
Abstract
Aim
To determine the red flags for serious organic causes of headache in children, to analyze if the management of headache in the Pediatric Emergency Department is appropriate, and whether the follow-up may limit repeated visits to the Emergency Department.
Methods
All the patients ≤ 18 years referred to our pediatric Emergency Department for non-traumatic headache over 5 years were retrospectively reviewed. The patients followed up by the Pediatric Headache Centre were also screened. Statistical analysis was undertaken using the Chi-squared test or Fisher’s exact test and multivariate analysis; significance at p < 0.05.
Results
1833 patients (54.6% males) accessed our Emergency Department 2086 times; 62.1% had primary headache, 30.0% had secondary headache, 7.8% received inconsistent diagnosis. Among those with secondary headache, 24 (1.1% of total visits) were diagnosed with serious disorders. The clinical red flags for “serious headache” were: Cranial nerves palsy, strabismus, and drowsiness. One hundred and eighty four patients (8.8 %) underwent neuroimaging (rate of pathological findings: 7.1 %); 37.2 % of the patients received analgesic therapy. One hundred and fifteen patients (6.2 %) returned within three months; 24 of these were referred to the Headache Centre, with only one accessing the Emergency Department again.
Conclusions
The vast majority of headaches referred to the Pediatric Emergency Department are benign, and primary forms prevail. “Serious headache” is rare and shows typical clinical features and abnormal neurologic evaluation; specific clinical red flags, along with suggestive personal history, should lead the pediatrician to prescribe only appropriate neuroimaging. Pain relief is still insufficient in the Pediatric Emergency Department despite appropriate guidelines. Last, the collaboration with the Headache Centre is crucial to limit repeated visits.
Introduction
Headache is a common condition in childhood and represents one of the most frequent reasons for access to the Pediatric Emergency Department (ED).
The reported prevalence of headache among children of school age varies greatly, from 6% to 82%, depending on the age and the definition criteria, and increases gradually during adolescence (1,2). Previous estimates report up to 75% of children having almost one episode of significant headache before 15 years of age, and up to 28% of adolescents describing migraine (3,4). Some authors suggest that headache accounts for approximately 1% of all pediatric ED visits (5–8).
CT scan performed in the evaluation of headache in pediatric ED: Comparison to the literature.

Total number of neuroimagings: CT scan + MRI.
The incidence of secondary headaches due to serious or life-threatening causes is low, but their identification is a major aim of the Pediatric ED, along with providing prompt, safe and effective healing of pain. The diagnostic approach to pediatric headache in the ED is thus of great importance. The American Academy of Neurology (AAN) Practice Guidelines edited in 2002 and reaffirmed in 2013 provide recommendations about the diagnostic approach only to children and adolescents with recurrent headaches, and make no specific statement about patients in the ED setting (2). Furthermore, despite the AAN guidelines and several studies considering neuroimaging unnecessary to exclude serious intracranial disorders if no other neurologic symptom is reported, the CT scan is still widely used for children with headache, as reported in Table 1. (9,11,14–16).
The aim of our study was to assess the characteristics of children referred to the Pediatric ED because of headache, in order to identify the clinical features that possibly let us differentiate primary and secondary forms. In particular, our main aim was to determine the clinical red flags that could help clinicians to recognize serious organic causes of headache. Furthermore, we evaluated whether the diagnostic tests and the treatment of headache in the Pediatric ED were appropriate and whether the follow-up after discharge might limit repeated visits to the ED for headache.
Methods
All the patients up to 18 years referred to the ED of the Regina Margherita Children’s Hospital of Turin, Italy, over 5 years between January 2011 and December 2015, reporting headache as the main symptom, were retrospectively reviewed.
We excluded patients with already known neurosurgical disorders, with ventriculo-peritoneal shunt and those with final diagnosis of post-traumatic headache.
The medical record databases of our ED were screened for information relative to the demographic profile of children (age, sex, and ethnicity), date of admission and discharge, clinical features of headache, associated symptoms, personal medical history, results of laboratory tests, neuroimaging investigations and specialist consulting visits, diagnosis at discharge and therapy administered. The medical record databases of our Pediatric Headache Centre were also screened for information relative to those children who had been referred there after discharge from the ED.
