
Abstract
Objective:
The study objective was to analyze cases of sudden death that presented to the National Deptartment of Clinical Neurosciences, Ireland, over a 10-year period (1997–2006) where headache was the presenting symptom.
Background:
Headache is a common yet challenging presentation in clinical neurology. In the vast majority of cases, the cause is trivial and reversible—however, in a few patients it may be indicative of a more sinister intracranial process. Recognizing associated “red flag” features and identifying possible life-threatening causes are crucial in ensuring prompt and appropriate intervention.
Design/methods:
A retrospective study/database of all autopsy cases presenting to the Neuropathology Department in Beaumont Hospital, Dublin, was carried out for the period 1997–2006. Cases were selected with headache as the presenting clinical feature. Traumatic head injuries or known central nervous system (CNS) disorders were excluded. Autopsy and medical reports were reviewed to identify associated red flag features at initial presentation according to the International Classification of Headache Diseases, second edition (ICHD-II) criteria.
Results:
Fifty-five autopsy cases out of a total of 499 complying with selection criteria were reviewed. Over the 10-year-study period, the number of cases of fatal headaches over time were negatively correlated. The most commonly associated red flag symptoms included age over 50: loss of consciousness and collapse, and worst/thunderclap character of headache. Cause of death at autopsy comprised vascular events 60.4% (N = 29), primary brain tumours/cysts 16.7% (N = 8) and meningitis 6.25% (N = 3). Aneurysms accounted for the majority of vascular cases 22.9% (N = 11), with loss of consciousness, occipital headache, neck pain and a focal neurological deficit seen more commonly in this subset of cases.
Conclusions:
Sudden-onset headache is a common and often alarming presentation. The majority of cases are of a benign nature; however, a small proportion may be indicative of a catastrophic etiology. Documenting “red flags” on initial presentation is crucial to acutely identify and treat those at highest risk. The results demonstrate an improving trend among clinicians in recognizing and initiating appropriate interventions in these patients, and highlights particular red flag features common in cases of fatal headaches.
Introduction
Intracranial causes of sudden death in adults are not uncommon, and include trauma, tumor, hemorrhage, ischemic stroke and epilepsy. In many instances, a headache may herald an acute catastrophic event. Headache, however, is one of the most common and often one of the most challenging symptoms in clinical neurology to decipher. In the vast majority of cases that present to emergency departments, the cause is trivial and reversible, but in a few patients headache may be indicative of a more sinister intracranial process.
Headaches can be broadly classified into primary (history or clinical examination do not suggest a secondary cause and imaging, such as CT scan, excludes the same) or secondary (attributable to another cause, e.g. vascular, neoplastic or infectious) (1). Primary headache disorders are common; however, in clinical practice there is frequently a high level of anxiety among patients and physicians that the headache could be due to a secondary cause. Investigation with neuroimaging is both expensive and low yield, unless there are specific alerting features in the clinical history and examination. Thus, these “alerting” features in secondary headaches are classified into “blue flag” features, not requiring urgent attention or “red flag” features, requiring urgent attention (1,2). In some cases, despite clinical evaluation, these features may be overlooked, and certain potentially treatable conditions are missed (3).
This study examined cases of sudden death where headache was the initial presenting feature. Incidence, epidemiology of cases, clinical features, associated presenting complaints and ultimate cause of death were reviewed, thus highlighting common features which may help clinicians promptly identify sinister causes of headache.
Methods
Presenting “red flag” symptoms of 55 fatal headache cases.

Pyrexia, night sweats, respiratory distress, pneumonia.
LOC: loss of consciousness.
Results
Between January 1997 and December 2006, 499 cases from the Department of Neuropathology autopsy database were identified as sudden unexpected deaths. All cases with traumatic etiology or a known underlying CNS abnormality were excluded. Fifty-five of these complied with the study selection criteria of having presented to an emergency department or primary care practice with principal complaint of headache.
Of the 55 cases, 51% (N = 28) were male and 49% (N = 27) were female. The number of deaths per year with headache as a presenting feature ranged from 11 (22% of all cases) in 1999, to 1 in 2004, with a mean of 5.5 cases per year (Figure 1).
