
Abstract
A bibliographical search was conducted for papers published between 1999 and 2007 to verify the validity of International Classification of Headache Disorders (ICHD)-II criteria for the Tolosa-Hunt syndrome (THS) in terms of (i) the role of magnetic resonance imaging (MRI); (ii) which steroid treatment should be considered as adequate; and (iii) the response to treatment. Of 536 articles, 48, reporting on 62 patients, met the inclusion criteria. MRI was positive in 92.1% of the cases and it normalized after clinical resolution. There was no evidence of which steroid schedule should be considered as adequate; high-dose steroids are likely to be more effective both to induce resolution and to avoid recurrences. Pain subsided within the time limit required by the ICHD-II criteria, but signs did not. We conclude that THS diagnostic criteria can be improved on the basis of currently available data. MRI should play a pivotal role both to diagnose and to follow-up THS.
Introduction
Tolosa–Hunt syndrome (THS) (1, 2) is a rare disorder characterized by periorbital or hemicranial pain accompanied by diplopia, that may eventually recur. The aetiology is still unknown, but the underlying pathophysiological mechanism has been proven to consist of a granulomatous inflammatory process. THS was identified as a nosological entity by the International Headache Society classification criteria published in 1988 (3). These criteria were substantially revised in the 2004 classification (4) (Table 1), and the literature was critically reviewed accordingly (5).
ICHD-II classification part three. Cranial neuralgias, central and primary facial pain and other headaches

In our opinion, there are several pending questions regarding the appropriateness of the diagnostic criteria according to the present International Classification of Headache Disorders (ICHD)-II, especially in terms of the best treatment choice, the duration of symptoms and signs and the anatomical distribution of lesions.
The classification criteria mention magnetic resonance imaging (MRI) explicitly for the diagnosis and implicitly for the differential diagnosis of THS (6, 7), but we think that a positive MRI performed with appropriate techniques (8–12) should be mandatory for diagnosis.
The ICHD-II states in point D that ‘adequate steroid dosage should resolve disease symptoms and signs within 72 h from the treatment onset’. The adequate dosage of steroids and the best route of administration are undefined. The consistency of the 72-h period, as a time limit for resolution of symptoms and signs, does not seem to be sustained by appropriate evidence in the literature and, in our opinion, does not fit the real disease course. Indeed, it seem to represent a critical misleading point in the diagnostic process. Another question pertains to the anatomical distribution of lesions for the diagnosis of THS. According to the ICHD-II criteria, all inflammatory granulomas located in the cavernous sinus, the orbital apex and the orbit, independently of the involved structures (nerves, muscles or both), can justify the diagnosis of THS. In contrast, most of the neurological and neuroradiological textbooks reserve this diagnosis for those lesions located in the cavernous sinus, while they define the inflammatory processes involving the orbit as ‘pseudotumour’. This discrepancy of terms and definitions limits the appropriateness of the diagnosis, prognosis and the best treatment choices.
Objectives
We set out to compare clinical features and outcome measures in discrete subgroups of THS patients according to:
the distribution of lesions (cavernous sinus, orbital apex, orbit, extraocular muscles);
different steroid dosage and route of administration.
Fruitfulness
We also set out
to verify the external consistency and appropriateness of the ICHD-II criteria for THS, paying particular attention to:
the time duration of symptoms and signs according to the steroid treatment
the inclusion of different anatomical locations of lesions conditioning involvement of different structures (nerves, muscle or both) in the same paragraphs of the ICHD-II;
to provide useful propositions about the best pharmacological treatment and the most appropriate criteria for MRI follow-up.
For these reasons, we reviewed the reports on patients suffering from THS who underwent MRI examination, but we also considered some conditions that mimic, but cannot be classified as THS due to the localization of the inflammatory process.
Methods
We conducted a bibliographical search on PubMed/Metacrawler and on Embase using the following Keywords: ‘Tolosa Hunt’, ‘Orbital pseudotumor’, ‘Idiopathic orbital inflammation’, ‘Painful ophthalmoplegia’. The limits of the search were the English language, and the date of publication between 1 January 1999 and 31 January 2007.
To be considered further, the cases had to:
have been studied by means of MRI;
fulfil the ICHD-II diagnostic criteria of THS with the exception of point D, concerning symptom resolution within 72 h after starting steroid treatment;
be as in point 2, but with an extension of the inflammatory process outside the orbit and the cavernous sinus;
be as in point 2, but with inflammation located in the ocular muscles only.
