
Abstract
Aims
To evaluate the impact of treatment success on depression and anxiety symptoms in medication-overuse headache (MOH) and whether depression and anxiety can be predictors of treatment outcome.
Methods
All consecutive patients entering the detoxification program were analysed in a prospective, non-randomised fashion over a six-month period. Depression and anxiety were assessed using the Hospital Anxiety and Depression Scale.
Results
A total of 663 MOH patients were evaluated, and 492 completed the entire protocol. Of these, 287 ceased overuse and reverted to an episodic pattern (responders) and 23 relapsed into overuse. At the final evaluation, the number of patients with depressive symptoms was reduced by 63.2% among responders (p < 0.001) and did not change in relapsers (p = 0.13). Anxious symptomatology was reduced by 43.1% in responders (ps < 0.001) and did not change in relapsers (p = 0.69). At the multivariate analysis, intake of a prophylactic drug and absence of symptoms of depression at six months emerged as prognostic factors for being a responder (OR 2.406; p = 0.002 and OR 1.989; p = 0.019 respectively), while lack of antidepressant drugs and presence of symptoms of depression at six months were prognostic factors for relapse into overuse (OR 3.745; p = 0.004 and OR 3.439; p = 0.031 respectively).
Conclusions
Symptomatology referred to affective state and anxiety can be significantly reduced by the treatment of MOH. Baseline levels of depression and anxiety do not generally predict the outcome at six months. Their persistence may represent a trait of patients with a negative outcome, rather than the consequence of a treatment failure.
Introduction
Medication overuse headache (MOH) is a well-known disorder characterised by chronic headache associated with regular overuse of symptomatic medications, according to the International Classification of Headache Disorders 3rd edition (Beta version) (1). MOH usually is the result of the progressive worsening of a migraine associated with the increasing intake of symptomatic drugs (2,3), although other types of primary headache have been associated with medication overuse (4,5). MOH represents a transient diagnosis, and drug withdrawal is a critical step in order to confirm the involvement of symptomatic drugs and/or for further refinement of diagnosis and treatment. In this sense, detoxification treatments based on withdrawal of the overused medications have proved effective in reverting the headache pattern from chronic to episodic within two months in the majority of patients receiving a diagnosis of MOH (6). To this end, there are many different treatments that could be used for achieving withdrawal from overused drugs, which range from education and a simple advice strategy (7) to proper detoxification according to outpatient or inpatient protocols (8). The choice of inpatient detoxification seems to be more appropriate and effective for complicated – i.e. characterised by multiple psychiatric comorbidities – MOH patients (9,10). Unfortunately, in a minority of patients, drug withdrawal is unsuccessful either because patients fail to stop drug overuse or because overuse discontinuation is not associated with an improvement of the headache (11–13). Psychiatric comorbidities, such as anxiety and depression, are two to 10 times more prevalent among people with migraine than in the general population, and more than 25% of migraineurs fulfill the criteria for these diagnoses (14–15). These considerations are particularly important for MOH, being in general associated to more psychiatric comorbidities than episodic headache types (16,17). For instance, both anxiety and depression are often associated with frequent headache and medication overuse (e.g. 16,18), even if the direction of the cause-effect relationship still needs to be fully understood. In addition, many factors, such as gender, type of primary headache disorder, overused medication, and dependence levels (19,20), may be involved in the prognosis and outcome of MOH, and their understanding has become a topic of interest in the current debate. Even less is known about the role of anxiety and depression in the response to treatments. A study conducted on a small MOH population (21) reported that depression, as measured via the Hospital Anxiety and Depression Scale (HADS) (22), was a predictor of a stable response to a detoxification program for up to four years. Such a finding was recently confirmed by an Italian 12-month longitudinal study (23) highlighting the predictor role of baseline self-reported depression scores for both relapse into chronic migraine and the need for another structured withdrawal. Taken together, these results suggest that the measurement of psychiatric comorbidities is important in the management and prognosis of MOH.
