
Abstract
Objective
The objective of our study is to assess the impact of triptan exposure on pregnancy outcome.
Methods
We performed a prospective observational cohort study with 432 pregnant women exposed to triptans and enrolled by the German Embryotox system. Pregnancy outcomes were compared with a migraine and a non-migraine comparison cohort. Primary objectives were major birth defects and spontaneous abortion; secondary endpoints were preterm delivery, birth weight, pregnancy complications and the rate of electively terminated pregnancies.
Results
Compared to a non-migraine cohort the rates of major birth defects (ORadj 0.84; 95% CI 0.4–1.9), spontaneous abortions (ORadj 1.20; 95% CI 0.9–1.7), preterm delivery (ORadj 1.01; 95% CI 0.7–1.5), and preeclampsia (ORadj 1.33; 95% CI 0.7–2.5) were not increased in triptan-exposed pregnancies.
Conclusions
Our findings support the evidence that triptans are not major teratogens. When compellingly needed during pregnancy, sumatriptan as the best studied triptan appears an acceptable treatment option. A detailed fetal ultrasound should be offered in cases of first trimester exposure to less well-studied triptans.
Trial registration number in German Clinical Trials Register: DRKS00007660
Introduction
Migraine is a common disorder in women of childbearing age, and usually requires pharmacological treatment (1,2). Up to 50% of pregnancies occur unplanned, and the fetus may be inadvertently exposed to antimigraine drugs (3). In particular, the first trimester represents a vulnerable period for drug toxicity (4). As pregnant women are typically excluded from clinical trials, observational data are of utmost importance for studying drug safety in pregnancy. Triptans are an effective treatment for acute migraine disorders (5). However, due to insufficient experience as to their safety during pregnancy, triptans are less frequently used by pregnant women than paracetamol or nonsteroidal anti-inflammatory drugs (2). Studies published so far have not found an association between triptans during pregnancy and birth defects in humans (6–13), while other adverse outcomes like spontaneous abortion (SAB) (14,15), preterm delivery (12,16) and low birth weight (≤2.500 g) (9) have been described sporadically. In particular, newer triptans have rarely been studied during pregnancy as yet. Disease-specific adverse effects of maternal migraine on the fetus and the course of pregnancy are insufficiently studied, and have rarely been considered in studies on triptan safety during pregnancy (8,9). The aim of this study was to assess the impact of triptans on pregnancy outcome, in particular on the risk of major birth defects and SAB.
Methods
Study design
This prospective observational cohort study includes pregnant women with migraine disorder and triptan medication (exposed cohort) in comparison with pregnant women without migraine disorder (non-migraine comparison cohort) and pregnant women with migraine disorder not taking triptans (migraine comparison cohort). All data were enrolled by the German Embryotox system, which is a well-established, publicly-funded institution accessed by pregnant women, obstetricians and other health care professionals in Germany. Through individual risk counseling, annually more than 4,000 critically exposed pregnancies are documented as to their outcome. The identification of cases takes place before the outcome of pregnancy or pathological results of prenatal diagnostics are known. In addition, the Embryotox system serves as a national clearing house for suspected adverse drug reactions in pregnancy and receives case reports for evaluation from health care professionals, patients, pharmaceutical industry and the Drug commission of the German Medical Association. Subjects in this study were enrolled between January 1999 and December 2014.
The study was approved by the Ethics Committee of the Charité Universitätsmedizin Berlin (EA4/002/15) and registered at the German Clinical Trials Register (DRKS00007660).
Data enrolment
All data are recorded using structured questionnaires via phone interview and/or as a written form. At initial contact, the patient’s consent for follow-up on pregnancy outcome eight weeks after the estimated date of birth is asked for. The primary questionnaire includes items such as maternal characteristics, medical and obstetric history, chronic diseases, smoking, alcohol, street drugs and family history, maternal profession, and educational achievement categorised as either low (nine-year exam or less), medium (10- or 13-year exam) or high (academic study). The follow-up covers additional medication, pregnancy complications, course of delivery, gestational age at birth and characteristics of the newborn such as sex, birth weight, length, head circumference, Apgar score, umbilical artery pH, birth defects, postnatal disorders and, if applicable, pregnancy loss and its circumstances. In cases of birth defects or other relevant complications, medical reports are requested.