Headache was divided into primary and secondary according to ICHD-III beta criteria; if explicitly reported, we identified specific subtypes of primary headache, such as migraine. Headache was defined as “serious” if the diagnosis included any organic and structural involvement of the central nervous system, and the patient needed prompt diagnostic workout and/or prompt therapeutic intervention at the ED. Statistical analysis was performed using SAS software for Windows, version 9.2 (SAS Institute Inc., Cary, NC, USA). The data are described as the mean ± standard deviation (SD) values or medians and ranges for continuous variables, normally or not normally distributed, respectively, and absolute and relative frequencies for categorical variables.
The Chi-squared test or Fisher’s exact test was used to evaluate proportions, as appropriate. In particular, the Chi-squared test for equal proportions was used to evaluate the statistical significance of the seasonal variability of ED visits for headache. Multivariate logistic regression was performed to control for potential confounding factors and to investigate the clinical features that had higher association with pathological headache; the results were described by Odds Ratios (ORs) and 95% Confidence Interval (95% CI). The choice of the variables to be included in the regression model was made using a stepwise method (option select = stepwise in the SAS proc logistic). We chose a significance level of 0.3, required for allowing a variable into the model, and a significance level of 0.35, required for a variable to stay in the model.
Subjects with missing values for at least one of the variables included in the models were excluded from the analysis.
A p-value < 0.05 was considered to be statistically significant, and all of the p-values were based on two-tailed tests.
Results