The Comoestas study is a multicentric multinational prospective study for the evaluation of the efficacy of a consensus treatment protocol in MOH subjects followed up for six months with a paper diary or with an electronic monitoring and alert system (24–26). In this paper, we report the results of a post-hoc analysis of the Comoestas database that was performed to evaluate in depth for a large and well-characterised population of MOH subjects i) the impact of treatment success on the symptoms of anxiety and depression in medication-overuse headache (MOH) and ii) whether symptoms of depression and anxiety can be associated to the treatment outcome.
Methods
Participants and study design
Design and results of the COMOESTAS study have been described elsewhere (24–26). Briefly, the Comoestas study was a multicenter study aimed at comparing the relapse rates six months after detoxification between MOH patients monitored with an electronic or a paper diary. Patients with MOH according to the criteria of ICHD-2, subsequently confirmed also with the ICHD-3 criteria, were recruited consecutively from August 2008 to February 2009 in six headache centres: Four in Europe (Italy, Denmark, Germany and Spain) and two in Latin America (Argentina and Chile). If eligible, patients were allocated to standard care with a paper diary or to structured care with an electronic diary (25). All patients underwent drug withdrawal followed by optional prophylactic treatment, according to a consensus protocol published elsewhere (2) and were followed up for six months.
Procedures
The procedure has been previously explained in detail (24,25). Briefly, at visit 0, patients were informed individually about MOH and the treatment programme by a specialised headache nurse or physician and began keeping a headache diary. One month later, at visit 1 (Day 0), the headache diary was checked and patients who still fulfilled the inclusion criteria were included in the study and underwent detoxification as inpatients (daily hospitalisation or regular hospitalisation) or as outpatients. Detoxification lasted seven days and consisted of the abrupt discontinuation of overused acute medications, which were substituted with rescue medications. As of Day 8, the patients were allowed only two days/week with symptomatic medications, different from the overused ones. Prophylactic treatment was optional; when prescribed, it was started on Day 1 and the choice was based on the patients’ characteristics and preferences, efficacy, and the side effects of previous treatments and co-morbid disorders. At visit 2 (two months after day 0) the patients returned to the headache centre for a follow-up visit. Visit 3 (six months after day 0) completed the study.
Levels of depression and anxiety were evaluated using the Hospital Anxiety and Depression Scale (HADS) (22) at baseline and at the six-month follow-up. The cut-off for the diagnosis of anxiety or depression was set at 8 (27). Hence, two groups of psychopathology were defined in this study: Case level anxiety (HADS-A ≥ 8) and case level depression (HADS-D ≥ 8). The study was approved by the local ethics committees from all centres apart from Denmark, where the local ethics committee stated that approval was not necessary because the study did not foresee any new pharmacological treatment. Participants gave informed consent before taking part.
Data management
We collected clinical data by means of a dedicated web-based platform (the Comoestas platform). Access to the electronic database was granted to participating centres following specific training and instructions. All centres were required to perform data entry in real time. Data input was continuously monitored by the coordinating centre (Mondino) for timely addressing of any missing information, logical errors, insufficient detail, or any other queries.
Endpoints and statistical analysis
For data analysis, we adopted the following possible outcomes (24,25):
Non-overusers at two months: That is, those who remained overuse-free regardless of their headache pattern (episodic or chronic). Responders: That is, patients who were overuse-free and had fewer than 15 headache days/month during the entire six-month observation period; Relapsers: That is, patients who became overuse-free at two months, but relapsed back into overuse in any month between three and six.
Note that the subjects who were still overusing at two months were excluded from the subsequent analyses. Data are presented as means with standard deviations in brackets. We used the Student’s paired and independent t-tests for data following a normal distribution. For dichotomous data, we used the χ2-test. Univariate and multivariate logistic regression (forward method) were applied to determine the predictors of the three outcomes (overuse at two months, responder, and relapser at six months), as defined above. The criterion for inclusion of variables in the multivariate model was statistical significance at the level of p ≤ 0.05, obtained by univariate analysis. An alpha of 0.05 was used for all statistical tests. Given that participants received two different protocols of care (paper diary versus electronic diary), we ran statistical analysis separately in the two groups of patients before analysing the total population as a whole. The same pattern of results was observed in the two groups separately and in the whole population when controlling for the care protocol received. For this reason, in the following paragraphs we are presenting the results obtained with analyses on the population as a whole, according to the outcome of interest. The SPSS 23.0 statistical software package was used to perform the statistical analysis.