Study cohorts
The inclusion criterion for the exposed cohort was triptan use for migraine disorder any time from conception to delivery. Therapy may have started earlier and could have lasted longer. The non-migraine comparison cohort included pregnant women who were neither exposed to triptans nor to one of the following established teratogens or fetotoxicants: Acenocoumarol, carbamazepine, lenalidomide, methotrexate, mycophenolate, phenobarbital, phenytoin, retinoids (acitretin, adapalen, isotretinoin, tazaroten, tretinoin), thalidomide, topiramate, valproic acid, warfarin, angiotensin-converting enzyme inhibitors and angiotensin II receptor antagonists. In addition, patients with acute malignancies were excluded. Comparison subjects were matched by year of ascertainment at a ratio of 4:1 (non-migraine comparison cohort: exposed cohort). The migraine comparison cohort included pregnant women suffering from migraine disorder but not taking triptans between their last menstrual period and delivery. In addition to the prospective cohorts, the retrospective Embryotox database was screened for case reports suggesting adverse drug reactions. These data are presented separately.
Outcome variables
The primary objective of this study was to estimate the risk of major birth defects and SAB. Secondary endpoints were preterm delivery, birth weight, pregnancy complications (preeclampsia, abruptio placentae) and the rate of electively terminated pregnancies (ETOP). Two independent experts categorized the observed birth defects into major and minor according to EUROCAT (17). In cases of disagreement, a third expert was consulted. All experts were blinded to the exposure status. Pregnancy loss with fetal weight <500 g was classified as SAB and ≥500 g as stillbirth. In cases of unknown birth weight, gestational age was used to differentiate between SAB (<23 weeks of gestation) and stillbirth (≥23 weeks of gestation). Gestational age was calculated using ultrasound-based measures during the first trimester or, if not available, the date of the last menstrual period.
Statistical analysis
The rates of birth defects were defined as the number of malformed children and fetuses divided by the number of all live births plus the number of pregnancy losses with birth defects. Birth defects caused by genetic or chromosomal anomalies were counted separately. Adjustment was based on propensity score stratification for sufficient bias reduction (18). The propensity score (PS) was estimated using boosted regression trees on the basis of the following covariates: Maternal age, body mass index, smoking habits, alcohol consumption, number of previous abortions and previous parities, as well as number of previous children with birth defects (19). Pregnant women were classified into five strata defined by the quintiles of the propensity score. To screen for critical exposure periods, pregnant women were stratified into four exposure intervals: Gestational week 0 to 6 + 6; 7 + 0 to 12 + 6; 0 to 12 + 6; >13 weeks. Hazard ratios (HR) were provided by using Cox proportional hazards models to estimate the effect of triptan exposure on the risk of SAB and ETOP. Time of exposure was taken into account. Live birth, SAB, stillbirth and ETOP were regarded as competing events. Because patients were identified at different gestational times, delayed study enrolment was taken into account (20). Adjustment of the analyses was performed by using the same covariates as mentioned above. Cumulative incidences of SAB and ETOP were not calculated because of disparity in time of exposure to triptans in the exposed group. The effect of triptan exposure on the risk of preeclampsia was assessed using logistic regression. The analysis was adjusted by propensity score stratification including the covariates mentioned above. In all models including covariate parameters, missing data were estimated by utilising multiple imputation by a chained equation, assuming the values were missing at random (21). Twenty imputed datasets were generated per outcome, including the respective outcomes and the covariates used for adjustment. Analyses of all imputed datasets were carried out as mentioned above, and results were combined subsequently using Rubin’s rule (22). All analyses were carried out with R version 2.15 (R Development Core Team).
Results
Four hundred and thirty-two pregnant women fulfilled the inclusion criteria for the exposed cohort (Figure 1). The migraine comparison cohort consisted of 475 pregnant women who suffered from migraine disorder without taking any triptans during pregnancy. The non-migraine comparison cohort of 1,733 pregnant women (ratio 4:1) was randomly drawn from 30,838 patients meeting the inclusion criteria. The majority of exposed women took triptans in the first trimester (75.2%) and used it orally (93.8%). Half of the patients (50.3%) took triptans on 1–5 days during pregnancy. Only 2.3% had a total exposure of >50 days. Sumatriptan was the most frequently used triptan (Table 1).
