
Abstract
Background
Migraine is a neurological disease involving recurrent attacks of moderate-to-severe and disabling head pain. Worsening of pain with routine physical activity during attacks is a principal migraine symptom; however, the frequency, individual consistency, and correlates of this symptom are unknown. Given the potential of this symptom to undermine participation in daily physical activity, an effective migraine prevention strategy, further research is warranted. This study is the first to prospectively evaluate (a) frequency and individual consistency of physical activity-related pain worsening during migraine attacks, and (b) potential correlates, including other migraine symptoms, anthropometric characteristics, psychological symptoms, and daily physical activity.
Methods
Participants were women (n = 132) aged 18–50 years with neurologist-confirmed migraine and overweight/obesity seeking weight loss treatment in the Women’s Health and Migraine trial. At baseline, participants used a smartphone diary to record migraine attack occurrence, severity, and symptoms for 28 days. Participants also completed questionnaires and 7 days of objective physical activity monitoring before and after diary completion, respectively. Patterning of the effect of physical activity on pain was summarized within-subject by calculating the proportion (%) of attacks in which physical activity worsened, improved, or had no effect on pain.
Results
Participants reported 5.5 ± 2.8 (mean ± standard deviation) migraine attacks over 28 days. The intraclass correlation (coefficient = 0.71) indicated high consistency in participants’ reports of activity-related pain worsening or not. On average, activity worsened pain in 34.8 ± 35.6% of attacks, had no effect on pain in 61.8 ± 34.6% of attacks and improved pain in 3.4 ± 12.7% of attacks. Few participants (9.8%) reported activity-related pain worsening in all attacks. A higher percentage of attacks where physical activity worsened pain demonstrated small-sized correlations with more severe nausea, photophobia, phonophobia, and allodynia (r = 0.18 – 0.22, p < 0.05). Pain worsening due to physical activity was not related to psychological symptoms or total daily physical activity.
Conclusions
There is large variability in the effect of physical activity on pain during migraine attacks that can be accounted for by individual differences. For a minority of participants, physical activity consistently contributed to pain worsening. More frequent physical activity-related pain worsening was related to greater severity of other migraine symptoms and pain sensitivity, which supports the validity of this diagnostic feature.
Study protocol
ClinicalTrials.govIdentifier: NCT01197196
Migraine is a primary headache disorder defined by having at least five attacks that last 4–72 hours, with clinical features including unilateral location, pulsating quality, moderate or severe pain intensity, nausea/vomiting, photophobia, phonophobia, and aggravation by or causing avoidance of routine physical activity (PA) (1). This latter feature has received less attention than other diagnostic criteria. A survey examining diagnostic practices in American Headache Society members found that pain worsening with routine PA during migraine attacks was the only diagnostic criterion that was deemphasized by practitioners when evaluating and diagnosing migraine (2).
The above is concerning, given the positive role of regular PA and aerobic exercise in the management of migraine (3,4) and low documented levels of daily PA in individuals with migraine relative to those without (5,6). It is possible that individuals who report that pain is worsened by PA may tend to avoid PA, which results in lower daily PA and exercise levels. A similar behavioral pattern often occurs in individuals who report PA as a trigger for migraine (7,8) and use PA avoidance as a migraine prevention strategy (9).
Along with receiving less attention in clinical practice than other symptoms that accompany migraine, pain worsening with PA during attacks has also received comparatively less empirical attention. Early studies document that nearly all patients with migraine (95–100%) retrospectively report worsening of migraine with routine PA (10–12), although reliance on retrospective measurement limits the validity and reliability of these estimates. We are aware of only one small prospective study that found that 68% of women with overweight/obesity reported at least one attack in which routine PA exacerbated migraine pain (5), suggesting that this clinical feature may be less prevalent than previously documented in retrospective studies. Of note, no studies have prospectively examined the frequency and consistency of PA-related pain worsening across migraine attacks, or examined correlates of this feature. In short, despite its role as a diagnostic criterion, worsening with PA is a poorly understood feature of migraine.
