
Abstract
The aim of this study was to evaluate, using a prospective and a cross-sectional design, the relationship between level of physical activity and migraine and non-migraine headache. In the prospective part, 22 397 participants, not likely to have headache, answered questions about physical activity at baseline (19841986) and responded to a headache questionnaire at follow-up. In the cross-sectional part (1995-1997), 46 648 participants answered questions about headache and physical activity. Physically inactive individuals at baseline were more likely than active individuals to have non-migraine headache 11 years later (odds ratio 1.14, 95± confidence interval 1.02, 1.28). In the cross-sectional analyses, low physical activity was associated with higher prevalence of migraine and non-migraine headache. In both headache groups, there was a strong linear trend (P< 0.001) of higher prevalence of ‘low physical activity’ with increasing headache frequency. The result may indicate that physical inactivity among headache-free individuals is a risk factor for non-migraine headache and that individuals with headache are less physically active than those without headache.
Introduction
Headache is a general health problem causing individual suffering as well as societal expense (1). The 1-year prevalence for headache in Norway is 38% (46% in women and 30% in men) (2). Globally, 11–13% of the adult population suffer from active migraine, and the majority report a negative impact on leisure activities, family life and working capacity (2–4). Optimal treatment is crucial, and non-pharmacological strategies are often recommended. Examples of such strategies are changes in lifestyle in order to avoid triggers, relaxation therapy, acupuncture and exercise (5–7).
Regular exercise has been suggested as a method of migraine management with a beneficial effect on both frequency and intensity, as well as on the duration of the attacks and patient well-being (8–11). On the other hand, headache can be provoked by physical exercise (12, 13). Hard physical exercise and lack of warm-up can trigger not only tension-type headache (TTH), but also in some cases migraine attacks (14, 15). A recent report has suggested a model of exercise for untrained patients with migraine that can increase maximum oxygen uptake without increasing the number of migraine attacks (16).
Our knowledge about headache and physical activity is limited, and few population-based studies have evaluated this relationship. In a large Canadian study, migraine did not have a deleterious effect on recreational activity levels among adolescents, but no data about frequency and intensity of migraine attacks was presented (17). Most previous studies evaluating the influence of physical exercise on headache are case–control studies. For example, Neususs et al. (18) reported that patients with headache had less aerobic endurance and flexibility than healthy controls. The prevalence of migraine was also found to be lower among 791 first-division basketball players in the USA than in the general population (19). However, it is unclear whether these basketball players are historical migraineurs who have become attack-free, or whether migraine is an obstacle to playing basketball at this level. This potential problem with selection bias is less likely in population-based studies evaluating the influence of physical exercise on migraine.
Using the data of one of the world's largest epidemiological studies, the Nord-Trøndelag Health Survey (HUNT), we aimed to evaluate, using a prospective design, the relationship between level of physical activity at baseline and subsequent risk for migraine and non-migraine headache. A secondary aim was to evaluate the cross-sectional association between physical activity and frequency of migraine and non-migraine headache.
Materials and methods
Participants
All inhabitants, ≥ 20 years old, in Nord-Trøndelag county of Norway were invited to participate in the Nord-Trøndelag Health Surveys, HUNT 1 (1984–1986) and HUNT 2 (1995–1997).
The main purpose of HUNT 1 was to study blood pressure, diabetes mellitus and factors of lifestyle, and 74 599 (88%) of the potential participants underwent a health survey and answered a questionnaire that was sent to them. Questions about level of physical activity were also included in the questionnaire. There were no specific questions concerning headache. However, headache status was indirectly established through a question about the use of analgesics during the last month, which 59 471 persons answered. A total of 41 581 individuals said they had not taken analgesics and were defined as a relatively headache-free population (20, 21). Of these, 33 694 were available for the follow-up study, HUNT 2, of whom a total of 22 397 (66%) had answered both the headache questions and at least one of the questions about physical activity in HUNT 1. A total of 15 411 (68%) answered all three questions about physical activity. Regarding HUNT 1, a detailed description of the study population, including participants and non-participants, has previously been published (22). The study population from HUNT 1, eligible for the present study, is described in Fig. 1.