Cases exposed to triptans. Selection of the exposed cohort from the German Embryotox pharmacovigilance database. All archived data sets between 1999 2014 were checked for their suitability to the inclusion criteria. Number of patients by trimester of exposure and triptan substance. Subjects exposed to more than 1 triptan or during first and second/third trimester are counted several times. aNumber of patients exposed to >1 triptan

Maternal characteristics.

BMI, body mass index
SAB, spontaneous abortion
ETOP, elective termination of pregnancy
Anti-migraine medication in the migraine comparison cohort.

Exposure to more than one substance is possible
Naproxen (3), mefenamic acid (2), dexketoprofen (1), celecoxib (1), indometacin (1)
Propyphenazone (11), aminophenazone (2)
Tramadol (6), piritramide (2), buprenorphine (1)
Mecloxamine (4), camylofin (2), local anesthetics (2) [lidocaine (1), mepivacaine (1)], antihistamins (2) [buclizine (1), promethazine (1)], iprazochrome (1), pentoxifylline (1), xylomethazoline (1), tetrazepam (1), botulinum toxin (1)
Metoprolol (32), propranolol (9), bisoprolol (2), atenolol (1)
Lamotrigine (1), valproic acid (1), carbamazepine (1)
Amitriptyline (10), trimipramine (1), imipramine (1), doxepine (1), opipramol (1)
Venlafaxine (3), fluoxetine (1)
Flunarizine (4), nimodipine (1)
Vitamin B (3), vitamin D (1), vitamin A (1), vitamin C (1), unknown (2)
Alcohol (2), L-tryptophan (1)
Pregnancy outcomes and birth defects
Rates of pregnancy outcomes including birth defects.

Adjusted odds ratios (OR)/hazard ratios (HR) of pregnancy outcomes including birth defects.
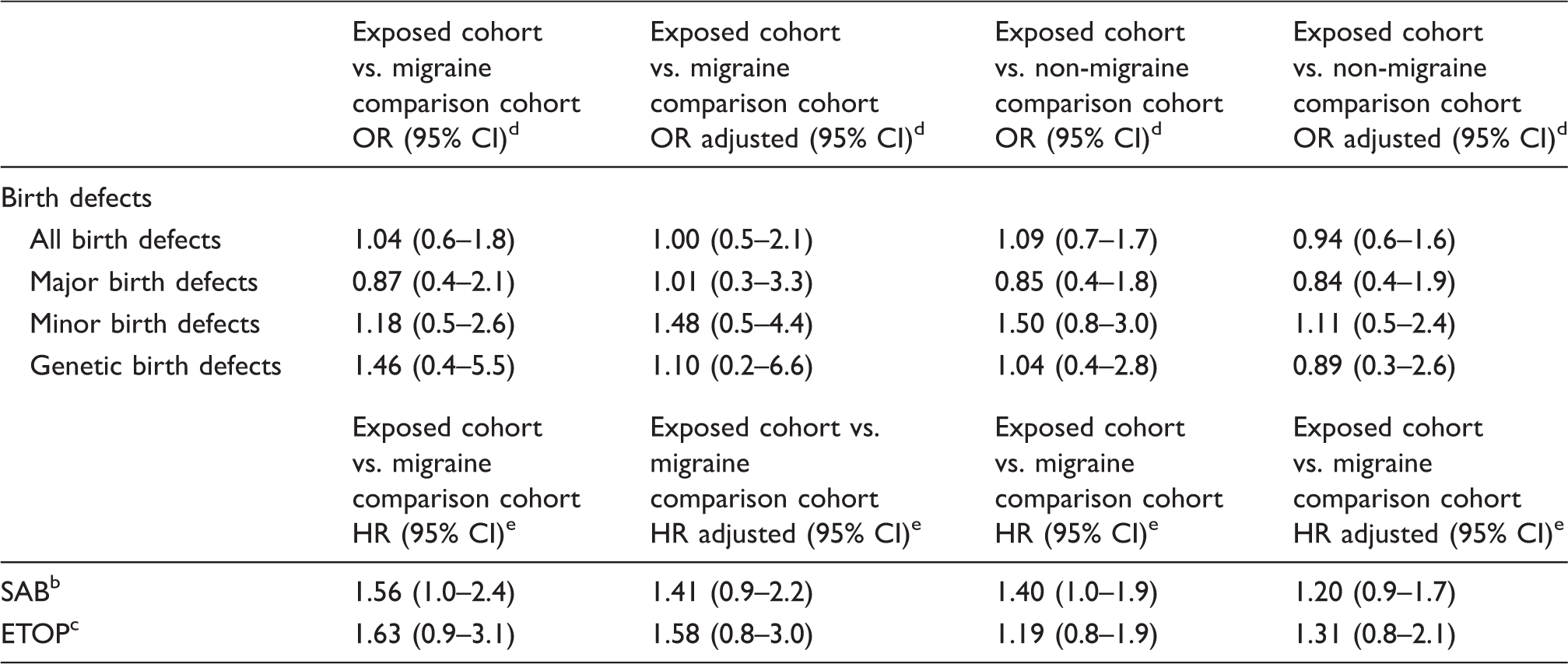
There are various denominators because of various numbers of spontaneous abortions and elective terminations of pregnancies with major, minor or genetic birth defects which were respected in both numerators and denominators (see methods)
SAB, spontaneous abortion
ETOP, elective termination of pregnancy
OR, odds ratio
HR, hazard ratio
Details of major birth defects in the exposed cohort.