Number of autopsy cases per year with headache as presenting feature.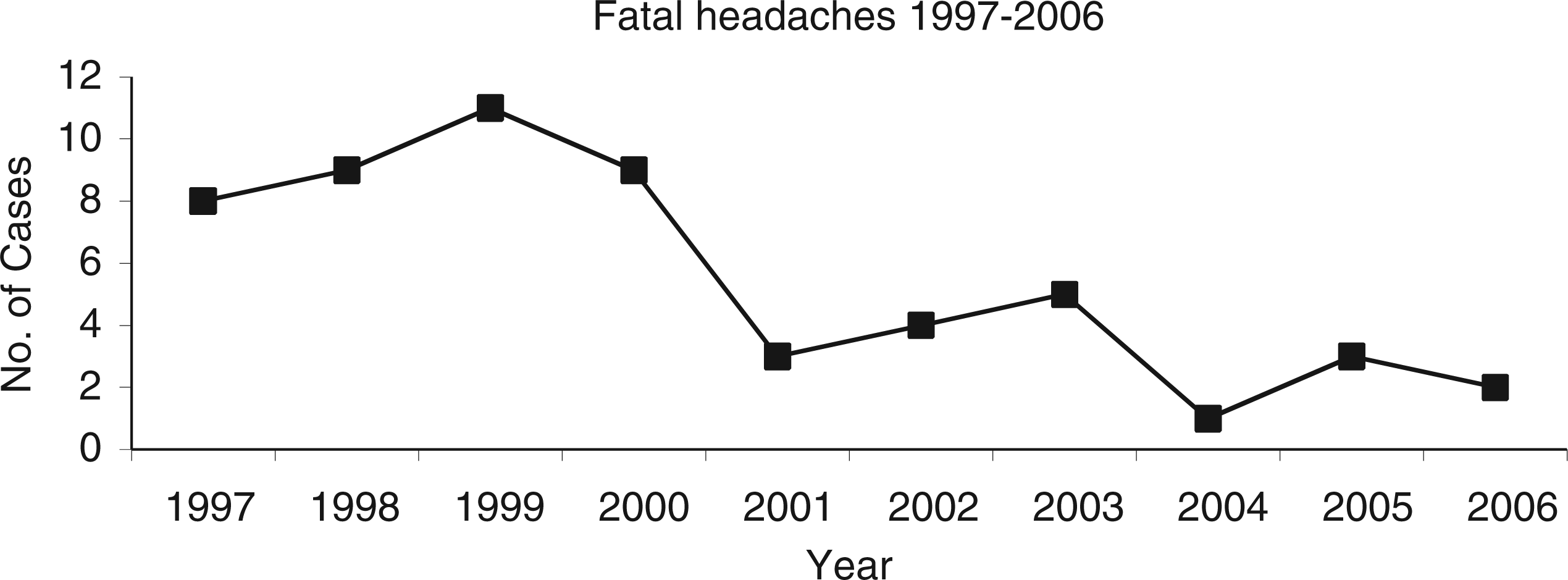
The age of the study population ranged from 12 to 82 years. The peak incidence of deaths, 34.5% (N = 19), occurred in the 51–70 age group. There were no cases identified in the >10 years age group, and the least number of recorded cases were in the 10–18 and 19–25 year-old age group, with three cases each (Figure 2). Of patients >50 years old, 26.7% (N = 8) had multiple co-morbidities, including one or more of the following: hypertension, diabetes, atrial fibrillation, history of pulmonary embolus, or renal or cardiac conditions. Sample sizes of cases among varying age groups were too small to be statistically significant for red flag symptoms; however, one etiology was more prevalent in the younger age group, with 40 years used as the median. Sinus venous thrombosis (SVT) comprised 8% (N = 4) of total cause of death from sinister headache. All four cases of SVT occurred in female patients <40 years of age in pro-thrombotic states, with 100% occurrence of two primary red flag features: prolonged occipital headache with neck pain, and a progressive focal neurological deficit.
