
Abstract
Background
Neuroimaging for headache commonly exceeds published guideline recommendations and may be overutilized.
Methods
We conducted a retrospective cross-sectional study of all outpatient community patients at Mayo Clinic Rochester who underwent a neuroimaging study for a headache indication in 2015. We assessed the neuroimaging utilization pattern, clinical application of red flags, and concordance with neuroimaging guidelines.
Results
We identified 190 outpatients who underwent 304 neuroimaging studies for headache. The median age was 46.5 years (range 18–91 years), 65% were female, and most reported no prior history of headache (n = 97, 51%). A minority of patients had prior brain imaging studies (n = 44, 23%) and neurological consultations for headache (n = 29, 15%). Few studies were ordered after consultation with a neurologist (n = 14, 7%). Seventy-seven percent of patients were documented to have a “red flag” justifying the imaging study. Abnormal neuroimaging findings were found in 3.1% of patients with warning flags (5/161); carotid dissection (n = 3) and reversible cerebral vasoconstrictive syndrome (n = 2). An estimated 35% of patients were imaged against guidelines.
Conclusions
The prevalence of serious causes of headache in a community practice was low despite the presence of a documented red flag symptom. Inadequate understanding or application of red flags may be contributing to recommendations to image patients against current guidelines. Interventions to reduce unnecessary neuroimaging of patients with headache need to be designed and implemented.
Background
The cost of neuroimaging for headache evaluation is an estimated $1 billion annually in the United States (1), which is greater than the annual total Medicare reimbursement to neurologists for non-procedural care ($686 million) (2). Over five years, approximately 40% of patients with headache undergo neuroimaging, which frequently does not reveal a serious cause of headache (1,3,4). Neuroimaging studies not uncommonly reveal incidental findings leading to unnecessary worry and follow-up testing (5). Optimizing adherence to clinical practice guidelines with respect to neuroimaging for headache highlights an opportunity to improve high value care for headache patients (1,6–12).
“Red flags” are clinical warning signs or symptoms that suggest the need for neuroimaging studies to diagnosis secondary causes of headache. Some guidelines and investigators also describe “yellow” (13) or “orange” flags (14) (e.g. headache awakening from sleep, new onset of unilateral headache, and postural headaches) (13) in an attempt to stratify the risk of non life-threatening secondary causes of headache. Identification of warning flags to guide neuroimaging decisions is recommended (13–15), but their use and application in a clinical practice is incompletely understood. These flags have largely been established by expert opinion without clear consensus published in the literature. Furthermore, the pretest probability of a neuroimaging abnormality for each red flag is not known, with the exception of “thunderclap headache”, which carries a high risk for a serious abnormality (16).
The approach and impact of applying warning flag definitions to trigger neuroimaging in a community outpatient practice has not been well studied. Furthermore, warning flags may be open to interpretation, and it is not known whether primary care providers and neurologists would agree upon the presence or absence of a warning flag in the clinical history. Advancing our understanding of the clinical decision-making and use of headache warning flags in a community practice and whether clinicians are following neuroimaging guidelines would help inform the design of practice models that may reduce unnecessary imaging, increase appropriate imaging, and improve the overall value of care for patients with headache.
Our primary aims were to perform: a) a descriptive analysis of neuroimaging patterns in a community based primary care practice with respect to practice guidelines and commonly suggested indications (i.e. red flag symptoms); and b) a descriptive analysis of the rate of symptomatic neuroimaging findings.
Methods
We conducted a retrospective cross-sectional study of adult patients impaneled in the Employee and Community Health practice at Mayo Clinic, Rochester, MN. Employee and Community Health is a primary care medical home that includes the divisions of Primary Care Internal Medicine and the departments of Family Medicine. Employee and Community Health provides medical care to approximately 155,000 patients residing in and around Olmsted County, Minnesota. All patients are assigned a physician, nurse practitioner, or physician assistant as their primary care provider. The Integrated Community Neurology clinic supports the medical home providing curbside, electronic, and face-to-face consultations (17). This study was approved by the Mayo Clinic Institutional Review Board.
Patient ascertainment
Within the Employee and Community Health population, we identified all patients within a claims database who underwent a neuroimaging study with a primary ICD-9 and ICD-10 code for a primary headache disorder in 2015. Only patients seen in the outpatient setting who underwent a neuroimaging study for headache were included. Patients were excluded if the neuroimaging study occurred in the emergency department or hospital, the neuroimaging was conducted to follow up on a known condition causing a secondary headache, or the neuroimaging was recommended for a primary reason other than headache as determined by retrospective chart review. All neuroimaging studies were interpreted by neuroradiologists at our institution.
