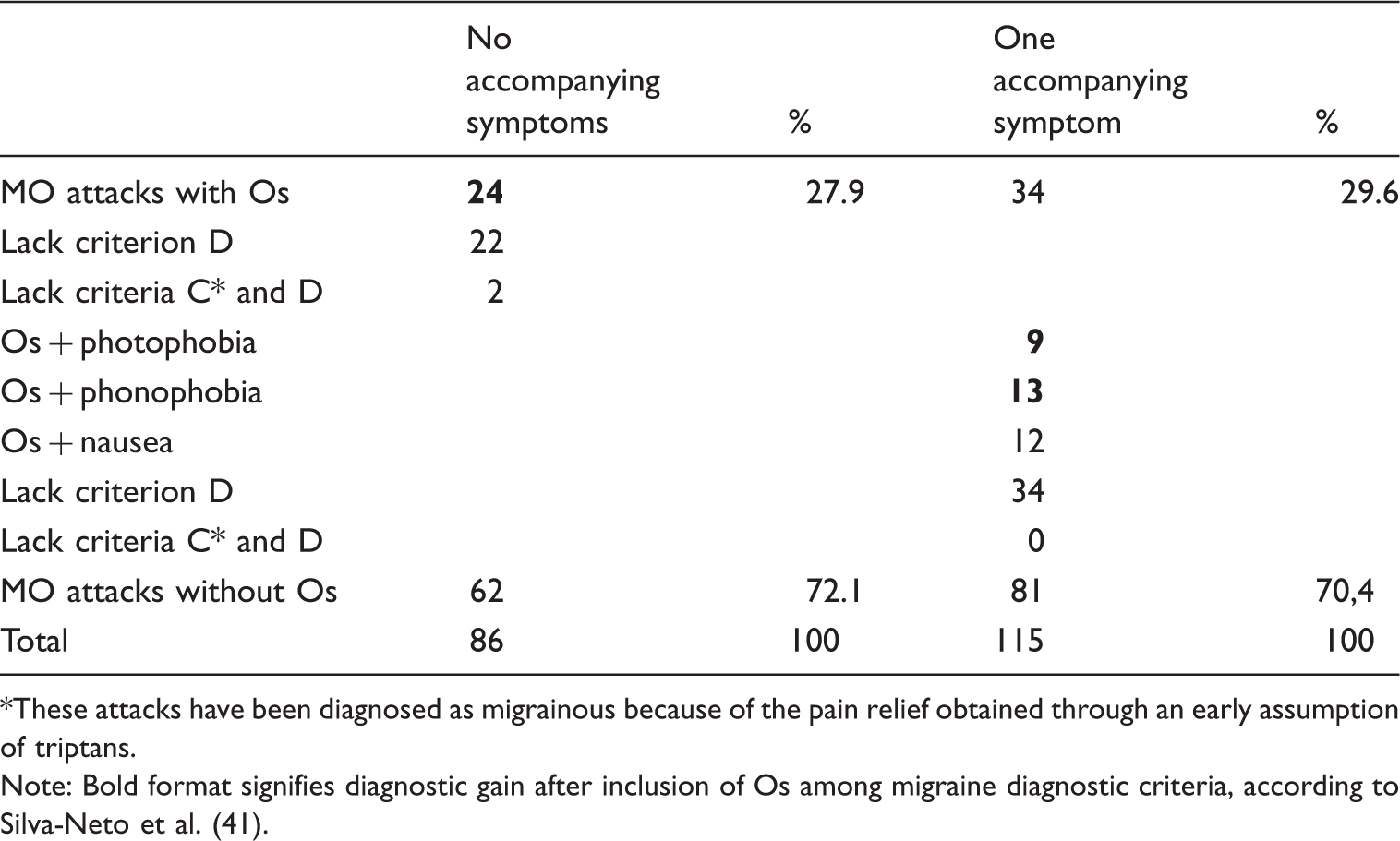
Figure 5 unveils the remarkable relation between Os and the number of accompanying symptoms (see criterion D for the diagnosis of MO, according to ICHD-3), in patients suffering from pure MO (128 patients). Os prevalence increases in parallel with the number of accompanying symptoms. Due to the well-known recommendation of taking migraine-specific acute medication at the onset of the pain phase, Os sets at an outstanding 27.9% (24/86) among MO attacks with no other hypersensitivities or nausea/vomiting (considered as migrainous headache because of the pain pattern and the efficacy of migraine-specific acute treatments). It increases to 96.9% among MO attacks with all four accompanying symptoms of criterion D, passing through an Os prevalence of 29.6% among MO with one accompanying symptom (34/115). Considering the MO attacks accompanied by Os and no other symptoms, 22/24 fulfilled all the ICHD-3 diagnostic criteria for MO except for criterion D, while 2/24 did not fulfil the C and D criteria, but clearly responded to an early triptan medication. Again, among patients suffering from pure MO, nine attacks reported Os with photophobia (7/9 fulfilled all diagnostic criteria except D, 2/9 rapidly resolved with triptans), 13 had Os with phonophobia and no other symptoms (they fulfilled all diagnostic criteria except for criterion D) (Table 6).
