
Abstract
Introduction
The term Tolosa-Hunt Syndrome was first used more than half a century ago to describe painful ophthalmoplegia accompanied by cranial nerve palsies. In the decades since, its diagnostic criteria have evolved considerably. The beta version of the 3rd Edition of the International Classification of Headache Disorders narrows these criteria to require the demonstration of granulomatous inflammation on MRI or biopsy. We believe this may introduce challenges to accurate diagnosis.
Discussion
Requiring the demonstration of granulomatous inflammation for a diagnosis of Tolosa-Hunt Syndrome may introduce the potential for false negative and false positive diagnoses. Although the disorder presents secondary to granulomatous inflammation, MRI technology may not be able to identify it reliably, and biopsy is not always indicated for its symptomatology. Additionally, several cases have been reported of Tolosa-Hunt Syndrome diagnosed with MRI-confirmed granulomatous inflammation that later prove to be attributable to other pathologies. The emphasis on neuroimaging may therefore exclude some true Tolosa-Hunt Syndrome cases and include others resulting from other latent pathologies that are not visible on MRI.
Conclusion
We wish to offer several potential modifications to the International Classification of Headache Disorders guidelines for Tolosa-Hunt Syndrome, including making the demonstration of granulomatous inflammation on MRI or biopsy non-mandatory and lengthening patient follow-up to two years for cases in which MRI is unrevealing.
Keywords
Introduction
The term Tolosa-Hunt Syndrome (THS) first appeared in the literature in 1966. In their seminal paper, Smith and Taxdal combined cases observed separately by Drs. Tolosa and Hunt to define THS as painful ophthalmoplegia accompanied by cranial nerve palsies that responded to corticosteroid therapy within 48 hours (1). Although the etiology of THS remains unknown, its diagnostic criteria have evolved significantly since their early description (2–4).
Previous diagnostic criteria for Tolosa-Hunt Syndrome
In the first edition of the International Classification of Headache Disorders (ICHD), published in 1988, diagnosis of THS was indicated by unilateral orbital pain associated with paralysis of one or more of the III, IV, and VI cranial nerves that was relieved within 72 hours after initiation of corticosteroid therapy, and with the exclusion of other causative lesions by neuroimaging and carotid angiography (2). Although this largely followed the criteria laid out by Smith and Taxdal, the ICHD’s last criterion crucially defined THS as a diagnosis of exclusion. The second edition of the ICHD, published in 2004, used a nearly identical description (3). In 2013, however, the definition of THS was significantly narrowed with the publication of the beta version of the third edition of the ICHD (4).
Tolosa-Hunt Syndrome in the era of magnetic resonance imaging
The most recent ICHD-3 beta criteria require, in addition to the above, the presence of granulomatous inflammation of the cavernous sinus, superior orbital fissure, or orbit, as demonstrated by magnetic resonance imaging (MRI) or biopsy, for a diagnosis of THS (4). In general, improved specificity is beneficial to a definition. Nevertheless, in the case of THS we believe that this change may introduce two diagnostic problems.
First, given the complexity and heterogeneity of its underlying pathology, THS can present with an unremarkable MRI; the emphasis on neuroimaging therefore may exclude some THS cases. Second, granulomatous inflammation in the absence of other MRI findings is likely insufficient to diagnose THS; the emphasis on neuroimaging may also include cases that do not have THS and instead result from other latent pathologies that are not visible on MRI.
In this report and focused review of the literature, we describe evidence supporting each of these lines of thinking and conclude with revision suggestions for the diagnostic criteria of Tolosa-Hunt Syndrome.
False negative diagnoses of Tolosa-Hunt Syndrome
Although studies dating as early as Tolosa’s 1954 paper suggest that THS is secondary to granulomatous inflammation (1,5–7), even modern MRI technology may not be able to identify it reliably.