SAB, spontaneous abortion
ETOP, elective termination of pregnancy
VSD, ventricular septal defect
PFO, patent foramen ovale
ASD, atrial septal defect
According to EUROCAT definition, microcephaly was only classified as major birth defect when neonatal head circumference was at least three standard deviations below the mean adjusted for sex and gestational age at birth17
Distribution and rates of major congenital malformations by organ systems in the three cohorts.

There are various denominators because of various numbers of spontaneous abortions and elective terminations of pregnancies with major congenital malformations which were respected in both numerators and denominators (see methods)
Rates of birth defects and odds ratios (OR) relating to exposure time of triptans.

30 live-births could not be included due to missing details on maternal triptan expsoure period during the first trimester
One child with a genetic anomaly resulting in an ETOP could not be classified into subgroups due to missing details on maternal triptan exposure period during the first trimester
OR, odds ratio
There are various denominators because of various numbers of spontaneous abortions and elective terminations of pregnancies with major, minor or genetic congenital malformations which were respected in both numerators and denominators (see methods)
Pregnancy complications and neonatal characteristics
Neonatal characteristics.
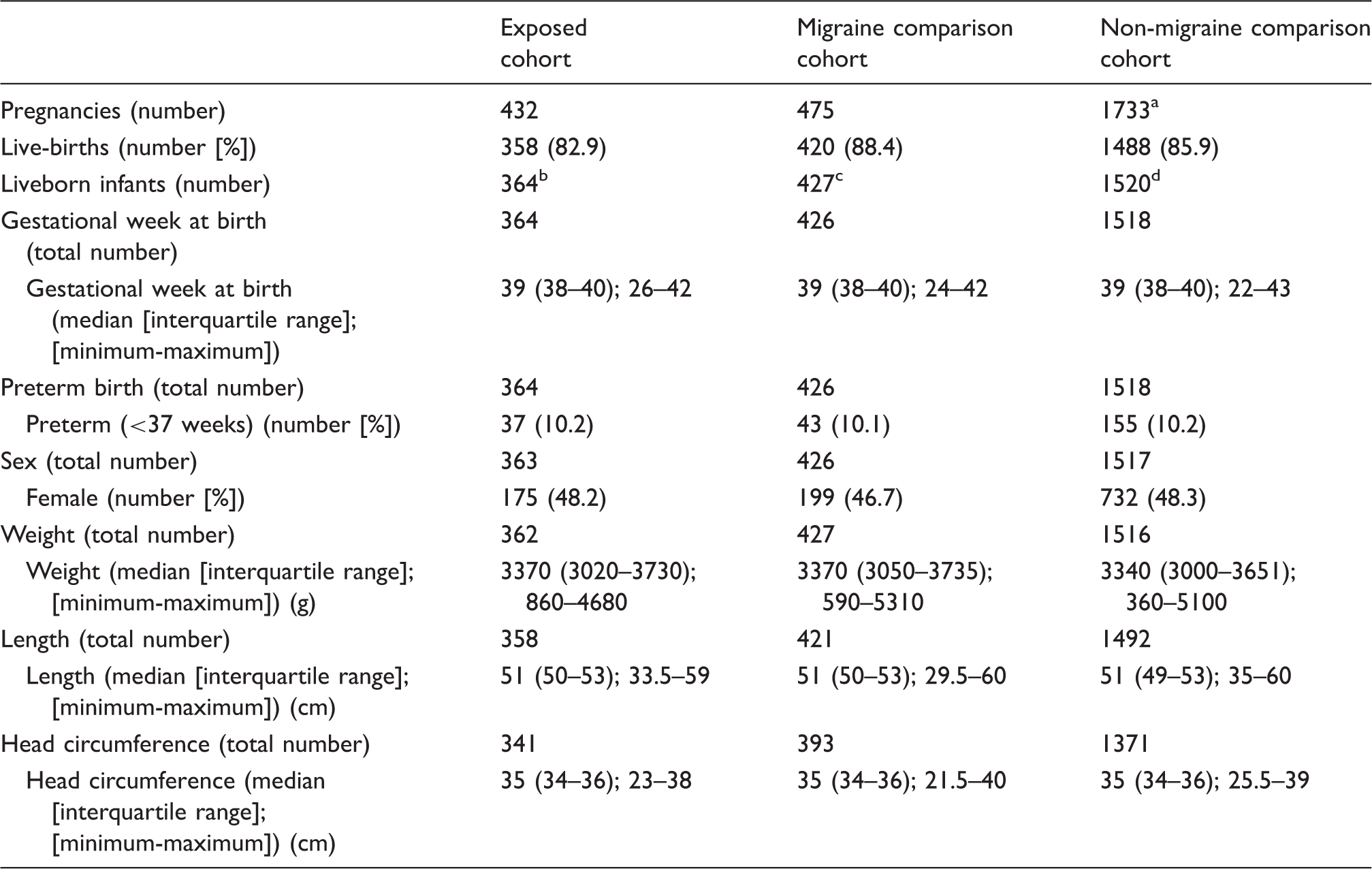
Including one twin pregnancy resulting in one spontaneous abortion and one liveborn infant and one triplet pregnancy resulting in two spontaneous abortions and one liveborn infant
Including six sets of twins
Including seven sets of twins
Including 31 sets of liveborn twins, 1 liveborn infant out of a set of twins and 1 liveborn infant out of a set of triplets
Retrospectively reported cases
Among 16 retrospective case reports on triptan exposure during pregnancy received between 1999 and 2014, there were three SABs and one preterm delivery. The remaining pregnancies ended in term live-births and no birth defects or other adverse pregnancy outcomes were reported.