Percentages of osmophobia (Os) prevalence along with the increasing number of accompanying symptoms, composing criterion D of ICHD-3 (data refer to 128 patients with migraine without aura). Distribution of osmophobia among migraine without aura attacks with no other accompanying symptoms (referring to those included in criterion D of ICHD-3 for migraine without aura diagnosis) or among migraine without aura attacks with only one out of four accompanying symptoms. These attacks have been diagnosed as migrainous because of the pain relief obtained through an early assumption of triptans. Note: Bold format signifies diagnostic gain after inclusion of Os among migraine diagnostic criteria, according to Silva-Neto et al. (41).
Discussion
The intrinsic structure of ICHD-3 diagnostic criteria of MO and TTH allows a diagnostic overlap (1): moderate intensity, duration of pain, shared symptoms such as photo- or phonophobia may complicate the differential diagnosis between MO and TTH. According to some authors, such diagnostic challenge could be faced by looking at the unilaterality of pain, pulsating pain quality, and exacerbation with physical activity for the diagnosis of MO (4), or considering the different instinctive manoeuvres adopted by M and TTH patients (42). In this clinical scenario, our prospective study suggests Os as that long-desired pathognomonic clinical criterion for diagnosis of M versus TTH.
Os was present in 45.7% of the attacks described by our patients with MO, while it has never been reported during ETTH, neither in tension-type headaches attacks of patients suffering from MO and ETTH or from MA and ETTH. 67.2% of patients with MO reported Os in at least one of the four prospectively analysed attacks. This prevalence is higher than those reported in previous retrospective studies from our group (43% and 43.9%) (25,27), and similar to those reported by Morillo and Wang (14,20). If we consider as osmophobic also those MO patients who reported Os at the retrospective interview without reporting it in the prospective questionnaire (11/76), Os results as part of the migrainous pattern in 75.8% of MO patients (97/128). This retrospective-prospective difference may be due to the limited number of M attacks studied in the prospective phase, to the variability of migrainous pattern, and to the circumstantial absence of relevant olfactory stimuli in the environment. Our prevalence data confirm the adjunctive value of a prospective attitude in revealing an under-reported symptom (43). Among migrainous patients who had denied Os in the retrospective investigation, 26.9% reported Os in at least one of four attacks in the prospective questionnaire (14/52). However, in our study, Os prevalence is lower than that reported by some authors (10,19). Motivations may be found in the variability of the individual migraine pattern, in the limited number of prospectively studied attacks and in an early assumption of the acute treatment determining a non-neglectable abortiveness rate of accompanying symptoms (Os appeared during the pain phase in half of cases).
The data from our prospective study confirmed the results of our previous retrospective study (25): 84% of M patients experienced Os from the beginning of their headache history. Os developed at the beginning of the attack in 40% of patients or during the attack in 50%. Os anticipated the occurrence of pain in 9% of cases, often reported by patients as olfactory-triggered attacks (43% of these cases). Os stopped with the pain phase in 45% and before the end of it in 47% of cases. In our sample of patients, the attacks with Os were more frequently characterised by a typical migrainous pain pattern, with respect to those without Os. We observed a consistent stereotypy in the specific features of Os, with 71% of patients reporting a recurrence of the specific combination of annoying smells and 76% of patients describing the same phase of appearance of Os during the attacks.
The comparison between retrospective and prospective questionnaires demonstrate that patients may have difficulty recalling Os. On one hand, 26.9% (14/52) of patients who denied suffering from Os at the retrospective evaluation reported Os at least once in the prospective analysis; on the other hand, 14.5% (11/76) of patients who had experienced Os in their migraine history did not report Os in the prospective questionnaire. These controversial data are probably due to the low number of attacks analysed in the prospective phase and to the low availability of smell stimuli with respect to other main sensory modalities.