Distribution of fatal headache as a presenting feature in the various age groups.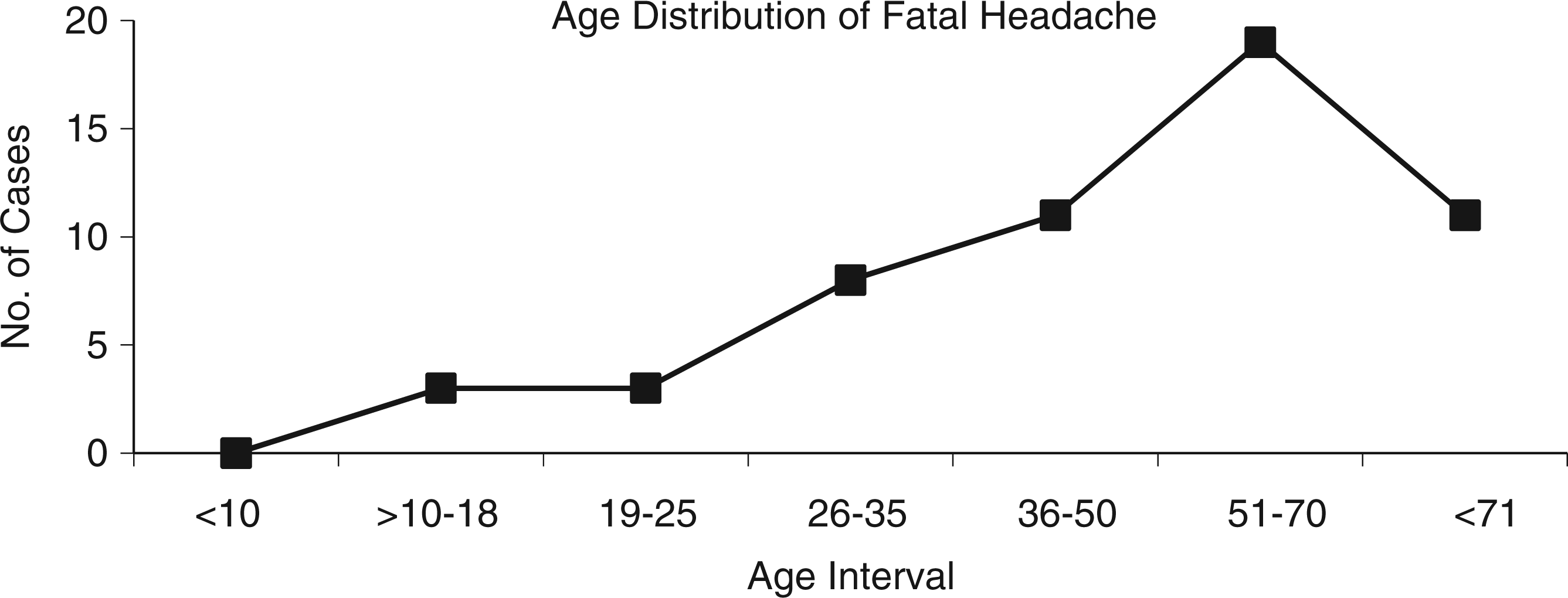
All 55 patients presented with an associated red flag symptom to the emergency room (Table 1). The occurrence of a headache in patients over 50 years of age was the most common red flag feature, presenting in 54.5% (N = 30) patients. Loss of consciousness or collapse occurred in 52.72% (N = 29); “worst” headache and thunderclap headache in 45.5% (N = 25) and 51% (N = 28), respectively; and nausea and vomiting in 30.9% (N = 17). The red flag features that occurred less frequently included ataxia/incoordination, at 1.8% (N = 1); meningeal irritation, 10.9% (N = 6); and a peripheral sensory deficit, 12.7% (N = 7). To assess the reliability of our metrics, we compared our data to those reported by Sobri et al., in their clinical study on red flag features and abnormal neuroimaging (4). Our patient populations were relatively well matched in age and gender as well as the red flag features recorded, apart from thunderclap headache, which Sobri et al. did not report. The Pearson correlation between our results and theirs was 0.51, p = 0.09. The correlation is highly positive despite the small sample size, demonstrating congruency of certain red flag features in our autopsy series with those of a clinical series related to abnormal imaging (supplementary data).
A total of 7 of the 55 cases were later discovered to have suspected trauma with significant subdural hemorrhage (SDH) at autopsy, and were excluded from the final headache study group in analysis of etiology of headache. The ultimate causes of death found at autopsy in the headache group (N = 48) were vascular events, which comprised 60.4% (N = 29); primary brain tumors/cysts, comprising 16.7% (N = 8); meningitis, comprising 6.25% (N = 3); and other, comprising 16.7% (N = 8) (Figure 3). “Other” incuded ischemic infarction (N = 3), undocumented suspected trauma cases with SDH (N = 5), SVT (N = 4), cerebral abscess (N = 1) and cerebral metastases (N = 1). Primary brain tumors made up 8.3% (N = 4); specifically, pituitary adenoma (N = 2), glioblastoma multiforme (N = 1), and meningioma (N = 1).