Therefore, in the current study, we utilized prospective daily diary data from women with migraine and overweight/obesity who were enrolled in a weight loss intervention study to examine both the overall frequency and individual consistency of pain worsening with PA across multiple attacks over a 28-day baseline period prior to treatment. As a secondary aim, we evaluated factors that could be potentially associated with PA-related pain worsening, including other migraine symptoms, weight status, allodynia, depression and anxiety, and daily total PA levels. We hypothesized that: (a) the frequency of PA-related pain worsening would be lower than previously documented in retrospective studies and (b) PA-related worsening would be positively associated with other migraine characteristics and disability. Based on the absence of existing empirical prospective data, the test of the associations between PA-related pain worsening with psychological symptoms, weight status, and objectively-measured PA levels were exploratory.
Method
Participants and procedure
Participants were women (n = 132) aged 18–50 years with neurologist-confirmed migraine and overweight/obesity (BMI = 25.0–49.9 kg/m2) seeking treatment to lose weight and decrease their headaches in the Women’s Health and Migraine (WHAM) trial (13). After providing written informed consent, women completed a baseline assessment that included objective measurement of height and weight and self-reported questionnaire assessment of headache, psychosocial, and demographic characteristics. Next, women began recording their headache activity for 28 consecutive days, consistent with monitoring periods used in clinical practice, which was completed using a smartphone headache diary. Subsequently, women completed a 7-day period of objective monitoring of PA. Thus, PA-related pain worsening and objective measurement of PA were not concurrently assessed. All measures were completed before randomization and initiation of treatment. The current study included secondary analysis of baseline data. Cases were included in analyses on the basis of having completed the smartphone headache diary and 7-day objective monitoring of PA. The study protocol was approved by the Rhode Island Hospital Institutional Review Board (Providence, RI, USA). All authors had full access to study data throughout data collection, analysis, and manuscript preparation. Authors (SGF, JGT, DSB) assume full responsibility for the integrity of the data.
Measures
Migraine characteristics and clinical features: A smartphone and accompanying web-based daily headache diary was used to assess headache activity daily for 28 consecutive days (13). Participants used the smartphone to record migraine attack occurrence (yes/no), maximum headache pain intensity (0 “no pain” to 10 “pain as bad as you can imagine”), duration (hours) and accompanying symptoms including pain worsening with PA (“Did the headache change with activity such as walking stairs? [Worse, Unchanged, Better]), and nausea, photophobia, and phonophobia (occurrence [yes/no] and severity [0–3]). Reports were stamped and recorded each day and in real time and were automatically transmitted to the research team. Each participant’s daily entries were summarized (averaged) at the end of the 28-day monitoring period.
Allodynia: The Allodynia Symptom Checklist (ASC-12), a 12 item self-report questionnaire, was administered at baseline before the headache monitoring period to assess the presence and severity of cutaneous allodynia symptoms during migraine attacks (14). ACS-12 scores of 0–2, 3–5, 6–8, and ≥9 indicate none, mild, moderate, and severe allodynia, respectively.
Migraine disability: The Headache Impact Test (HIT-6) is a six item self-report assessment of the extent to which headache impact on “usual daily activities”, pain severity, need for rest, fatigue, frustration, and difficulty with concentration (15). The HIT-6 was administered at baseline before the headache monitoring period. Higher HIT-6 scores indicate greater impact on normal everyday life and functional impairment.
Anthropometric measurement: Height was measured in millimeters using a wall-mounted Harpenden stadiometer (Holtain Ltd, Crosswell, Crymych, Pembrokeshire, UK). Weight was measured in light street clothing, without shoes, and to the nearest 0.1 kg using a calibrated digital scale (Tanita BWB 800; Tanita Corporation of America, Inc., Arlington Heights, IL, USA). BMI was calculated from these measures using the formula: BMI (kg/m2) = weight (kg)/(height [m])2.