Discussion
This study analysed 432 pregnant women exposed to triptans during pregnancy in comparison to a migraine comparison and a non-migraine comparison cohort. We did not detect an association between triptan exposure during pregnancy and birth defects. Two of the nine exposed infants with major birth defects had been co-exposed to known teratogens (#5 carbamazepine, #9 isotretinoin, Table 5). Isotretinoin has been shown to cause cleft lip and palate (23,24), which was observed in infant #9. Our findings are in accordance with previous studies (6,8,9,11–13,16) and pregnancy registries (7,10,25). Given a baseline risk of 3% for major birth defects, the power of our study allows detection of a 2.0-fold risk increase. It is noteworthy that three of the nine major birth defects in our exposed cohort were limb defects. This prevalence of 0.8% is higher than in the comparison cohorts (0.5% and 0.3%) and the EUROCAT population based prevalence for limb defects of 0.4% (26). However, due to the small number of only three affected infants in our study, this may be a chance finding. Furthermore, there is no specific pattern of defects (congenital club foot plus finger hypoplasia, syndactyly and polydactyly; #4, #5, #7, Table 5). Banhidy et al. (27) described an association between severe migraine disorder during pregnancy and congenital limb defects. In our study, only two children (0.5%) in the migraine comparison cohort had limb defects (both club foot). In contrast to the results of a former study (9), the overall rate of major birth defects in the migraine comparison cohort was not increased. All in all, these findings neither support a significant teratogenic effect of triptans nor of migraine itself. Eletriptan and frovatriptan showed the highest rates of major birth defects (5.6% and 5.3%, respectively). However, the total number of exposed subjects as well as the number of observed birth defects are too low to draw a definite conclusion and further studies are required to assess the potential risk of these triptans.