Diagram of the study population, prospective study.
HUNT 2 was more extensive and contained > 200 health-related questions, including questions about both headache and level of physical activity. A total of 51 383 (56%) individuals of the 92 566 participants answered the questions about headache. Of these, 46 648 (91%) answered at least one of the questions about physical activity.
Headache diagnosis
In HUNT 2, 13 of the questions were about headache, as has previously been described in detail (23). The questions about headache clarified whether or not a participant had headaches, whether there were migraines, and frequency. Participants who answered ‘yes’ to the question about headache during the last 12 months were classified as suffering from headache. Based on the 12 remaining questions, they were then classified into subgroups: migraine or non-migraine headache. Headache not fulfilling the criteria for migraine was classified as non-migraine. Based on questions about the frequency of headache, the sufferers were divided into three groups: < 7 days/month, 7–14 days/month and > 14 days/month. The diagnostic method, a modified version of the current International Headache Society criteria, has been validated based on clinical interviews. Briefly, the positive predictive value for migraine was 84% and for non-migraine headache 68%. The negative predictive value was 78% for migraine and 76% for non-migraine headache (23).
Assessment of physical activity
In HUNT 1 the participants answered three questions about physical activity (frequency, duration, and intensity). Based on the question about frequency, the patients could be classified as active or inactive (24) (see Fig. 2).

Questions about physical activity in HUNT 1.
In HUNT 2, the questions about physical activity were repeated, but altered in several respects. First, physical activities were measured not only at present, but during the last year. Second, participants reported the number of hours per week at different intensities of exercise, i.e. ‘light’ physical activity (without being out of breath or breaking into a sweat) and ‘hard’ physical activity (push until out of breath or break into a sweat). These questions concerned only leisure time. Based on these answers, the patients could be classified into groups of low, medium and high physical activity (24) (see Fig. 3).

Questions about physical activity in HUNT 2.
Ethics
This study was approved by the Regional Committee for Ethics in Medical Research, and the HUNT study was also approved by the Norwegian Data Inspectorate.
Data analysis
We evaluated the influence of physical activity reported in HUNT 1 and HUNT 2 on headache, including migraine, using logistic regression analysis with odds ratio (OR) and 95% confidence interval (CI) as measures of association. Potential confounding was evaluated by adjusting for sex and age. Other potential factors such as education, smoking, level of physical activity at work (cross-sectional study only), and body mass index were also evaluated, but excluded from the final analyses because they changed the OR by < 0.05. When appropriate, headache frequency categories were treated as a continuous variable and incorporated into a two-sided test for trends, to evaluate the probability of a linear relationship between headache frequency and low physical activity. Data analysis was performed with SPSS for Windows version 14.0 (SPSS Inc., Chicago, IL, USA).
Results
Physically inactive individuals at baseline in 1984–1986 were more likely to have non-migraine headaches 11 years later (OR 1.14, 95% CI 1.02, 1.28) than individuals who exercised at baseline. In contrast, migraine tended to be less likely to appear later in life among physically inactive persons (OR 0.85, 95% CI 0.70, 1.03). The frequency or duration of physical activity showed no relation to migraine or non-migraine headache, whereas high-intensity activity (‘practically until exhaustion’) was associated with a higher prevalence of migraine but not non-migraine headache 11 years later. This was true for women but not for men (Table 1).
The prospective part of the study: prevalence odds ratio (OR)∗ for migraine during HUNT 2 at different levels of intensity of physical exercise during HUNT 1 in women
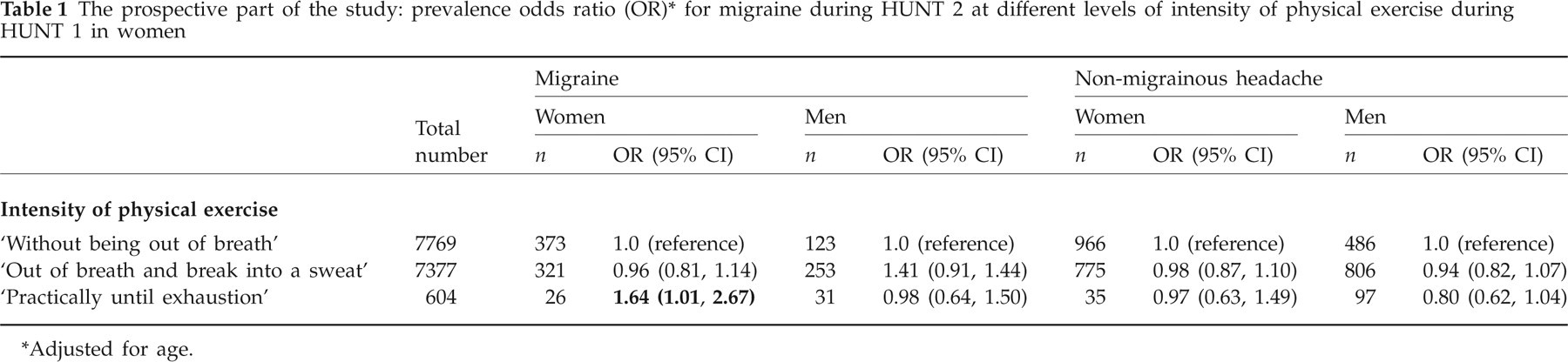
Adjusted for age.
In the cross-sectional part of the study, low physical activity was associated with higher prevalence of migraine and non-migraine headaches (Table 2).
The cross-sectional part of the study (HUNT 2): prevalence odds ratio (OR)∗ for headache at different activity levels