Psychological characteristics: The Center for Epidemiologic Studies-Depression Scale (CES-D), a 10 item self-report questionnaire, was used to assess depressive symptoms in the past two weeks. Higher scores indicate greater symptom severity (16). CES-D scores ≥ 16 reflect clinically-elevated depressive symptoms. The Generalized Anxiety Disorder-7 (GAD-7), a seven item self-report questionnaire, was used to assess anxiety symptoms in the past two weeks (17). Higher scores reflect more severe anxiety symptoms. GAD-7 scores ≥ 10 reflect clinically-elevated anxiety symptoms. The Pain Catastrophizing Scale (PCS) is a 13 item measure of pain-related cognitions, which reflects the tendency of individuals to respond to pain with catastrophic thoughts (18). The PCS yields a total score with higher scores reflecting greater pain catastrophizing, with a score ≥ 30 reflecting clinically-elevated levels. These measures were collected at baseline before the headache monitoring period.
Total daily physical activity participation: The SenseWear Mini Armband monitor (SWA, BodyMedia Inc, Pittsburgh, PA) was used to objectively measure daily total PA participation during the 7-day period subsequent to the 28-day headache monitoring period. The SWA is a wireless multi-sensor monitor worn over the upper left triceps muscle that simultaneously integrates motion data from a triaxial accelerometer, physiologic metrics from multiple sensors (i.e. heat flux, galvanic skin response, and skin and near-body temperatures), and sex, age, body weight, and height information to estimate energy expenditure and intensity of activities using proprietary software algorithms (SenseWear Professional Software, version 7.0). Participants were asked to wear the SWA during all waking hours for seven consecutive days. The number of daily minutes spent in total PA was determined using metabolic equivalent (MET) values, with activities ≥ 1.5 METs classified as PA. For data to be considered valid, participants needed to have worn the SWA for ≥ 8 hours/day on ≥ 4 days during the 7-day assessment period.
Data analytic approach
Analyses were conducted in SAS v9.4. Daily records in which a migraine attack was reported were summarized within-person. The proportion of attacks in which PA resulted in each of its effects on pain (worsened, unchanged, improved) was computed within-person and reported as a percentage. Initial descriptive statistics were used to characterize the sample in terms of any occurrence (between-subject) and proportion of attacks (within-subject) in which worsening, unchanged, and improved pain was reported with PA (mean ± SD). The intraclass correlation coefficient (ICC) was calculated using a logistic model with random effect of participant to provide an indication of the degree to which variance in PA-related worsening of pain was attributable to individual differences (i.e. participant characteristics) versus unmeasured contextual factors likely occurring at the time of headache. Next, correlations were used to examine the association between the proportion of attacks characterized by PA-related pain worsening and study variables. Based on visual examination of the distribution of the proportion of attacks with PA-related worsening (see Figure 1), univariate quantile regression analyses (19) were used to examine the conditional association between study variables at varying proportions of PA-related worsening of pain. The 50th and 75th percentiles were specified, which corresponded to 25% and 64.1% of attacks in which worsening with PA occurred. Percentiles ≤ 25% were not reported given zero values (0% of attacks with worsening) in this portion of the distribution. Variables were converted into z-scores prior to model entry to derive standardized coefficients consistent with zero-order correlations. All tests of statistical significance were two-tailed. This study involved a secondary analysis of baseline data collected as part of a randomized controlled trial. For the randomized controlled trial (13), a sample of 140 participants was estimated to adequately power comparison of changes in monthly headache frequency between the behavioral weight loss intervention and migraine education control arms.