The study population consisted of 1833 patients (1000 males and 833 females, respectively 54.6% and 45.4%), who accessed our ED 2086 times (0.9% of all the visits for any purpose during the study period): 1659 children had one single access, 139 had two visits, and 25 had more than two visits, with a median time of 42 days between consecutive ED visits (range 0–1433 days). One hundred and fifteen patients had repeated visits within 3 months of the previous access, corresponding to 272 accesses (59.3% of repeated visits); 90 of such visits occurred within 10 days with a peak within 3 days. Among patients returning within 10 days, 78.5% had persistent headache, 11.2% showed new symptoms (e.g. vomiting, fever), 8.1% had a new episode of headache, and 2.0% returned under a specific prescription of their general practitioner.
Patients’ characteristics stratified by age.
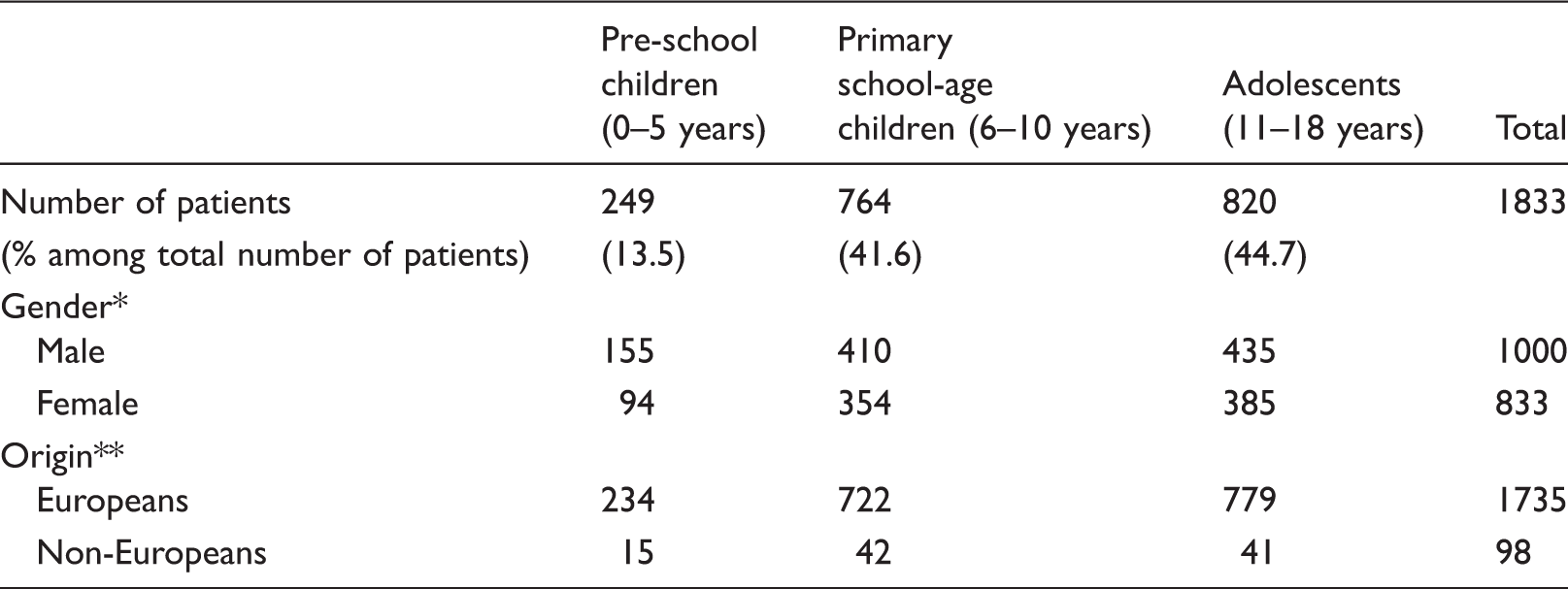
p = 0.04, **p < 0.001.
One hundred and sixty three patients (7.8% of total visits for headache) underwent further investigations after the ED visit. Furthermore, we observed a seasonal variability of ED visits for headache, with February, May and November being the months in which most of the visits occurred; ED visits were less common in August (p < 0.001, Figure 1).
Seasonal variability of ED visits for headache.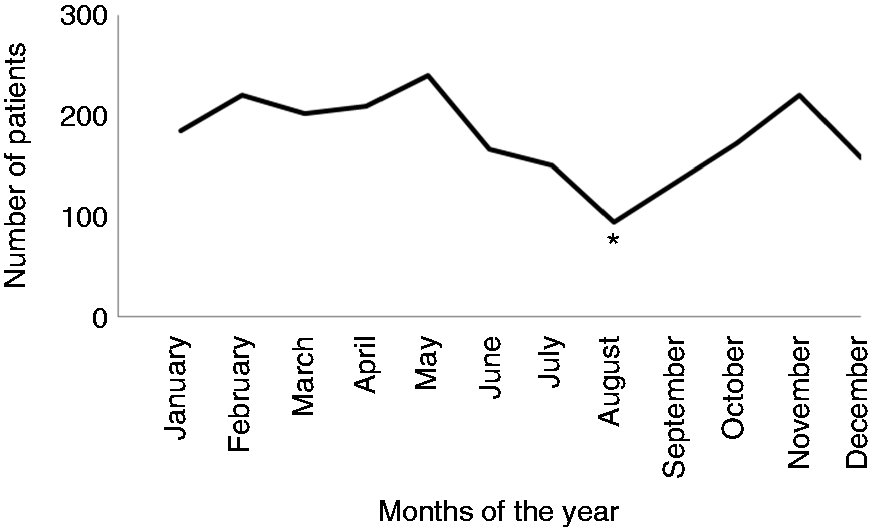
Types of headache
Among all the visits, 1295 patients had primary headache (62.1% of all the visits for headache), 628 had secondary headache (30.1 %) and 163 (7.8%) received a final diagnosis that did not explain headache (e.g. constipation, abdominal pain, dermatological disease).
In the primary headache group, 1222 patients (94.4%) received a diagnosis of “not otherwise specified primary headache”; migraine accounted for 70 cases (5.4% of primary headaches; mean age 11.12 ± 2.47 years) and a similar distribution between genders (37 males and 33 females, p = 0.46); three patients received a diagnosis of benign paroxysmal vertigo (mean age 5.66 ± 2.08 years).