Cause of death at autopsy of 48 patients presenting with fatal headache to Centre for Neurological and Neurosurgical Science, Beaumont Hospital, 1997–2006.
Of the 29 vascular events found at autopsy, multifactorial hemorrhages accounted for 18.7% (N = 9) of total deaths; aneurysms for 22.9% (N = 11); giant cell arteritis for 4.2% (N = 2); arteriovenous malformation (AVM) for 4.2% (N = 2); arterial dissection for 2.1% (N = 1); and venous thrombosis for 8.3% (N = 4) (Figure 4). Multifactorial hemorrhages included those cases with no vascular structural abnormality identified at autopsy as a source of hemorrhage, but did occur in the setting of either a single or multiple risk factors, including hypertension, concomitant anticoagulant use, amyloid angiopathy, diabetes, chronic renal disease and hepatic or heart disease.
Pathological diagnosis in cases of vascular events.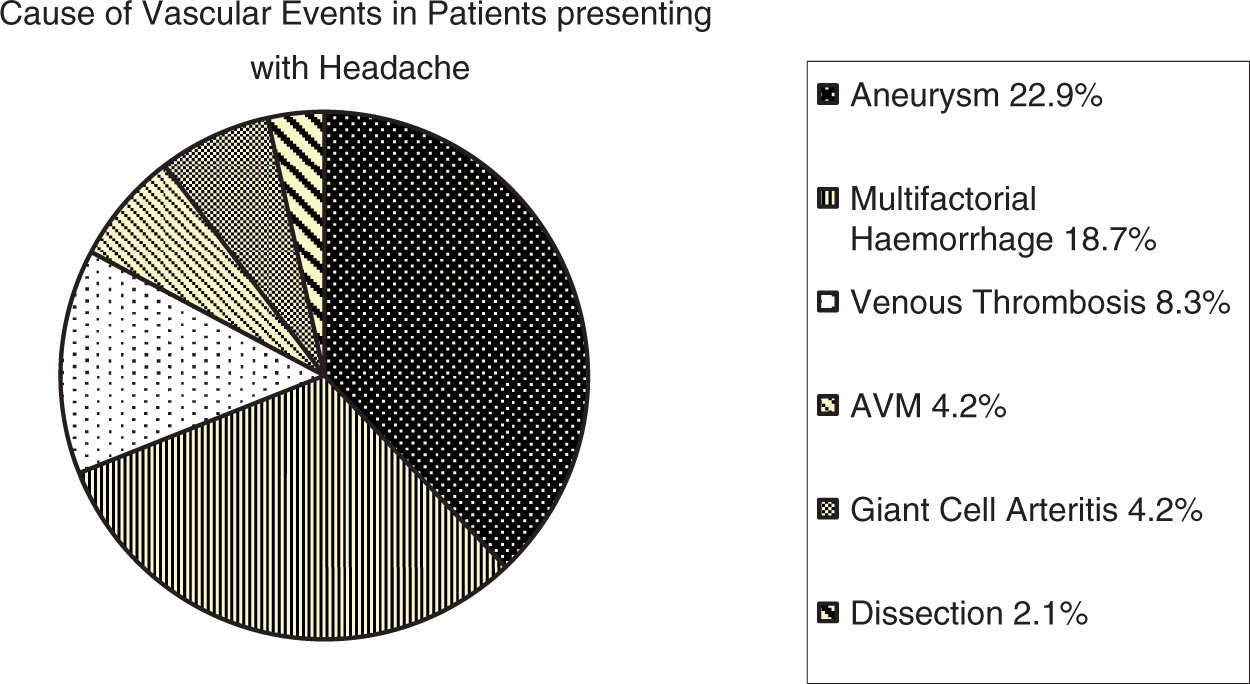
Cases where aneurysm rupture and subsequent intracerebral hemorrhage were found to be the cause of headache comprised 20% (N = 11) of the total study group (N = 55). The male-to-female ratio within this group was 1:3 (males N = 3, females N = 8). Loss of consciousness or collapse in clinical history was the most common red flag feature in this subset, at 64% (N = 7). Occipital/temporal headache and neck pain occurred in 45.5% (N = 5), and a focal neurological deficit (cranial nerve palsies, hemiparesis/parasthesia) was present at initial examination in 36.4% (N = 4).