Adjusted for sex and age.
In both headache groups, there was a strong linear trend (P < 0.001) towards higher prevalence of ‘low physical activity’ with increasing headache frequency (Table 3).
The cross-sectional part of the study (HUNT 2): prevalence and odds ratio (OR)∗ of low physical activity related to frequency of headache

Adjusted for sex and age.
Discussion
To the best of our knowledge, this is the first prospective study evaluating the influence of physical activity on the occurrence of migraine and non-migraine headache. The results of the prospective part of the study indicated that physical inactivity at baseline was associated with a higher risk of non-migraine headache 11 years later. In the cross-sectional part of the study, a low level of physical activity was consistently associated with higher prevalence of migraine and non-migraine headache. The reported headache frequency had a greater impact on this association than the diagnosis itself.
Our results differ from previous population-based cross-sectional studies reporting no association between migraine and physical activity (17, 25). Although not significant, physical inactivity at baseline tended to be associated with a lower risk of migraine at follow-up. The reason for this is unclear. However, physical activity is a well-known trigger of migraine (13) and, theoretically, avoiding exercise may reduce the risk of activating a migraine. The potentially ‘harmful’ effects of exercise were illustrated by the fact that high intensity of training ‘practically until exhaustion’ in women was associated with an increased risk of developing migraine later in life.
Physical inactivity appears to have different effects on migraine and non-migraine headache, based on the finding that physical inactivity at baseline was associated with greater risk of non-migraine headache. In our validation study, TTH was found to be the most common headache type (80%) among patients with non-migraine headache (23). A finding that may be relevant from a cross-sectional study in Denmark (25) was that men who reported low physical activity also had a higher prevalence of TTH. In our cross-sectional part of the study it was consistently found that a low level of physical activity was associated with higher prevalence of migraine and non-migraine headache, and, for both headache types, the prevalence of low physical activity increased with increasing headache frequency.
In cross-sectional studies the relationship between cause and effect cannot be determined. One possible explanation for the association between low physical activity and a high prevalence of migraine and non-migraine headache is that headache is a reason for being less physically active. This fact is supported by a study about TTH and physical activity, which concluded that TTH negatively affects patients' levels of physical activity (26). It is possible that people with migraine avoid exercise, since it is a migraine trigger, and therefore are less active. One should, however, also be open to the opposite possibility, that regular physical activity may, at least to some extent, prevent headache or reduce headache frequency (7–10). However, randomized controlled studies are needed to evaluate this.
The strengths of this study are the large unselected population and the use of validated headache diagnoses and validated questions concerning physical activity. However, there are also limitations that must be taken into account. No questions about headache were included in HUNT 1, and headache status at baseline is therefore indirectly defined using information on the use of analgesics. We have assumed that participants reporting ‘never’ to the question about use of pain-relieving medication during the past month were unlikely to have headaches (20, 21). Although some patients with headache do not use acute medication (27–31), it is reasonable to assume that respondents who did not use analgesics have very few if any problems with headaches, compared with the general population. Another limitation is that the questionnaire-based headache diagnoses were not optimal compared with interview diagnoses (23). There is a possibility of non-differential misclassification of diagnosis, which may weaken real associations. Generalization of our results must be made with caution. Although the respondent rate was acceptable, we cannot rule out the possibility of selection bias.
Conclusions
Total inactivity among headache-free individuals is a risk factor for non-migraine headache. In the cross-sectional study we found that individuals with migraine and non-migraine headache are less physically active than those without headache. Frequency of headache has a greater impact on physical activity than the type of headache.
Acknowledgements
Special thanks to James Varkey and Pernilla Jonsson for support during the study. The authors received financial support from Praktikertjänst AB, Stockholm, Sweden and the Renee Eanders Fond, Sweden. The Nord-Trøndelag Health Study (The HUNT study) is a collaboration between The HUNT Research Centre, Faculty of Medicine, The Norwegian University of Science and Technology (NTNU); The Norwegian Institute of Public Health; and the Nord-Trøndelag County Council.