Causes of secondary headache in the pediatric ED.

Causes of serious headaches in the pediatric ED.

Associated symptoms and clinical features in non-serious and serious headache.

P-values in bold are those with statistical significance.
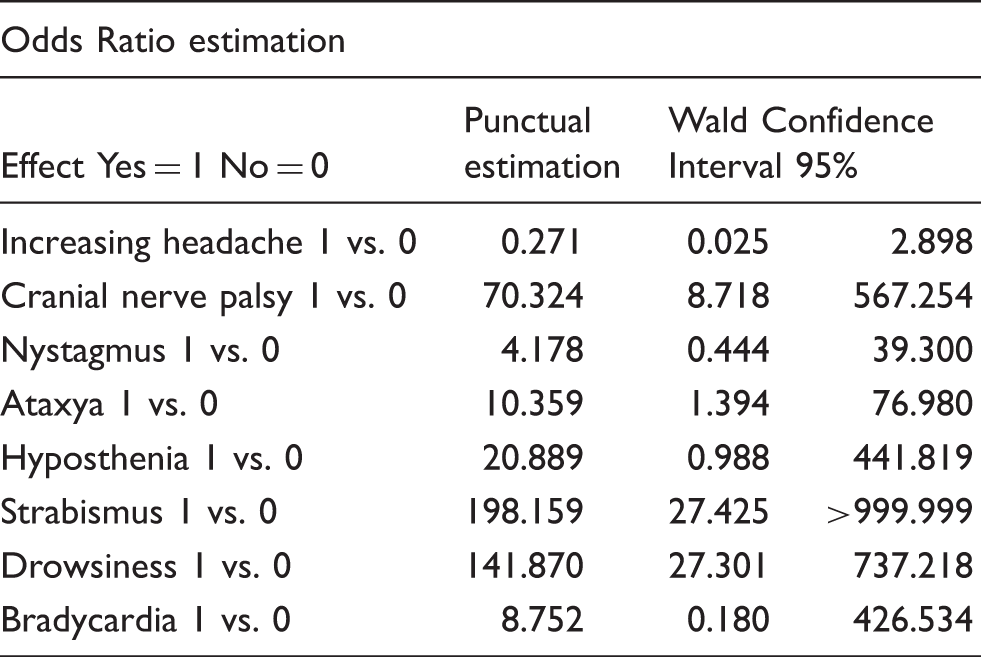
Clinical features associated with a greater risk of serious headache by multivariate analysis.
Prevalence of non-serious and serious headache according to the number of clinical red flags showed by patients.

p < 0.001.
Serious headache: Odds Ratio for 2 red flags vs. 0: 380.1 (I.C. 108.9 > 999.9); Odds Ratio for 1 red flag vs. 0: 39.3 (I. C. 28.1–284.8).
Diagnostic tests and treatment at the ED
Among all the patients, 390 specialist consulting visits were requested: 187 neurological, 156 ophthalmological, 19 neurosurgical, and 28 otorhinolaryngoiatric. An EEG was performed on 120 patients and showed specific abnormalities in 15 cases (12.5 %).
Neuroimaging investigations were performed on 184 patients (8.8 % of total visits): 175 had a brain computed tomography (CT) scan, nine had a brain magnetic resonance imaging (MRI) scan and four had both a brain CT and MRI, with a 12.5% rate of abnormal findings (23 patients): 13 patients (7.1%) had pathological findings, while in 10 other cases (5.4%), neuroimaging revealed incidental benign abnormalities not related to the reported symptoms (Chiari I malformation and arachnoid cysts without hydrocephalus). Among the children undergoing neuroimaging, 148 (80.4 %) received a diagnosis of primary headache at discharge. Out of the total neuroimaging investigations, 117 scans (63.5 %) were ordered by an emergency pediatrician, 56 (30.4 %) by a neurologist and nine (4.8 %) by another consultant. Pediatricians showed a higher rate of pathological findings compared to the other specialists (10.2 % vs. 2.0%, p = 0.04).
Treatment of headache in pediatric ED.