THS with normal MRI
In their 2015 paper, Abdelghany et al. present a representative case of THS accompanied by an unremarkable MRI. They describe a 60-year-old woman with a history significant for end-stage renal disease and non-Hodgkin’s lymphoma who presented with unilateral headache, painful ophthalmoplegia, ptosis, and confusion. One week prior to presentation she experienced peri- and retro-orbital pain accompanied by nausea, vomiting, and exodeviation of the right eye. Four days prior to presentation she visited the emergency department of another hospital, where she was discharged with pain medication after normal MRI and magnetic resonance angiogram (MRA). When her symptoms worsened, she presented to the authors’ hospital. Apart from the symptoms already described, general and neurological exams were unremarkable. All laboratory investigations, including lumbar puncture, were normal. Computed tomography (CT) of the head and chest X-ray were normal. A repeat non-contrast MRI of the head and orbit with coronal and axial T1 spin-echo and T2 turbo spin-echo sequences, T1 fat-suppressed at the orbit and cavernous sinus level, was unremarkable and revealed normal cavernous sinuses. The patient was nevertheless diagnosed with THS following marked improvement 48 hours after treatment initiation of 4 mg/kg of methylprednisolone (8).
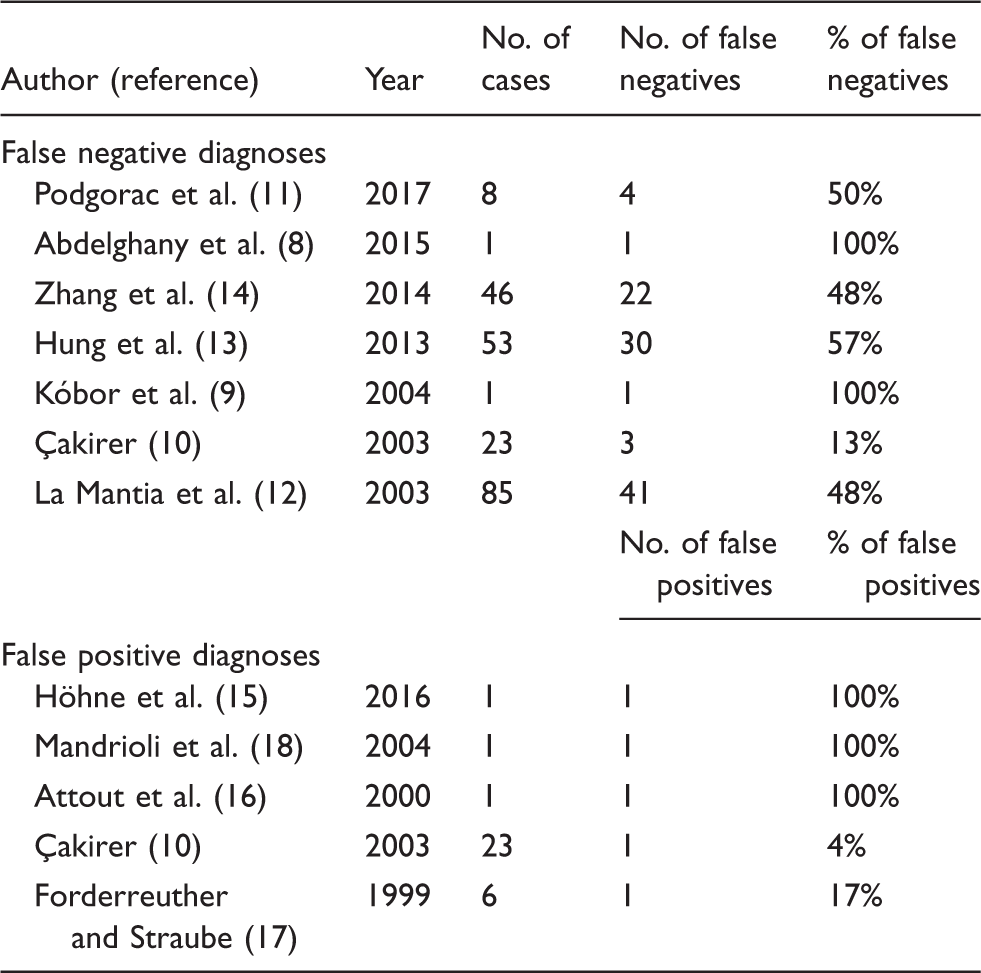
THS with normal MRI has been reported by other authors as well. Kóbor et al. describe a 12-year-old girl whose MRI and MRA were normal 4 weeks after symptom onset (9). In a case series on MRI findings before and after corticosteroid therapy in patients diagnosed with THS, Çakirer notes that 13% of cases had normal MRIs (10). In another case series by Podgorac et al., granulomatous inflammation could not be demonstrated for 50% of patients diagnosed with THS (11). La Mantia et al. completed a review of the literature on THS from 1988 to 2002, and 48% of cases meeting contemporaneous diagnostic criteria for THS had normal neuroimaging findings (12). Although the authors hypothesized that better imaging protocols would have diagnosed more cases of granulomatous inflammation, it cannot be assumed that this is true for all patients with unremarkable MRIs. Furthermore, Hung et al. completed a case series on patients presenting to their hospital with THS between 1990 and 2011; “benign THS” was diagnosed in 57% of patients since MRI findings did not reveal inflammation (13). Finally, the most recent review of the THS literature, completed by Zhang et al. and including cases between 2003 and 2013, found that 48% of patients with confirmed THS had no abnormalities on MRI. The authors concluded that it is “very questionable whether ICHD-3 beta diagnostic criteria should rely on [MRI] (or biopsy) so completely” (14).
False positive diagnoses of Tolosa-Hunt Syndrome
Although less well described in the literature, a number of cases of THS that fulfill ICHD-3 beta criteria but are later attributed to different pathologies have been reported. The most recently published case report on this topic provides a representative example.