Data collection
Patient demographics, headache presentation, ordering provider, documentation of presence or absence of “red flags” (15,18) and “yellow flags” (13) were collected. The “red flags” assessed were anticoagulation, trauma, systemic symptoms or comorbidities (fever, weight loss, night sweats, cancer, immunosuppression, or infections), neurological symptoms or signs, thunderclap onset, new headache onset age >50 years, new or different headache than previous headaches, progressively worsening headache, precipitation of headache by Valsalva maneuver, postural headache, and pregnancy. The “Yellow Flags” assessed were headache awakening at night, new onset unilateral headache, “worst headache of life”, and headache persistence. The frequency of warning flags was calculated and a subgroup analysis of the most common warning flags was performed with a focus on potential opportunities to avoid neuroimaging.
Patients were classified according to The International Classification of Headache Disorders, 3rd edition (beta version) (ICHD-3 beta) (19) based on retrospective chart review performed by a neurologist (NPY). If a headache did not clearly meet criteria for migraine, tension-type, or cluster headache it was classified as headache not otherwise specified (NOS). The neuroimaging studies performed and symptomatic abnormalities were summarized. Non-specific T2 signal abnormalities were not included in the summary of incidental imaging abnormalities.
Guideline recommendations
Patients with a diagnosis of a primary headache disorder, normal neurological examination and absence of a red flag were determined to be imaged against guideline recommendations (6–11).
Results
Population summary
Within the total Employee and Community Health population, 3281 unique adult patients were evaluated for a headache in a total of 5072 visits with an average of 1.5 visits per patient per year. Eighty percent of unique patients (2622/3281) and 85% of total headache visits (4324/5072) occurred in the outpatient setting. The most common primary diagnoses based on billing code for all visits were migraine (46.6%), headache NOS (45.2%), tension (5.4%), cluster (0.9%), post traumatic (0.9%), other (0.7%), and new daily persistent headache (0.4%). Neuroimaging studies were performed on 490 patients. The majority of neuroimaging studies were performed in the emergency department or inpatient setting (n = 265, 54.1%), in the outpatient setting for patients with known secondary causes of headache requiring follow up imaging (n = 14, 2.9%), or for primary indications other than headache (n = 21, 4.3%). The remaining studies were performed on outpatients with an unclear cause of headache (n = 190, 38.7%) which comprise the cohort for this study. The overall rate of neuroimaging study per unique outpatient was 7.2% (190/2622) and the rate of neuroimaging per all outpatient headache visits for the population was 4.4% (190/4324).
Clinical presentation
Characteristics of patients undergoing neuroimaging (n = 190).

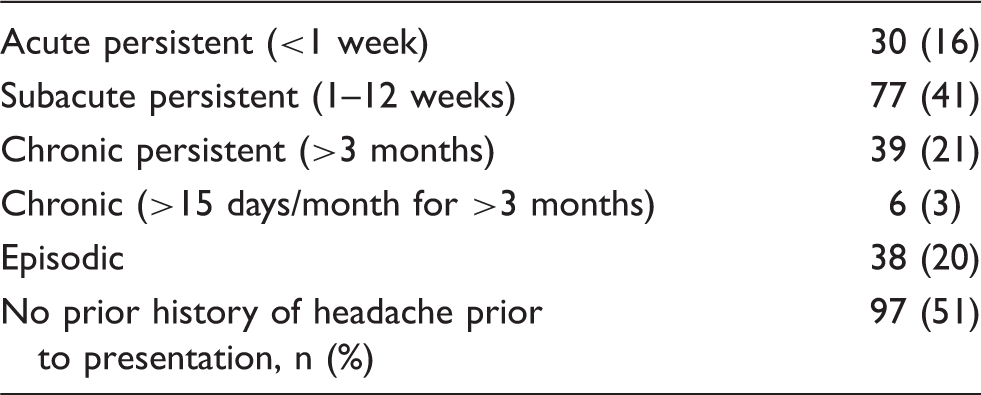
Clinical course of headache prior to neuroimaging (n = 190).
Of 190 patients, 64 presented with symptoms other than headache including dizziness (n = 25, 33.8%), visual disturbance (n = 23, 31.1%), sensory syndrome (n = 18, 24.3%), cognitive changes (n = 13, 17.6%), nausea (n = 13, 17.6%), aphasia (n = 7, 9.5%), gait ataxia (n = 6, 8.1%), weakness (n = 6, 8.1%), and vomiting (n = 1, 1.4%). These symptoms were likely due to migraine aura in 13/64 (20.3%) of patients. Most patients had a normal neurological examination documented by the primary care provider (n = 180, 94.7%) with 29% of the normal examinations confirmed by a neurologist. Of the patients with an abnormal examination, all had known non-headache related explanations for their examination abnormalities, such as a known prior stroke.