Follow-up after accessing the ED: The Pediatric Headache Centre
On discharge from the ED, 646 patients (30.9%) received the indication to refer to the Pediatric Headache Centre and 259 of them (40.0%) actually did.
As regards the follow-up of the children who had multiple ED accesses for headache, 32 patients among the 115 who had repeated visits within 3 months (27.8%) received the indication to refer to the Pediatric Headache Centre; 24 of them (75.0%) were actually followed up, and only one of them accessed the ED again because of headache after starting the follow-up.
Only 2.5% of patients already regularly followed at the Headache Centre accessed the ED because of headache during the study period.
Discussion
We describe the largest population of children with headache reported from the longest study period so far in a Pediatric ED (5–8).
The prevalence of headache among all the visits at our Pediatric ED is similar to that reported by other authors (5–8). Consistent with previous data, our population showed a slight male-to-female prevalence, which flattens with increasing age; adolescents were the most represented, in contrast with other studies in which school-age children were prevalent (5–8). We also observed a seasonal variation of ED accesses for headache, with a peak of visits in months usually associated with higher school-related stress and a nadir in summer, in accordance with literature (18).
The majority of our patients received a diagnosis of primary headache, confirming previous experience from our hospital (7), but in contrast with other studies, in which secondary headache is prevalent (5,6,8,10,16); these results suggest not only an increase in primary forms of headache at pediatric age, but also a greater awareness among ED pediatricians about such forms.
Despite migraine being the most frequent primary headache in children, it represented only a minority in our cohort. This is not unexpected, because the main aim of ED pediatricians is not to differentiate the several types of primary headache, but to recognize the history and clinical features suggestive of primary forms and the clinical red flags for serious disorders underneath secondary ones. Age and gender of our migraine patients were consistent with our previous observation (17).
According to literature, the majority of secondary headaches are benign, self-limiting and mainly caused by infections, in particular of the upper airways (5–8,10,16). The overall frequency of “serious” causes of headache that we have observed was very low, even less than reported in other studies (5–8,10,11). The two children with serious headache who were diagnosed at the second access to our ED did not show any clinical red flag and had a normal neurological evaluation on their first access. Some hours later, the onset of a new symptom (drowsiness) led them back to the ED. Our hospital is the regional reference centre for pediatric neurological and neurosurgical disorders, so we are confident that no other serious headache was missed. Our results regarding the clinical features associated with serious headache confirm that an accurate neurological evaluation, along with accurate personal history, is fundamental in the approach to children with headache and should guide clinicians in the diagnostic work-up. In fact, on one hand 79.2% of the children with serious headache showed at least one clinical red flag; on the other hand, among the five children without clinical red flags, only two did not show any suggestive risk factor in their personal history and general physical examination. Instead, interestingly, nocturnal awakenings and nystagmus were not associated with a higher risk of pathological conditions. Our observation, in particular regarding nocturnal awakenings, is in contrast with previous data (15) and suggests that these clinical features are non-specific, especially if isolated.
The rate of neuroimaging in our population was lower than reported in the majority of the other studies, but we also had a lower rate of pathological findings (Table 1). Data from literature show that pathological findings are reported in less than one out of four children undergoing neuroimaging, and only one group reports 40% of abnormal findings in their series: neuroimaging in children with headache is indubitably overused and should lead to a more careful evaluation of personal history and clinical features considered so far (9,11,14–16). The dose of radiation from a single brain CT scan (20 to 56 mGy units of radiation) carries quantifiable risk to the pediatric population: it has been shown that cumulative doses of 50 mGy can almost triple the risk of leukaemia, and doses of 60 mGy can triple the risk of brain cancer (15). Children are more sensitive to radiation than adults, and their longer life expectancy increases their window of opportunity for manifesting long-term sequelae from radiation. Children with severe symptoms, but without emergency symptoms, should undergo MRI rather than CT scan. Though MRI is much more informative than CT scan, the latter is commonly preferred because it can be more easily accessed in the ED setting and because it answers more rapidly to the need for relief of anxiety for children and their families. The higher anxiety rate reported among patients who did not undergo a CT scan supports this perception, but the lifelong cumulative cancer risk due to radiation should be always kept in mind before asking for a brain CT in children. Furthermore, some neuroimaging investigations in our patients showed accidental findings; this can further complicate management, as it is known to contribute to increased patient stress and anxiety, as well as further testing. Anyway, the reported rates of neuroimaging in children with headache in the ED are still lower than those reported in adults, varying from 14–50% (19,20).