The reassuring results of our prospective study are supported by the lack of birth defects among the cases reported retrospectively to our institute by health care providers, health authorities, and pregnant women from all over Germany. This retrospective adverse drug reaction database allows a search for signals of teratogenicity including late onset events. The absence of reports despite many years or even decades of marketing speaks against a major risk of the given drug. It is noteworthy that although valproic acid is the strongest teratogen among antiepileptic drugs it was taken as migraine prophylaxis by five women in the exposed cohort and two in the migraine comparison cohort. Germany and other European countries have strengthened the warnings and restrictions of the use of valproic acid, considering its evidenced teratogenicity. Even for epilepsy it should not be considered as first choice in women of childbearing age and girls (EMA 2017) (28). Some studies discussed serotonergic properties of triptans to be potentially associated with SAB (4,29,30). A statistically significant risk increase for SAB was found by Shechtman et al. (14) and Bérard et al. (15), but in contrast to our investigation, neither study included a migraine comparison cohort to disentangle possible effects of the underlying disease. In addition, potential confounders such as maternal obesity and smoking were not extensively considered in the study of Bérard et al. (15). Other authors could not observe an association between triptan intake during pregnancy and an increased risk of SAB (8,9,12,13). After adjustment, our results suggest a slight trend towards increased SAB rate. The non-significant increase in ETOPs in our exposed cohort was not based on prenatal diagnosis of fetopathology, but may be explained by fear of drug toxicity. Pregnant women exposed to triptans during pregnancy showed a higher rate of placental abruption than the comparison cohorts. However, statistical significance was not reached, which could be due to the low number of affected women, of whom only one took triptans during the third trimester, close to the date of the abruption. Our findings do not confirm an increased risk of preterm delivery nor reduced birth weight, similar to the results of other studies (31,32). Other authors observed more preterm deliveries and a reduced birth weight in association with triptan intake (9,12,16) and in pregnant migraine patients without triptan exposure (9,16). However, these investigations were based on prescription data, which may not reflect the true circumstances of exposure. The increased rate of low birth weight described by Nezvalová-Henriksen et al. was only observed in women taking triptans during the second trimester (9). Further studies reporting on preterm delivery either had no migraine comparison cohort to control for effects of the underlying disorder (12) or were based on a small exposed cohort consisting of only 34 women (16). Although an association between vascular complications, especially preeclampsia, and migraine disorder was discussed by other working groups (31,33,34), our results do not support such an association.
The strengths and limitations of prospective observational pregnancy outcome studies have been discussed elsewhere in detail (35). One limitation of this study is that several women could not precisely recall the gestational days of exposure. The power of sub-analysis for the individual triptans was limited due to low sample sizes. Our cohorts may not be representative of the pregnant population in Germany. Women with higher educational achievement are overrepresented (36). However, the regional distribution of study subjects is approximately the same as the female population of childbearing age in Germany (data not shown). Furthermore, several parameters of the Embryotox comparison cohort such as rate of fetal loss and birth weight are similar to the German population statistics (37). The greatest strength of our study is the prospective character and an additional migraine comparison cohort to control for potential effects of the underlying disease. The fact that data collection followed a similar protocol across the three cohorts makes a substantial bias unlikely. Another major strength of our study is that exposure data are protocolled close to the time of intake and do not rely on prescription data.
Conclusion
Our findings support the evidence that triptans are not major teratogens. Moreover, our findings do not indicate a substantial risk of the migraine disorder itself for birth defects or other adverse pregnancy outcomes. When compellingly needed during pregnancy, sumatriptan, as the best studied triptan, appears an acceptable treatment option. A detailed fetal ultrasound should be offered in cases of first trimester exposure to less well-studied triptans.
Clinical implications
In this observational cohort study, the use of established triptans appears to be a safe treatment option for migraine disorder during pregnancy. Analyses did not show increased rates of birth defects, spontaneous abortion or other adverse pregnancy outcomes in comparison to the control groups. Potential teratogenic effects of the migraine disorder itself could not be seen. Data on eletriptan and frovatriptan are still insufficient for definite conclusions.
Footnotes
Acknowledgements
The authors would like to thank their team colleagues for counselling patients and HCP and for the documentary work. Furthermore, they would like to thank all participating physicians and patients who provided detailed information and contributed to the study. Documentation and evaluation of pregnancy outcomes under medication are performed on behalf of the German Federal Institute for Drugs and Medical Devices (BfArM).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.