Histogram of within-subject reported proportion (percent) of attacks in which PA-related worsening occurred.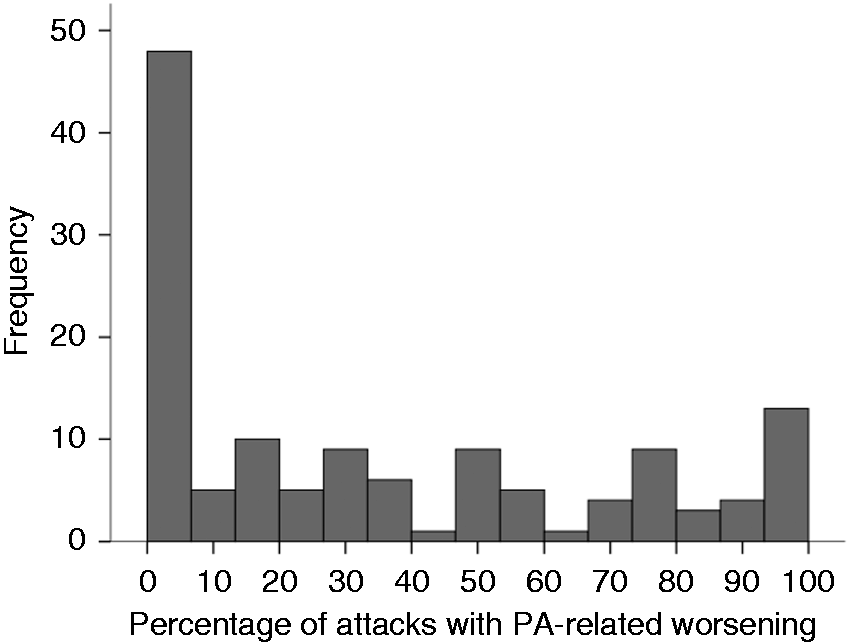
Results
Sample characteristics
Women (n = 132, average age 38.5 ± 8.1) were identified as white (76.5%), black (11.4%), or other/mixed race (12.1%); 18.9% identified as Hispanic. The majority of women were married (52.3%) or never married (25.0%) and completed at least some college (87.1%). Average BMI was 35.5 ± 6.6. An average of 5.5 ± 2.8 migraine attacks per 28 days were reported, with an average duration of 20.1 ± 15.9 hours with moderate maximum pain intensity (5.9 ± 1.5). The prevalence of chronic migraine in the sample was 12.1% (n = 16). On average, photophobia was reported during 66.7 ± 25.1% of migraine attacks, phonophobia during 61.5 ± 26.2% of attacks, nausea during 38.2 ± 28.8% of attacks, and aura with 15.9 ± 26.2% of attacks.
Reported effect of PA on pain
The distribution of the proportion of attacks characterized by worsening of pain with physical activity is illustrated in Figure 1. Results indicated high within-person consistency in reporting PA-related pain worsening (ICC = 0.71, CI95% = 0.62 – 0.78). The within-person consistency is reflected in the two tails of the distribution (Figure 1), in which about half of the sample consistently reported the presence or absence of PA-related worsening during attacks.
Between-subject effects: Approximately two-thirds of women (63.6%) reported at least one attack in which PA contributed to worsening of pain. Most women (90.2%) reported at least one attack in which pain was unchanged by PA, and 10.6% of women reported at least one attack in which pain improved with PA.
Within-subject effects: As illustrated in Figure 1, 36.4% (n = 48) of participants did not report any attacks during the 28-day monitoring period in which PA worsened pain. A small number of participants (9.8%, n = 13) reported worsening of pain with PA during all attacks (100%). The average proportion of attacks where PA was reported to worsen, improve, or not impact pain, which gives each participant equal weight regardless of the number of attacks they experienced, is presented in Figure 2. On average, PA contributed to worsening of pain in 34.8 ± 35.6% of attacks, had no effect on pain in 61.8 ± 34.6% of attacks, and improved pain in 3.4 ± 12.7% of attacks.