Discussion
Sudden-onset headache is a common condition presenting to emergency departments, with the majority of cases being primary headache syndromes and secondary tension-type headache (6). In a significant minority of cases, however, headache may be the symptom of a potentially life-threatening event such as subarachnoid hemorrhage (SAH) or primary brain tumor. In this study, autopsy and medical records of sudden deaths over a 10-year period where the primary presenting complaint was a headache were reviewed. Excluding cases with a traumatic etiology or underlying CNS disorder, a total of 48 cases satisfied our selection criteria, with a mean incidence of 5.5 cases per year. Over the period from 1997 to 2006, there is a clear decrease in the number of fatalities in patients presenting with headache as a primary feature in the emergency department, with the highest number of cases recorded in 1999 (N = 11), and least in 2004 (N = 1). The decreasing incidence trend (Figure 1) would suggest improvements made among clinicians in recognizing red flag headaches in patients requiring urgent investigation. We would also surmise that over that period, the availability of out-of-hours neuroimaging and improvements in radiology services are likely to have made a significant impact on lowering the incidence of fatalities among this patient group. Prompt detection of symptoms, confirming a diagnosis with neuroimaging and referral for urgent treatment have all meant that fatal headaches now have a less frequent occurrence.
The study also emphasizes aspects of the presenting red flag features of headaches. In our study population, the more statistically significant, alarming red flag features which ultimately heralded a fatal cause of headache were as follows: headaches in those over 50 years of age, headaches described as “worst”/thunderclap, a history of seizure/collapse/loss of consciousness, and associated nausea and vomiting. Previous studies have investigated red flag features and their varying frequencies among patients presenting to emergency departments or primary care with headache (7,8). Consistent with findings in our study, alarming signs, such as thunderclap or change in headache character, and nausea/vomiting, rank high in diagnosing a serious secondary cause of headache; however, in our study, impairment/loss of consciousness, and headaches in those over 50 years, were found to be of particular significance, and were more frequent than expected in patients with ultimately fatal headaches. Other red flags, such as focal neurological deficits, papilledema and meningeal signs, did not occur with the same frequencies as in other studies (3,4). Using neuroimaging as a screening tool for predicting intracranial pathology, Sobri et al. analyzed red flag features in patients presenting with headache, and found three statistically significant features: paralysis, papilledema and “drowsiness, confusion, memory impairment and loss of consciousness” (4). Assuming that, with the severity of the ultimate pathology in our autopsy series, for a significant proportion (if not all) cases in our study, neuroimaging, if performed, would have shown abnormal results, we compared our red flag features to those in Sobri et al.’s clinical study. We found a Pearson correlation of 0.51 (p = 0.09). With such a small sample size in this restrospective case series (N = 39), one would not expect a significant correlation, but it is nevertheless highly positive, with red flag features congruent in all but two features, which were not recorded in the clinical data by Sobri et al. (supplementary data). It is also worth noting, that as our study is the first to look at post-mortem cases, there is some expected heterogeneity, with certain data values (red flag features) not recorded in the clinical case series reported by Sobri et al., and ultimately more serious events occurring in the autopsy series.
With identification of red flag features, the indication for urgent neuroimaging arises. The majority of studies on this are based on retrospective data. It is suggested that CT scan should be the initial test of choice for new-onset headache in adults, which is the most common reason among clinicians for requesting neuroimaging (6,9). Our study would further suggest that headache in patients >50 years, as well as in those with an associated impairment in consciousness, should be an indication for urgent imaging. Lumbar puncture is recommended thereafter, if CT scan is equivocal, to rule out an SAH. In adults where there may be a suspected metastatic brain lesion, contrast-enhanced MRI is preferred.