For each case we noted the following data: sex, age, side, symptoms (orbital pain, diplopia, visual loss, facial numbness or pain), signs (ocular motor palsy, ocular motor palsy and visual loss, ocular motor palsy and abnormal facial sensation, ocular motor palsy and facial palsy), associated diseases, MRI techniques, location of inflammatory tissue as detected by MRI (coded as not detectable, cavernous sinus only, orbit with or without cavernous sinus, cavernous sinus and/or orbit with extension to other intracranial structures, and extraocular muscles), time elapsed between onset of symptoms and starting treatment, duration of clinical follow-up, duration of MRI follow-up.
We also considered the treatment schedules and distinguished three groups: the ‘regular’ steroid dosage group including patients who were treated with an initial dosage of about 1 mg/kg per day, and the ‘high’ steroid dosage group including patients who were treated with an initial dosage of 500–1000 mg/day for a few days and then usually switched to a ‘regular’ regimen for a longer period, and treatments ‘other’ than steroids.
Finally, for each subject we noted the following outcome features: pain resolution (coded as more or less than 72 h, and coded as number of days), symptoms resolution (coded as more or less than 72 h, and coded as number of days), time of pathological tissue disappearance on MRI (coded as yes or no, and coded as number of days), occurrence of recurrence (coded as yes or no).
On the basis of the location of inflammatory tissue as detected by MRI, the subjects were divided into three diagnostic groups:
the THS group (no inflammatory tissue detectable, cavernous sinus only, orbital apex and/or orbit with or without cavernous sinus);
the THS plus group (cavernous sinus and/or orbit with extension to other intracranial structures);
the orbital myositis (OM) group (extraocular muscles).
In the THS group we distinguished a further three subgroups on the basis of the lesion site:
normal MRI subgroup;
cavernous sinus subgroup (cavernous sinus only);
orbital apex and/or orbit and cavernous sinus subgroup (orbit with or without cavernous sinus).
For each of the three diagnostic groups, the mean and standard deviation (SD) values of each of the above-mentioned variables were computed. We then compared the mean values between groups by means of a Kruskal–Wallis or Mann–Whitney test for the continuous variables, and by means of a χ2 test for the ordinal variables.
In the THS group for each of the outcome variables (pain resolution, symptom resolution, time of pathological tissue disappearance at MRI, occurrence of recurrence), we compared the mean values between the cavernous sinus subgroup and the orbit and cavernous sinus subgroup.
Finally, considering all the subjects together, the possible relationship between the kind of steroid treatment (regular and high-dose) and the outcome variables (sign disappearance, MRI normalization, and recurrence) was evaluated by means of χ2 and Mann–Whitney tests.
The critical P-value was set at P = 0.01.
Results
The bibliographical search revealed 536 articles, 48 of which met the criteria to be included (8–11, 13–56). Overall we included 62 subjects extracted from 48 reports: 38 in the THS group (three of which showed a normal MRI and three were not treated), 16 in the THS plus group and eight in the OM group.
In the THS group, inflammation was detectable only in the cavernous sinus in 23 (60.5%) patients, in the cavernous sinus and/or in the orbit in 12 (31.6%) patients and was not detectable in three (7.9%) patients only.
The features of the individual reports described in each of the papers included in this Review are available as supplementary on-line material, and Tables 2 and 3 summarize the data.