Frequency of worse, unchanged, and improved migraine from PA.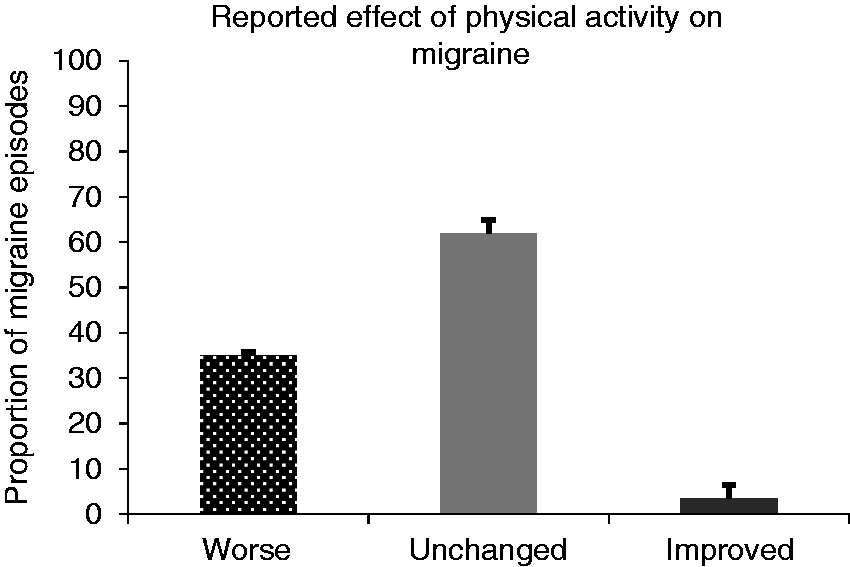
Correlates of PA-related pain worsening
Sample characteristics and correlates of worsening attack with PA.

p < 05, **p < .01
The magnitude of the correlations between study variables were examined for women low (25% of attacks) and high on proportion of attacks characterized by PA-related pain worsening (64.1% of attacks), which corresponded to the 0.50 and 0.75 quantiles, respectively (see standardized values in Table 1). Similar-sized magnitudes of associations emerged at the 0.50 and 0.75 quartiles of the proportion of attacks with PA-related worsening and clinical features. PA-related worsening of pain was conditionally associated with higher BMI at the upper quartile of worsening attacks proportion (p = 0.02).
Discussion
The interplay between migraine and PA is complex and remains understudied (3). There is a surprising dearth of literature on worsening of pain with PA during attacks, a clinical and diagnostic feature of migraine. The current study is the first to prospectively evaluate the overall frequency and individual consistency of this feature across multiple migraine attacks.
There is large variability in the impact of PA on pain during migraine attacks that can be accounted for by individual differences. In the current sample of women with migraine and overweight/obesity, approximately two-thirds of women reported at least one attack characterized by worsening with routine PA during the 28-day monitoring period. This is in contrast to prior retrospective studies that have documented the presence of this feature in nearly all individuals with migraine (10–12). The observed discrepancy is not surprising given the well-documented inconsistencies between retrospective and prospective reporting of migraine symptoms and features (20–23). There is also evidence of significant heterogeneity in PA’s effect on pain during an attack: Nearly all women with migraine reported at least one attack in which PA did not change pain and 10.6% of women had at least one attack in which PA improved pain. Additionally, approximately one in every three attacks was characterized by worsening with PA. There appears to be a sub-set of individuals with migraine that do not (or very rarely) experience PA-related pain worsening and another sub-set of individuals that experience this on an occasional or more frequent basis. This pattern of findings is consistent with conceptualization of PA-related pain worsening as a diagnostic criterion in that some, but not all, individuals with migraine have this symptom during attacks.
We also uniquely examined potential correlates of PA-related pain worsening during migraine attacks. Results showed that a higher proportion of attacks involving PA-related pain worsening demonstrated small-sized associations with more severe clinical features, including nausea, photophobia, phonophobia, and allodynia. The magnitude of these associations was comparable at both the lower and upper quartiles of the proportion of attacks with worsening pain with PA. Thus, individuals with migraine who report a higher proportion of attacks in which pain is exacerbated by PA may, to a minimal extent, also experience more severe associated features (i.e. photophobia, phonophobia) and central pain sensitivity. The clinical significance of these small-size correlations is unknown. Nevertheless, the current findings provide novel evidence that worsening with PA corresponds with other clinical features of migraine, which further supports its validity as a clinical feature. Notably, exacerbation of pain with PA is distinct from other clinical features in that it reflects worsening rather than development of pain (24,25). This may explain why worsening with PA has been de-emphasized in the literature (24) and in clinical practice (2).