Pathologies mimicking THS with granulomatous inflammation on MRI
Höhne et al. describe a 63-year-old man who presented with unilateral left-sided orbital pain and diplopia. Lumbar puncture was positive for oligoclonal bands, though other laboratory investigations were normal. MRI revealed granulomatous inflammation of the cavernous sinus and the patient’s symptoms resolved immediately following treatment with 100 mg/day of prednisolone. The patient was diagnosed with THS. Orbital pain nevertheless recurred when corticosteroid treatment was reduced, and symptoms slowly returned. When they became intolerable several years later, a subsequent MRI showed a contrast-enhancing mass in the cavernous sinus and after extensive workup the patient was definitively diagnosed with cryopyrin-associated periodic fever syndrome (15).
Comparable reports have been published by other authors. Attout et al. describe the case of a 78-year-old patient presenting with symptoms consistent with THS and MRI showing granulomatous inflammation. Although THS was initially suspected, further workup revealed the presence of systemic non-Hodgkin’s lymphoma (16). Förderreuther and Straube report the case of a 57-year-old patient with THS-like symptoms and an abnormal MRI who responded to corticosteroid therapy. A definitive diagnosis of CNS vasculitis was made several months later, on the basis of subsequent imaging and CSF findings (17). In his series of 23 cases, Çakirer describes one patient diagnosed initially with THS following the classical constellation of symptoms and a MRI showing a mass indistinguishable from cavernous sinus tissue. Corticosteroid therapy resolved the orbital pain, but the patient was reevaluated two weeks later when neurological symptoms persisted, and was demonstrated to have a paracavernous sinus meningioma. As Çakirer points out, neurinomas, lymphomas, sarcoidosis, meningiomas and pituitary macroadenomas all “may have signal intensities similar to the soft tissue lesions of THS” (10). Kobor et al. concur, noting that in addition to mimicking the non-specific granulomatous inflammation of THS, some neoplasms can also improve on steroid therapy (9).
Finally, Mandrioli et al. present a case illustrating the most acutely dangerous setting of a false positive THS diagnosis. A 43-year-old man was admitted following one week of acute-onset left-sided retro-orbital pain and subsequent sixth nerve palsy. Although MRI findings were benign, THS was diagnosed based on recovery from ophthalmoplegia following corticosteroid treatment. MRI at four-month follow-up, however, revealed a lesion enlarging the left cavernous sinus, and by sixth-month follow-up the pain and sixth nerve palsy had returned. A biopsy showed actinomycetes colonies, and the patient subsequently responded favorably to antibiotic treatment (18). As demonstrated by this case, misdiagnosis of THS in the setting of infection risks serious consequences as corticosteroid treatment, which may initially palliate symptoms, can exacerbate the underlying infectious etiology.