For each variable the table shows the mean and the standard deviation (SD) values, and the range for each diagnostic group, and the results of the Kruskal–Wallis test (K–W) for mean comparison
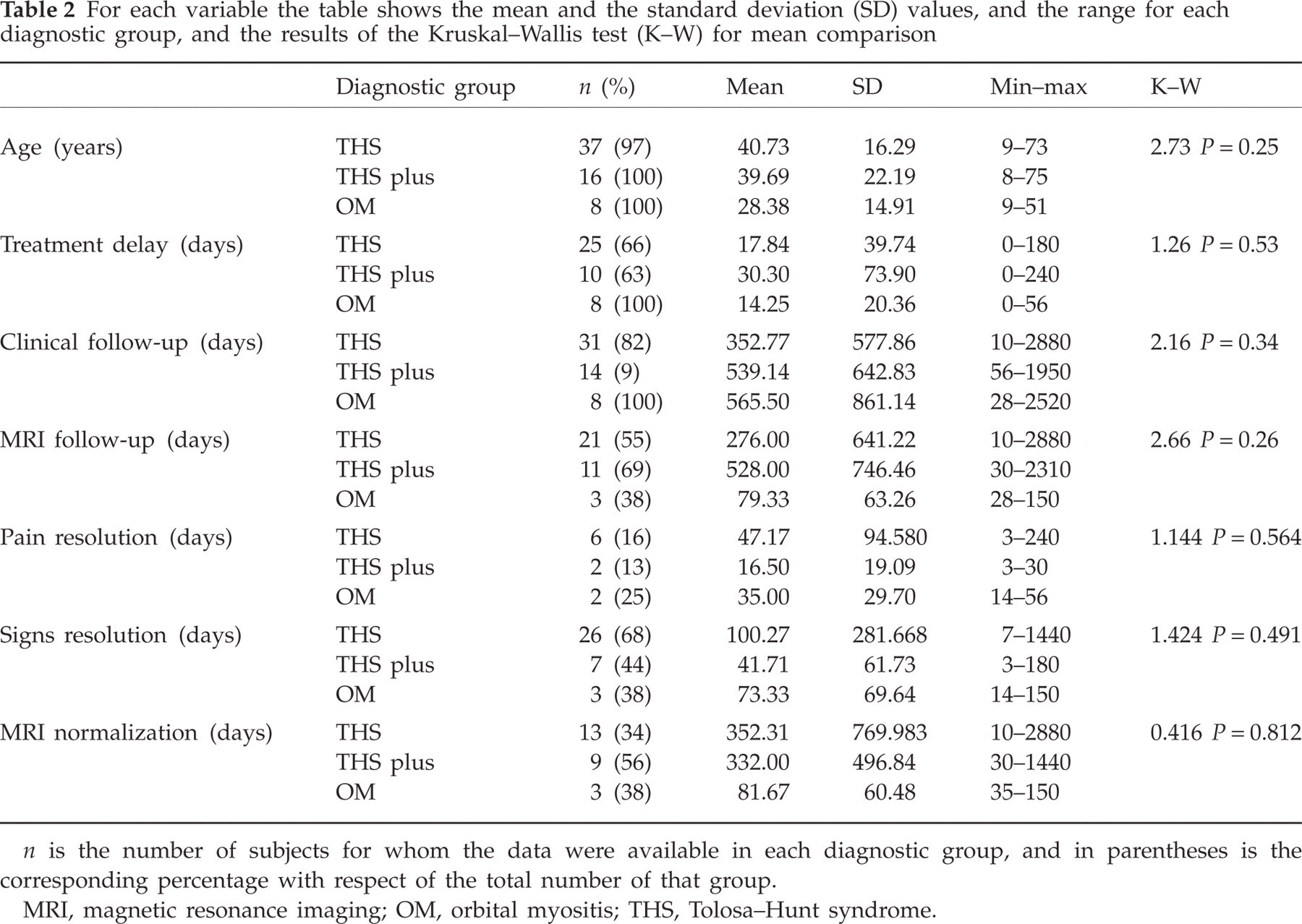
n is the number of subjects for whom the data were available in each diagnostic group, and in parentheses is the corresponding percentage with respect of the total number of that group.
MRI, magnetic resonance imaging; OM, orbital myositis; THS, Tolosa–Hunt syndrome.
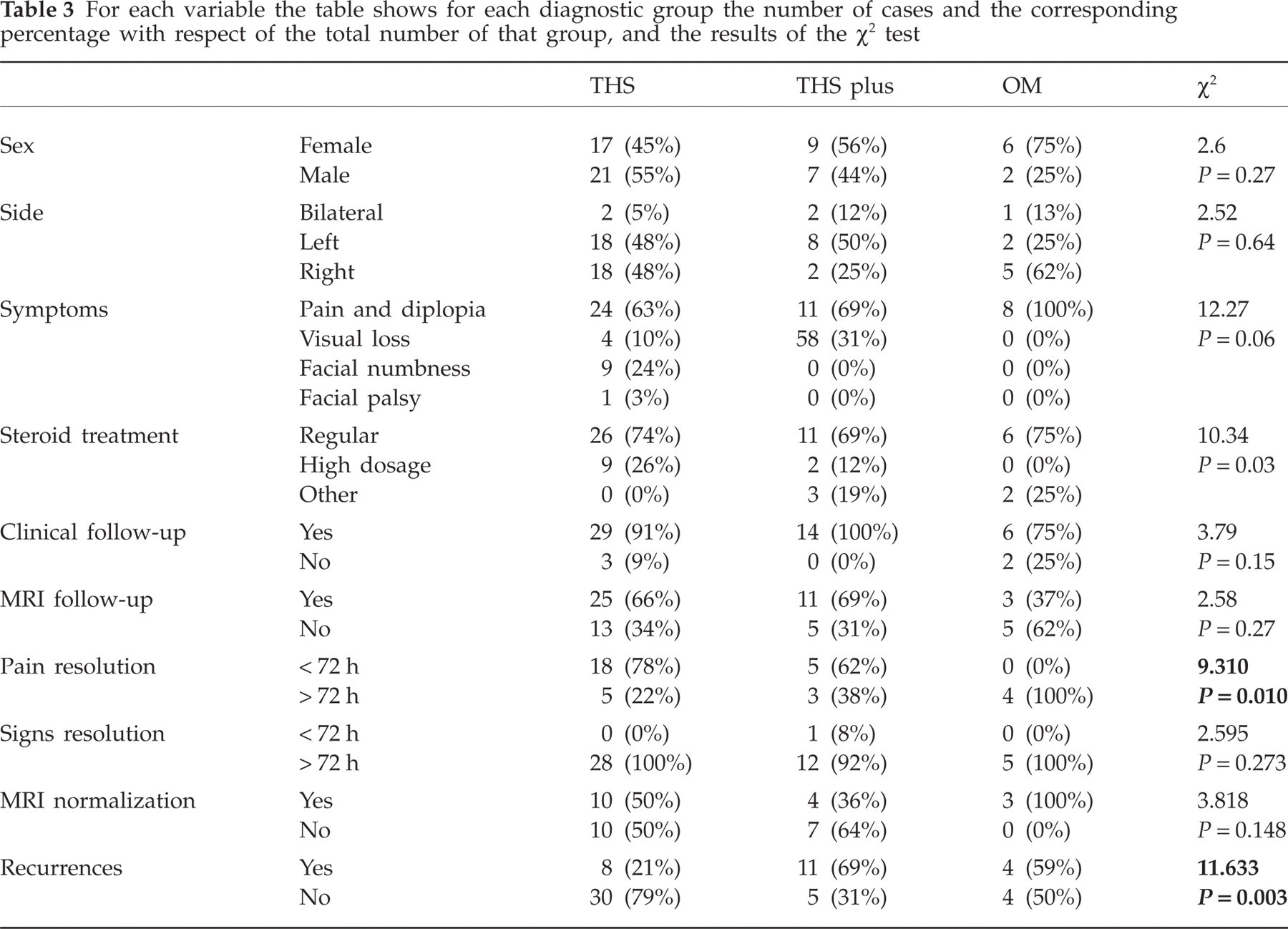
For each variable the table shows for each diagnostic group the number of cases and the corresponding percentage with respect of the total number of that group, and the results of the χ2 test
In all the patients for whom these data were available (30/62, 48.4%), the interval between pain and ocular motor palsy onset was always < 2 weeks, as required by the classification criteria.
The three diagnostic groups did not differ in most of the variables (Tables 2 and 3), and the variability of the data may partly account for this negative finding. The only exceptions were pain resolution within the 72-h time limit, and recurrence. Pain resolution within the 72-h time limit occurred more frequently in the THS and THS plus than in the OM group (Table 3), and recurrence was more likely in the THS plus and in the OM than in the THS group (Table 3).
Although the pain resolved within 72 h after starting treatment, as required by the classification criteria, in most of the THS and THS plus patients, the signs resolved only in one THS plus patient within this time limit (Table 3). The mean time needed for sign disappearance was not statistically significantly different in the three diagnostic groups (Table 2).
The mean duration of MRI follow-up was not statistically significantly longer (Mann–Whitney U 110, z =−0.08, P = 0.933) in patients who showed normalization (n = 16; 230 days) than in those who did not (n = 14; 448 days), but the normalization of MRI always lasted longer than sign resolution in all three diagnostic groups (Table 2).
When the outcome variables were compared in the two THS subgroups (the cavernous sinus subgroup and the orbit and cavernous sinus subgroup), no significant difference was found.
Fifty-four (87%) patients underwent steroid treatment, five (8%) underwent treatment other than steroids (including surgical removal of the inflammatory tissue) and three (5%) were not treated. Treatments most often lasted about 2 months, but the duration could range from a few days to several years.
By considering all the patients together, the mean time needed for sign disappearance was longer after regular (n = 27; 104 days) than after high-dose steroid treatment (n = 8; 35.5 days), but these two figures did not prove to be statistically significant (Mann–Whitney; P = 0.686). The time to reach MRI normalization showed similar behaviour, being longer after regular (n = 20, mean 369.5 days, range 10–2880 days) than after high-dose treatment (n = 3; mean 119.3 days, range 10–320 days), but again this difference was not statistically significant (Mann–Whitney U 17.5, z = 1.14, P = 0.253).