Neuroimaging
Neuroimaging studies were ordered by primary care physicians (n = 125; 66%), advanced practice providers (n = 35; 18%), and neurologists (n = 30, 16%). The imaging studies performed included brain magnetic resonance imaging (MRI) (n = 104, 54.7%), head computed tomography (CT) without contrast (n = 98, 51.6%), brain magnetic resonance angiography (MRA) (n = 62, 32.6%), neck MRA (n = 31, 16.3%), brain magnetic resonance venography (n = 4, 2.1%), head CT angiogram (n = 3, 1.6%), brain CT venography (n = 2, 1.1%), and neck CT angiogram (n = 2, 1.1%). Only five studies (2.6%) revealed an acute abnormality that would explain the presence of symptoms.
Red and yellow flags
Documented red and yellow flags (n = 190)*.

Patients may have more than one red or yellow flag.
Abnormal neuroimaging findings and presentation
All five cases with abnormal neuroimaging had a documented red flag. Two patients diagnosed with reversible cerebral vasoconstrictive syndrome presented with recurrent thunderclap headaches. The remaining three patients were diagnosed with a carotid arterial dissection; one presented with a new unilateral headache and abnormal neurological examination (Horner's syndrome) ipsilateral to the side with pain, a second patient presented with a unilateral headache and symptoms consistent with transient ischemic attack (amaurosis fugax and transient aphasia), and the third patient presented with new unilateral pulsatile tinnitus with ipsilateral cephalgia not consistent with migraine.
Red and yellow flags subgroup analysis
Thunderclap onset
Three of 17 patients reported to have thunderclap headache may have, in retrospect, experienced sudden worsening of their known primary migraine disorder. An additional three patients were found to have MRA evidence of vasospasm consistent with reversible cerebral vasospasm syndrome. Four patients presented with thunderclap headache triggered by intercourse (n = 2), extreme exercise (n = 1), and Valsalva maneuver (n = 1). All patients completed an MRA or CTA of the head, and five completed an MRA or CTA of the neck.
Neurological symptoms or signs
Concern for transient ischemic attack or stroke due to sudden unilateral sensory and motor symptoms or visual disturbance was common in this group (27%; 12/44). In addition, 12% (5/44) of patients reported headache with persistent dizziness and mild ataxia on examination. Two patients with carotid dissection were diagnosed with MRA of the neck; one presented with Horner's syndrome and the other with transient ischemic attacks (amaurosis fugax and aphasia). Three patients presented with probable functional neurological deficits and headache.
Previous headache new or different
Three patients with migraine presented with new headaches triggered by intercourse. Patients in this group often (24%; 8/34) presented with headache that did not clearly fulfill criteria for a primary headache disorder and were new or unlike prior reported headaches. In addition, 18% (6/34) had a known history of migraine that changed in character or frequency in patients with normal neurological examination.
New onset unilateral headache
Five patients presented with predominantly facial pain, one patient responded solely to indomethacin, two likely suffered from trigeminal neuralgia, and two others may have had migraine. Both patients with carotid dissection were included in this subgroup, however 58% (11/19) of patients in this group were not imaged with MRA or CTA of the neck.
Head trauma
Minor head trauma was documented as the rationale for headache in 17% of patients (32/190). Three of these patients were on anticoagulation and one on clopidogrel, and the neuroimaging was pursued to evaluate for intracranial hemorrhage. Others were imaged for persistent headache associated with neurological symptoms or mildly abnormal examination. Most patients imaged for trauma (70%; 133/190) had a normal examination and likely suffered from post-traumatic headache, or primary migraine or tension headache.
“Worst headache of life”
Among patients reporting the “worst headache” of their life, review of clinical records revealed that 56% (9/16) suffered a significant exacerbation of their known primary headache disorder without a thunderclap history, and all had normal neurological examinations. Two patients in this subgroup were diagnosed with reversible cerebral vasoconstrictive syndrome, and also presented with the red flag of thunderclap headache.
Persistent headache
The failure of a headache to improve with time was the rationale for imaging in 19% of cases (36/190). Persistence was defined by the provider without use of a strict time line. Eight percent (16/190) of cases with persistence presented with symptoms consistent with a primary headache disorder and had normal neurological examinations and absence of red flags. Chart review suggested that six percent (12/190) of these patients likely suffered from status migrainosus, or transformation of migraine from episodic to chronic daily pattern.