Our study has not been designed as a field-testing of an Os-including new diagnostic criterion. However, the analysis of the different combinations of accompanying symptoms during M attacks conveys relevant evidence to support the inclusion of Os among M diagnostic criteria. Differently from what has recently been reported on this topic (7), among MO attacks characterised by only one of the four accompanying symptoms included in diagnostic criterion D, Os was present in 30% of cases (34/115), nine times in association with photophobia and 13 times in association with phonophobia (Table 6). Most striking, among MO attacks with no associated symptoms among those composing criterion D (these headaches had been considered as MO because of the pain pattern and the efficacy of migraine-specific acute treatments), 28% were accompanied by Os (24/86). Os is easily assessable and probably should be the first accompanying symptom to ask for, in front of a patient suffering from primary headache: it appears as a valuable symptom in daily clinical activity and a specific clinical marker of M (5). If included among the diagnostic criteria, Os will enable physicians to increase their diagnostic sensitivity for M (versus TTH). In order to reach the maximum diagnostic accuracy, we believe that the proposal of a revised criterion D by Silva-Neto et al. (41) would be appropriate. Criterion D revisions according to the ICHD-2 Appendix version or Wang's proposal would include attacks with Os and photophobia, or with Os and phonophobia (4.3% of our cases, 22/512); both would not include attacks with Os alone (4.7% of cases in our study, 24/512). Moreover, the ICHD-2 version excludes attacks with nausea and without another accompanying symptom (5.3% of our cases, 27/512). On the contrary, the proposal of “At least one of the following: (a) nausea and/ or vomiting; (b) photophobia and phonophobia; (c) osmophobia” (41), will allow the diagnosis of MO to be achieved with isolated Os as well, without excluding any previously migraine-diagnosed patients. It would enable a total of 9.0% (46/512 attacks) increased sensitivity of criterion D in our case series. With regard to the proposal for the inclusion of a new item concerning smell-triggered attacks (41), in our opinion it seems unnecessary, as in our case series Os characterises all the olfactory stimuli-triggered attacks (reported at least once by 7.8% of MO patients [10/128]).
Main limitations of our study can be found in the number of attacks analysed in the prospective phase (four), in the exclusion of CM, in the limited number of patients included and in the intrinsic design of the study, which was not specifically structured to perform a complete field testing of the different proposals of criterion D for diagnosis of M. Nevertheless, the results from our prospective survey point to Os as a highly specific migrainous symptom, extremely useful in the differential diagnosis between M and TTH, in line with the literature (5). Different from several previous studies (7,9,16,19,20,21), no ETTH patients experienced Os. Two-thirds of MO patients experienced aversion to smell, with even higher expected prevalence in the case of a long-time prospective observation. Patients generally have low awareness of Os; it is usually associated with other typical migrainous features such as nausea, vomiting, phono- or photophobia, but we demonstrated that Os might be isolated as well, or accompanied by only photophobia or phonophobia.
Conclusions
Osmophobia is a specific clinical marker of migraine, simple to ascertain and able to disentangle the sometimes challenging differential diagnosis between migraine without aura and tension-type headache. Our prospective study confirms its high prevalence, with an absolute specificity. With the limitations of a study not designed to perform a field testing of diagnostic criteria, we suggest that osmophobia may increase diagnostic sensitivity towards migraine. We therefore recommend the inclusion of Os among the diagnostic criteria for migraine, hopefully with the same authority as other main accompanying symptoms. Our raw data of 9% gain in diagnostic sensitivity needs to be verified through a large field-testing study on probable tension-type headache and probable migraine patients.
Article highlights
Osmophobia is a highly specific migrainous symptom, extremely useful in the differential diagnosis between migraine and tension-type headache. In our prospective study, two-thirds of migraine without aura patients experienced aversion to smell at least once in a series of four consecutive attacks, while it was never reported in association with episodic tension-type headache. Usually associated with other typical migrainous features such as nausea, vomiting, phono- or photophobia, osmophobia may develop with no other accompanying symptoms, or it may be associated with photophobia or with phonophobia in 9.0% of migrainous attacks. We recommend the inclusion of osmophobia among the diagnostic criteria for migraine, as it may increase sensitivity, keeping absolute specificity.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.