Clinical diagnosis in the emergency room will always play the main role in evaluating headaches. Identification of red flags and referral for imaging are key to decreasing morbidity and mortality in secondary headache disorders. We would conclude that in the study of fatal headaches, the presence of one of the three statistically significant red flag features should warrant prompt neuroimaging in the form of CT scan, followed by lumbar puncture if imaging is non-diagnostic. Using red flag features as a screening method for neuroimaging has been highlighted in a number of studies (3,4,8) in evaluating secondary causes of headache, and from our data, we would agree with using these clinical signs and symptoms in ascertaining high-risk patients. As the majority of cases of fatal headaches in our population were comprised of severe vascular events and large primary brain tumors/cysts, CT scan would be the most sensitive imaging modality in an emergency setting. Those SAH and tumor cases who had CT scans either in the emergency setting or just after hospital admission were all positive, which is not surprising considering the severity of their cases and their ultimate demise. These numbers, however, were low, and echo the findings of a retrospective study in the UK from Locker et al., who found an underuse of CT in alert, Glasgow coma scale (GCS) ≥ 14 patients who presented with abnormal neurological exams or first or “worst” headache (10). They cite the possible frequent occurrence of headache in the general population, as well as a lack of knowledge and inaccurate diagnoses, as leading to serious inadequacies in thoroughly investigating these patients. Despite the now increasing availability of after-hours MRI, CT scan is still the most efficient way to rule out more catastrophic and imminently fatal causes of headache, such as hemorrhage and tumors, and likely will be positive in such instances. In our study population, a large proportion of cases had no imaging, because of either initial misdiagnosis/improper triage or non-availability of after-hours imaging in the earlier years of the study period. After CT scan, MRI/CT angiography for suspected aneurysms/AVMs, and MR venography in suspected venous thrombosis, could be considered.
Age alone is a significant red flag feature, particularly at the extremes of age: >50 years and <10 years (5). There was a strong correlation found with advanced age and fatal headache in this study (Figure 2). In this older cohort, co-morbidities such as hypertension, diabetes and heart disease increase, with over one-quarter of cases found to have one or more. This further adds to complications and higher rates of mortality. In the younger age groups, the number of cases were less powered to infer statistical significance both in the prevalence of certain red flag features, and ultimate cause of headache found at autopsy. Using 40 years as a dividing line between “old” and “young”, one etiology, SVT, occurred exclusively in the younger population. As well as demonstrating a predilection of SVT for the younger age group, SVT findings illustrated that gender is an important consideration, and highlighted a particularly strong association between certain red flags and SVT, thus helping triage and urgently investigate this particular constellation of symptoms: prolonged occipital headache and progressive focal neurological deficit. Along with SVT, ruptured SAH was noted to occur more frequently in women than men, with a ratio of 3:1.
Time interval between headache onset and death was one aspect that unfortunately, due to inconsistencies found with the retrospective nature of record review, we were unable to evaluate more accurately. It would have been extremely useful from a clinical point of view to highlight by etiology the time intervals between headache onset and death. In the majority of cases, exact time of death was unclear; a small proportion were discovered a number of days later either at home or in the outdoor environment, while a proportion of cases admitted to the hospital were placed on ventilatory support varying from days to weeks before death following withdrawal of artificial life support. The important point for clinicians, however, is that the cases reviewed were not so abrupt or catastrophic as to cause immediate death. Patients still presented in time for a history and examination. Whether a patient dies an hour into hospital arrival with a colloid cyst rupture, for example, or a week later from an SAH, should not make a difference to the way we triage these patients in firstly identifying red flag features of their headache and then referring for appropriate emergency diagnostic imaging. Etiology of the headache would ultimately make a difference to therapeutic options and mortality, but this was beyond the scope of this autopsy study.
Due to the retrospective nature of the study and the lack of a standardized documentation system in many emergency rooms during the study period, we are likely underestimating the number of fatalities that may have presented initially with headache. Additionally, we do not consider those who never attended an emergency room or had any medical intervention for the acute catastrophic events that culminated in death. Furthermore, secondhand historical testimonies of symptoms from family or friends prior to death, where medical attention was not sought, was disregarded due to the unreliability and poor validation of information. Total case numbers and associated red flag features are therefore likely underestimated. However, the cases that were reviewed give us a reasonably broad and true representation of the cases that do present to emergency rooms, and ultimately represent the expected patient profile that clinicians should be most adept with evaluating.
Headache is a common, often alarming presentation. While most cases are benign in nature, some may herald a more sinister etiology. Documenting so-called red flags on initial presentation is crucial to acutely identify and treat those patients at highest risk of secondary headache. Overall, there is an improving trend among clinicians in recognizing and initiating appropriate interventions in these patients, likely based on increasing awareness of particular red flag features and on major advances made in the availability of neuroimaging.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest
The authors have no disclosures or sources of support to report.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.