Nocturnal awakening
Nocturnal awaking was considered in the recommendation to image in 8% of cases (16/190). Five of these patients likely suffered from migraine and likely suffered from medication overuse headache. The remaining patients had other red flags to justify imaging.
Age
No patients presenting with a new headache after age 50 were found to have a neuroimaging abnormality. Excluding cases in which age >50 alone was used to justify imaging, 27.5% of these cases (22/80) may be considered to be imaged against guidelines (i.e. primary headache disorder with normal neurological examination).
Guideline recommendations
The rate of conducting neuroimaging against guideline recommendations was 23% (44/190). If cases in which age > 50 was the sole red flag were included, then 35% of patients (66/190) may be considered to be imaged against guideline recommendations.
Discussion
We present a descriptive study of the utilization of neuroimaging with respect to warning flags (red or yellow) in clinical practice, and adherence to neuroimaging guideline recommendation in outpatients presenting for evaluation of headache. We observed a high rate (85%; 161/190) of patients documented to have a warning flag, with a low rate (3.1%; 5/161) of imaging abnormalities. Our data is similar to prior reports of an overall low yield of neuroimaging abnormalities in patients presenting with headache (20–25). Headache patients presenting to the community outpatient setting appear to carry a low risk of serious neurovascular imaging pathology even when the headache history includes warning flags. These data suggest that some patients, even with warning flags, may be safely managed without neuroimaging. However, we caution that this study does not diminish the importance of recognizing warning flags or advocate against their assessment in practice. This study was not designed to determine the positive predictive value of an abnormality based on the presence of a red flag, but supports further prospective study of the value of red or yellow flags to better inform provider and patient decision-making.
Another key finding is that neuroimaging studies were frequently ordered despite guidelines recommending against their need given the clinical presentation. We estimate that up to 35% of patients were imaged against guidelines (if those imaged with the only red flag of age >50 are included). The factors leading to the practice are not clear. Presumably reassurance of the patient and provider may play a role in this practice. Some patient imaging against guidelines may have been performed with a goal of reducing patient anxiety, a practice that may be reasonable and cost effective for select patients (26). It is unclear whether current guidelines are not understood, not known, or simply not utilized, particularly by primary care providers, or perhaps not trusted because they are outdated. To date, the publication of neuroimaging guidelines (27) and patient-centered decision-making tools (28) have not been clearly demonstrated to reduce the utilization of neuroimaging (29). However, imaging clinical decision support remains a promising intervention (30), but relies upon non-expert obtained clinical history and application of guidelines.
Notably, all five of the neuroimaging abnormalities observed in our study were diagnosed with non-invasive angiographic studies rather than routine structural MRI or CT. All patients with thunderclap headache underwent non-invasive angiography. However, 58% (11/19) patients with new unilateral headache, two of which were diagnosed with carotid dissection, underwent angiogram studies of the neck, suggesting underutilization of non-invasive angiographic studies in our practice and the importance of considering cervical arterial dissection in this group.
In all the abnormal cases, a neurologist was involved in the decision to order vascular imaging or provided direct care soon after primary care presentation. In most other cases, primary care physicians and advanced practice providers ordered most studies, rarely with the input of a neurologist. This observation suggests that involvement of a neurologist earlier in the care process at the time of imaging decision may aid in appropriate neuroimaging test selection. In addition, earlier neurologist involvement may help determine which patients are low risk, in whom empiric treatment and avoidance of neuroimaging may be safe or supported by guidelines, thereby avoiding the cost and risk of discovering incidental imaging abnormalities (5). Specific presentations in our study in which a neurologist may have offered a different perspective included patients with persistence, progression, and “worst headache of life” reasons for imaging, which could be explained by transformation of migraine, which commonly occurs at a rate of 2.5% per year (31). Medication overuse headache was also overlooked as a common cause of nocturnal awaking with headache. Improved recognition of these common primary headache disorder presentations by clinicians may reduce the rate of neuroimaging, or perhaps these warning flags could be used to triage patients to early neurologist evaluation. The recommended expertise and knowledge of headache disorders needed to accurately determine which patients should be imaged and with which imaging modality (14,22) may not be feasible or practical to obtain for most primary care providers.