As regards the therapeutic approach at the ED, only one out of three patients received a pharmacological treatment. Unfortunately, this is not an unexpected result and is consistent with widespread underestimation and under treatment of pain in the Pediatric ED (21). A multicenter study published in 2013 by the Italian Pain In Pediatric Emergency Room group showed that despite the availability of national and international guidelines, the policies towards children’s pain management are still sub-optimal as regards the presence of local protocols, the use of algometric scales, and pain reassessment after treatment (22). Our results on this topic also have some limits due to the retrospective study design, because frequently algometric scales and previous domiciliary treatment were not clearly detailed on the ED records. Furthermore, we noted that in some cases when the patients had had the visit, they did not report headache any more, probably because the care for the headache contributes itself to reassure the patients and their families and to reducing their anxiety and their fear of a pathological diagnosis underlying headache.
In our hospital, there is a collaboration between the Pediatric Headache Centre and the ED: according to the ED doctor’s decision, patients discharged with a diagnosis of primary headache or those with repeated episodes of headache can be referred to the Headache Centre within a few days. Therefore, we have analyzed data about the follow-up in our Pediatric Headache Centre and, in particular, the possible effect of repeated visits to the ED for headache, as there are very few studies investigating such relations (7,16). Almost all the repeated visits within three months occurred in patients who had not been referred to the Headache Centre after the first visit to our ED or in patients who received a specific indication to follow up, but did not attend. On the other hand, only 2.5% of patients regularly followed at the Headache Centre accessed the ED because of headache during the study period. These observations suggest that the alliance between the ED and the Headache Centre is very important and might play a role in reducing the so-called “revolving doors”.
Limitations of this study include its retrospective design and lack of complete follow-up monitoring. The analysis was limited to the information reported on the clinical records, and it is possible that pertinent history and examination findings were not recorded.
Conclusions
The vast majority of headaches referred to the Pediatric Emergency Department are benign and self-limiting, with a prevalence of primary forms. The children with “serious headache” are a minority, and show typical clinical features and an abnormal neurological evaluation. In particular, our analysis identified four specific clinical red flags, associated with major risk of “serious headache”: cranial nerves palsy, ataxia, strabismus and drowsiness, and we observed that the higher the number of clinical red flags shown by the patient, the higher the risk. Furthermore, our results showed that the rate of neuroimaging is still too high compared to the rate of pathological findings. The neuroimaging prescription should be guided by the neurological examination, mostly by the detection of the mentioned clinical red flags. For patients with an unclear history or another isolated neurological sign, clinical observation could be more appropriate to evaluate the possible appearance of clinical red flags and the need for neuroimaging.
Moreover, our data confirm that pain relief must be implemented in the Pediatric ED. Finally, the collaboration with the Headache Centre is crucial to limit repeated visit and to ensure appropriate follow up. All the research material related to our paper is available by contacting the corresponding author.
Clinical implications
The vast majority of headaches referred to the Pediatric Emergency Department are benign and self-limiting, with a prevalence of primary forms. “Serious headache” is rare and shows typical clinical features and abnormal neurologic evaluation. The rate of neuroimaging is still too high compared to the rate of pathological findings, and this prescription should be guided by the detection of specific clinical red flags. Pain relief is still insufficient in the Pediatric ED despite appropriate guidelines. The collaboration with the Headache Centre is crucial to limit repeated visits.
Ethical approval
The study was performed according to the international regulatory guidelines and current codes of Good Epidemiological Practice. Because patient care was not altered by the inclusion in the study, the approval of ethical committee was not necessary.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.