A two-part rationale for revising the diagnostic criteria for Tolosa-Hunt Syndrome
The evolution of the diagnostic criteria for THS has proceeded slowly over the course of several decades. With each subsequent revision, ICHD guidelines have accorded more importance to the role of neuroimaging. In its most recent iteration, the ICHD-3 beta requires the presence of granulomatous inflammation of the cavernous sinus, superior orbital fissure, or orbit, as demonstrated by magnetic resonance imaging (MRI) or biopsy for diagnosis of THS (4). As demonstrated by the cases described above, we believe that this reliance on neuroimaging for THS diagnosis may be problematic.
First, the literature suggests that THS can present with an unremarkable MRI. As MRI technology and protocols improve, it is likely that some of these MRI diagnoses could be properly reclassified. Nevertheless, given the range of radiological skill levels in medical settings worldwide and the probability that not all THS cases present with granulomatous inflammation visible to even the most skilled radiologist, the number of false negative diagnoses might rise under ICHD-3 beta criteria. We agree that neuroimaging should be mandatory for suspected THS, especially for its critical use in identifying other pathologies causing symptoms that are consistent with THS, but we question whether the presence of MRI-confirmed granulomatous inflammation should itself be mandatory for a diagnosis of THS.
It should be noted that ICHD-3 beta criteria allow for the demonstration of granulomatous inflammation by MRI or by tissue biopsy. It is likely that THS is accompanied by granulomatous inflammation even when not visible on MRI. Nevertheless, biopsy of the cavernous sinus is a sophisticated and difficult procedure that must be performed by an experienced neurosurgeon. The constellation of THS symptoms often does not warrant the risks of biopsy, limiting its utility for diagnosis.
Second, evidence suggests that MRI-confirmed granulomatous inflammation can accompany THS-like symptoms in patients presenting with other pathologies, usually of neoplastic or infectious origin. These pathologies can also respond favorably to corticosteroid therapy, leading to misdiagnosis. The presence of granulomatous inflammation in addition to THS symptomatology can give clinicians a false sense of security in their diagnoses and prevent investigation for more dangerous etiologies. As painful ophthalmoplegia can arise secondary to myriad pathologies, diagnostic workups for all possibilities should be exhausted before arriving at a diagnosis of THS. In particular, lesions eroding bone or invading adjacent brain parenchyma should be red flags for non-THS etiologies. Regardless of MRI findings, workups for tuberculosis and fungal infections should also be completed.
Papers reporting Tolosa-Hunt Syndrome misdiagnoses.
Finally, we appreciate that ICHD-3 beta criteria would helpfully exclude false positive THS diagnoses in cases presenting with a normal MRI. A number of these cases have been described in the literature (19,20). Nevertheless, on balance, we believe that this merely trades one cohort of false positives for another. Given the previously described sense of security following MRI-confirmed granulomatous inflammation with THS symptoms, we prefer false positive diagnoses to consist of MRI-negative patients rather than MRI-positive patients, since MRI-negativity encourages further workup and MRI-positivity confers a sense of a definitive diagnosis.
Conclusion
Proposed revisions to the ICHD-3 beta diagnostic criteria for Tolosa-Hunt syndrome.

Clinical implications
The literature shows that MRI technology may not be able to identify Tolosa-Hunt Syndrome (THS) reliably, and biopsy is not always indicated for THS symptomatology. Cases have also been reported of MRI-confirmed THS that are later attributed to other pathologies. Requiring the demonstration of granulomatous inflammation for a diagnosis of THS may therefore introduce the potential for false negative and false positive diagnoses. We propose making the demonstration of granulomatous inflammation on MRI or biopsy non-mandatory for THS diagnosis, and lengthening patient follow-up to two years in cases with benign MRI findings.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.