Recurrence occurred in 19 (44.2%) patients who underwent regular steroid treatment and in only one (9.1%) of those treated with high-dose steroid (χ2 = 4.62, Fisher's exact test P = 0.039).
Discussion
We were able to consider 62 patients derived from papers about single or a few cases with some unusual features. However, these features varied from one subject to another, and we consider that as a group these patients are likely to be representative of THS, with the only exception that they do not need to fulfil the 72 h diagnostic criteria.
Some points clearly stand out:
The classification criteria require that both symptoms and signs resolve within 72 h after starting adequate steroid treatment. Unfortunately, the classification criteria do not state what ‘adequate’ means, and the literature reports individualized rather than standardized treatment. In addition, in only 2% of the patients did the signs resolve so quickly.
MRI showed the presence of inflammatory tissue in 92.1% of THS patients: this, and the clinical overlap of THS with other conditions such as those we labelled as THS plus and OM, strongly supports the importance of MRI for the diagnosis of THS.
The localization or extension of the inflammatory tissue does not seem to be a prognostic factor, and, more specifically, the patients from the THS plus group and those from the THS group behave similarly. It may be suggested to amalgamate the two groups. Furthermore, neuroradiological distinction between the THS syndrome (inflammatory tissue within the cavernous sinus) and the ‘pseudotumor orbitae’ needs further investigation to prove its clinical significance.
MRI data show that the disappearance of inflammatory tissue takes longer than symptom resolution, and that pathological tissue may not disappear even after several months. Accordingly, it may be suggested that MRI should be used to monitor the disease course and to support the decision of when treatment should be stopped.
However, the question of whether THS may have a relapsing course or may become a chronic condition, and whether these two outcomes depend on treatment, is left open.
Our review showed that the choice of treatment varied in terms of the kind of steroid, dosage, administration method and duration; but also suggested that recurrence is less likely in patients with high-dose than in those with regular steroid treatment.
Conclusion and proposal
Overall, in our opinion the classification criteria for THS syndrome could benefit from the points discussed above: (i) there is no evidence of what kind of steroid treatment is adequate; (ii) the 72-h time limit should be applied for pain resolution only; (iii) MRI plays a key role in diagnosis; and (iv) inflammatory tissue can extend beyond the cavernous sinus and the orbit. Points (iii) and (iv) imply that we need to use MRI techniques specifically aimed at showing the presence of inflammatory tissue, as suggested by Cakirer (8), La Mantia (5) and ourselves (9). The diagnosis of THS cannot rely only on MRI data, but these should be used in conjunction with clinical findings both to make the diagnosis and to follow-up patients suffering from THS and, in some cases, a biopsy will still be needed to ascertain the nature of the pathological tissue.
The classification criteria could be modified as follows:
One or more episodes of unilateral orbital pain persisting for weeks if untreated
Paresis of one or more of the third, fourth and/or sixth cranial nerves and demonstration of granulomatous material in the cavernous sinus, superior orbital fissure or orbit by MRI
Paresis coincides with the onset of pain or follows it within 2 weeks
Pain resolves within 72 h when treated with corticosteroids
Other causes have been excluded by appropriate investigations.
Notes
NRI should be performed with 3 mm thickness coronal and axial T1-SE and T2-TSE sequences and with T1 fat-suppressed weighted images after godolinium administration at the level of the orbit and cavernous sinus.
Other causes of painful ophthalmoplegia include vascular, neoplastic, infectious, systemic granulomatous diseases, basal meningitis, diabetes mellitus, ophthalmopletic migraine, thyroid ophthalmopathy and trauma.
Comments
Some reported cases of THS had additional involvement of the trigeminal nerve (commonly the first division) or optic, facial or acoustic nerves. Sympathetic innervation of the pupil is occasionally affected.
The syndrome is caused by granulomatous material in the cavernous sinus, superior orbital fissure or orbit in some biopsied cases; granulomatous material can have an intracranial extension, as demonstrated by MRI.
Careful clinical and MRI follow-up is required to confirm the diagnosis and to manage the steroid treatment.
It might also be beneficial to distinguish between definite THS, when all the criteria are met, and possible THS, when all the criteria but the one of point D are met.
These criteria implicitly suggest that THS is an idiopathic disorder whose pathophysiology consists of a granulomatous inflammatory process, and that THS could be moved from the ‘cranial neuralgia’ section to the ‘secondary headache’ section.
In conclusion, further multicentre studies are necessary to improve our knowledge of THS, but the revision of previous papers can suggest some changes to improve the classification criteria.