It is also worth noting that BMI was uniquely associated with worsening with PA when at the top quartile of proportion of attacks with worsening (≥64.1% of attacks). Individuals with migraine who typically experience aggravation of pain from routine PA may tend to avoid PA and aerobic exercise, resulting in low energy expenditure. However, consistent with one prior study (5), we did not find an association between the proportion of attacks with PA-related worsening with objectively-measured levels of PA. Thus, worsening of pain with routine PA does not appear to be related to actual levels of PA when subsequently monitored. Future research is needed to determine the directionality of the association between poor weight control and high frequency of worsening of pain from routine PA. Concurrent and objective measurement of PA during migraine attacks would permit examination of the acute impact of migraine on daily PA (and vice versa), which would bolster future work.
The current study has important strengths and points of innovation. It provides novel evidence of the overall frequency of PA-related pain worsening during migraine attacks. Through use of a prospective assessment period via headache diaries (reporting migraine occurrence, pain, and associated features), measurement error and the low validity inherent in retrospective recall was minimized. PA-related pain worsening was also assessed on a per-migraine basis across multiple migraine attacks. This permitted an empirical examination of the degree of individual consistency in reporting this feature.
Our findings should also be viewed in the context of certain limitations. First, this sample was comprised of women of reproductive age with overweight and obesity, a vulnerable subset of individuals with migraine given that obesity might be an exacerbating factor for migraine (26–29). In particular, women with overweight/obesity experience greater discomfort during physical activity relative to women with normal weight (30). Therefore, it is possible that women with overweight/obesity and migraine may experience greater pain worsening from physical activity compared to women with migraine and normal weight. This is an empirical question that warrants attention in subsequent studies. Future research that examines the frequency of migraine worsening with PA among a more diverse sample of migraine patients is recommended to strengthen the generalizability of the findings. Second, participants reported headache activity at the end of each attack within the day, limiting the ability to evaluate the temporal sequence of effects, or the effects of PA-related pain worsening on other migraine characteristics and clinical features over time. Objective measurement of PA during migraine attacks is needed to understand the acute effect of PA on migraine pain. Future studies utilizing experimental designs are needed to determine the directionality of the observed associations and to examine the acute within-day and next-day effects of PA-related worsening of pain. Third, the language used to query participants about on the effect of routine PA on pain during migraine attacks was intended to reflect the wording used in the ICHD diagnostic criteria (1). Thus, the current study did not consider the “dose” of PA and how it impacted pain. Future work in this arena should consider how different characteristics of PA (occurrence, type, intensity, or duration) influence migraine pain worsening. Of note, pain that causes avoidance of routine PA is coupled with PA-related pain worsening as a diagnostic criterion (i.e. “aggravation by or causing avoidance of routine physical activity”), although these features are phenotypically distinct. Additional research is recommended to further explore the nature of migraine-related avoidance of PA. Fourth, consistent with routine clinical monitoring, the headache diary monitoring period was 28 days. Future studies that utilize a longer monitoring period will have increased ability to detect patterning and variability in PA-related pain worsening over time. Last, there are likely unmeasured factors that correlate with and impact on the likelihood of pain worsening with PA during attacks. For example, several cognitive-affective processes may directly or indirectly influence PA’s impact on migraine, including beliefs (expectancies) about the effects of PA on migraine (31), fear and catastrophizing of pain and bodily sensations (i.e. anxiety sensitivity) (32–36) and pain-related attentional bias (37).