Although earlier neurologist involvement could lead to a reduction in unnecessary neuroimaging, it could also increase neuroimaging through improved identification of warning flags. In a national study of neurology practice (32), clinical care by a neurologist was associated with higher cost, with reduced adverse events and acute care presentations. In the National Ambulatory Medical Care Survey (NAMCS), neurologist visits were associated with increased neuroimaging (3). However, within the Veterans Administration system, neuroimaging rates for patients with headache is lower when compared to Medicare patients; although it is unclear whether neurologist input into the imaging decisions or other system factors explain these differences (33).
The care model of integrated neurology co-located within a primary care medical home has been associated with reduced brain MRI utilization in a general neurology practice (17). This practice was also shown to utilize neuroimaging less than the traditional tertiary neurology practice at our institution (34). This practice model provides timely access to neurological expertise for primary care teams via telephone curbside discussion, electronic consultations, and triage of face-to-face visits. This assistance could aid in identification of warning flags, facilitate proper neuroimaging test selection, or provide reassurance when a warning flag may be explained by a known primary headache disorder. This service was available to all patients imaged during this study, but was only utilized in 14% of cases. This suggests that increased utilization of our integrated practice model may reduce unnecessary neuroimaging and improve imaging test selection when needed. This model provides a unique care pathway that could be designed and deployed to outpatient headache patients with warning flags.
The strengths of this study include a detailed assessment of clinical decision-making within a well-defined community population. We evaluated patients who initially accessed care through a primary care team and who were subsequently referred to a neurologist at the discretion of the primary provider. We studied a broad range of patients who are typical of most primary care community practices. Our imaging rates of 10–14% of visits are similar to that observed in the National Ambulatory Medical Care Survey (NAMCS), in which 39% of patients with a migraine diagnosis and 51% with a chronic headache diagnosis were imaged over five years (3), although differences in study design limit this comparison. Therefore, our findings may be generalizable to community practices. Prior studies of imaging utilization relied on ICD diagnosis alone (3), and direct chart review was not performed in these studies to better understand clinical decision-making. The retrospective chart review allowed us to more accurately categorize headaches according to ICHD-3 beta criteria rather than ICD codes, and focus on outpatients that did not have a known or clear cause of their headache at presentation.
Our study has several limitations. Patients in this cohort did not have a standardized assessment or documentation of warning flags, which may have resulted in under-reporting if missed on chart review or over-reported if misinterpreted within the clinical history. Furthermore, neurological examinations and headache histories were not uniform and were obtained by many different providers with varying clinical expertise. There is also inherent bias of the retrospective design and a single investigator (NPY) determining the presence of a red flag, ICHD-3 beta diagnosis, and guideline adherence. The population size was smaller than expected, as most headache neuroimaging of at our institution occurred in the emergency department, which we excluded from the current study. We did not include a comparison to a control group or statistical comparison of subgroups because of the retrospective limitation and small sample size, and have presented only descriptive findings. Lastly, imaging was not standardized, and some patients may have had secondary headache that was not diagnosed because they did not have noninvasive vascular imaging or brain MRI when the head CT was completed.
Conclusion
The presence of neuroimaging abnormalities that would explain headache in our community practice was low (3.1%), even in the presence of documented warning flag symptoms (85%), suggesting that some patients with apparent warning flags may be safely managed without neuroimaging. When abnormalities were discovered, they were diagnosed with non-invasive vascular imaging studies with early neurologist input into neuroimaging test selection. Inadequate awareness of or application of warning flags and atypical presentations of primary headache disorders may be contributing to recommendations to perform neuroimaging on patients against guideline recommendations. Our findings highlight opportunities to improve the utilization of neuroimaging for headaches in the ambulatory community practice. Several interventions to reduce unnecessary neuroimaging of patients with headache are suggested for further study including: a) collaborative care models involving early neurological assessment of headache and input into neuroimaging decisions; b) shared decision-making tools; and c) primary care and patient education.
Footnotes
Clinical implications
Neuroimaging studies are often performed against guidelines in outpatients with a low risk of a serious secondary cause of headache.
Outpatients presenting with headache and red flags appear to have a low risk of a serious secondary cause of headache, suggesting that some of these patients may safely be managed without neuroimaging.
Novel primary care – specialty collaborative care models – may lead to improved neuroimaging test selection, reduce unnecessary imaging, and improve clinical outcomes.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was made possible by CTSA Grant Number UL1 TR000135 from the National Center for Advancing Translational Sciences (NCATS), a component of the National Institutes of Health (NIH). Its contents are solely the responsibility of the authors and do not necessarily represent the official view of NIH. This publication was also made possible using the resources of the Robert D and Patricia E Kern Center for the Science of Health Care Delivery.