Conclusions
Findings support the validity of PA-related pain worsening as a diagnostic feature of migraine: (a) This feature occurred in many (63.6%), but not all individuals with migraine and overweight/obesity; (b) a minority of participants (<10%) consistently reported PA-related pain worsening in all attacks, whereas a sizeable proportion of individuals do not (or very rarely) report this feature; (c) the variability in PA-related pain was largely attributable to individual difference factors and not unmeasured contextual factors; and (d) more frequent PA-related pain worsening was related to greater severity of other migraine symptoms and allodynia, which were small-sized associations. Overall, patients with migraine should be encouraged to capitalize on migraine-specific and general health-related benefits of regular PA participation (3,4). A minority of individuals with migraine who consistently experience PA-related pain worsening may require tailored interventions to assist in increasing PA and exercise. These individuals may benefit from gradual exposure to PA and aerobic exercise to increase engagement in PA (38,39). Future research is needed to examine the acute effects of PA on pain during migraine attacks, explicate the characteristics of routine PA (type of activity, intensity, duration) that increase the likelihood of worsening pain during migraine, and identify cognitive-affective factors that contribute to within-person variability in the frequency of occurrence of PA-related pain worsening, which can be targeted in cognitive-behavioral interventions (38,40,41).
Article highlights
Worsening of pain with routine physical activity during attacks is a principal migraine symptom, although is poorly understood. Worsening of pain with routine physical activity was reported in many (63.6%) but not all women with migraine and overweight/obesity. A minority of participants (< 10%) consistently reported physical activity-related pain worsening in all attacks, whereas a sizeable proportion of individuals did not (or very rarely) report this feature. More frequent worsening of pain with physical activity was related to greater severity of other migraine symptoms and allodynia, which supports the validity of this feature of migraine. There is large variability in the impact of physical activity on pain worsening during migraine attacks, which is primarily accounted for by individual differences and not unmeasured contextual factors.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J Graham Thomas received research support from the National Institutes of Health (NIH) R42 DK103537 (principal investigator), R01 DK095779 (principal investigator), R41 HL114046 (principal investigator), R01 NS077925 (co-investigator), and Weight Watchers International Inc, and serves as a consultant to Applied VR, KetoThrive, and Weight Watchers International Inc. Ana M Abrantes received research support from the National Institutes of Health (NIH) R21 CA214102 (multiple principal investigator), R01 CA173551 (principal investigator, R01 NR014540 (co-investigator), R01 HL127695 (multiple principal investigator), R34 AA024295 (principal investigator), R21 DA041153 (multiple principal investigator), R21 DA041553 (multiple principal investigator), and R01 NR015977 (co-investigator). Jelena Pavlovic received consulting honoraria from Allergan Inc. Richard B Lipton received research support from the NIH (PO1 AG03949 (program director), PO1AG027734 (project leader), RO1AG025119 (investigator), RO1AG022374-06A2 (investigator), RO1AG034119 (investigator), RO1AG12101 (investigator), the National Headache Foundation, and the Migraine Research Fund; serves on the editorial board of Neurology and as senior advisor to Headache; has reviewed for the National Institute on Aging (NIA) and National Institute of Neurological Disorders and Stroke (NINDS), holds stock options in eNeura Therapeutics, and serves as consultant, advisory board member, or has received honoraria from: Allergan, the American Headache Society, Autonomic Technologies, Boston Scientific, Colucid, Eli Lilly, Endo, eNeura Therapeutics, Novartis, and Teva. Todd A Smitherman serves as a consultant for Alder Biopharmaceuticals. Dale S Bond received research support from the NIH, R01 NS077925 (principal investigator), R01 DK108579 (multiple principal investigator), R01 DK112487 (co-investigator), R01 DK112585 (co-investigator), R03 DK114254 (co-investigator), travel support from the American Headache Society, and serves as a member of the Slimming World, Inc. Special U.S. advisor group. Samantha G Farris, Julie Roth, Megan A Irby, Donald B Penzien and Kevin O’Leary declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institute of Neurological Disorders and Stroke (R01-NS077925; PI: Bond) and the first author is supported by a grant from the National Heart, Lung, and Blood Institute (T32-HL076134-11; PI: Wing).