Results
Patient population
Baseline characteristics of patients that completed the study. The primary headache type was assessed based on history.

Data are presented as means with standard deviations or percentages in brackets. MIG: migraine; TTH: tension-type headache; MOH: medication-overuse headache; HADS: Hospital Anxiety and Depression Scale.

Clinical pattern on six month follow-up.
HADS anxiety and depression score at baseline
According to HADS, a total of 249 (50.6%) patients fulfilled the criteria for depression and 300 (61.0%) for anxiety at baseline (n = 492).
When comparing the non-overuser and overuser groups at two months, we observed that at baseline, the percentage of depressed patients was significantly smaller in the non-overuser group (n = 178, 36.3%) when compared to the overuser group (n = 52, 60.5%) (p < 0.001), whereas these two groups were similar in terms of anxiety (n = 247, 50.3% and n = 49, 57.0% for non-overuser and overuser subjects, respectively) (p = 0.15).
When analysing the responder and non-responder groups, we found that at baseline patients fulfilling the criteria for depression were equally distributed in the two groups: Responders n = 95, 33.1%, and non-responders n = 45, 37.5% (p = 0.23). The same was also true for anxiety: Responders n = 144, 50.2%, and non-responders n = 54, 45.0% (p = 0.20).
When comparing relapsers with non-relapsers, we observed that at baseline, a greater proportion of relapsers (n = 14, 60.9%) fulfilled the criteria for depression when compared to non-relapsers (n = 140, 34.4%) (p = 0.011), whereas these two groups did not differ as regards anxiety (n = 12, 52.2% and n = 198, 48.6% for relapsers and non-relapsers respectively) (p = 0.45).
When reasoning in terms of absolute values, HADS scores at the baseline (n = 492) were: 6.4 ± 3.8 for depression and 7.8 ± 4.1 for anxiety.
Non-overuser patients (6.3 ± 3.8) scored lower at the HADS depression subscale than overuser patients (7.5 ± 3.7) (p = 0.007) at baseline. Non-overuser and overuser groups were similar for their HADS anxiety scores (non-overuser: 7.9 ± 4.1, overuser: 8.5 ± 4.0) (p = 0.17).
No differences resulted at baseline between responder and non-responder groups in the HADS depression (responder: 6.1 ± 3.7, non-responder: 6.1 ± 3.7) (p = 0.99) and HADS anxiety (responder: 7.9 ± 4.1, non-responder: 7.3 ± 4.0) (p = 0.15) scores.
Relapsers (8.3 ± 4.1) scored significantly higher at the HADS depression subscale than non-relapsers (6.1 ± 3.7) at baseline (p = 0.007). Relapsers and non-relapsers were, however, similar as regards their HADS anxiety scores (relapsers: 7.8 ± 4.1, non-relapsers: 7.7 ± 4.1) (p = 0.94) scores.
Changes in the percentage of subjects with symptoms of depression or anxiety from baseline to the six-month follow-up
At the end of the study (n = 492), the number of patients with depression was reduced by 51.3%, that is, from 193 (39.0%) to 94 (19.0%) (p < 0.001), while the number of those with anxiety was reduced by 36.1%, from 244 (49.3%) to 156 (31.5%) (p < 0.001).
When analysing the responder and non-responder groups, the percentage of patients with depression was reduced significantly in both groups: By 63.2% in the responder group [from 95 (33.1%) to 35 (12.2%) (p < 0.001)] and by 44.4% in the non-responder group [from 45 (37.5%) to 25 (20.8%) (p = 0.001)]. Similarly, the proportion of patients with anxiety at six months was reduced in both groups: By 43.1% in the responder group [from 144 (50.2%) to 82 (28.6%) (p < 0.001)] and by 22.2% in the non-responder group [from 54 (45.0%) to 42 (35.0%) (p = 0.038)].
The analysis of the relapser and non-relapser groups showed that at six months the percentage of patients fulfilling criteria for depression in the non-relapser group was reduced by 57.1%, from 140 (34.4%) to 60 (14.7%) (p < 0.001), whereas it was substantially stable in the relapser group (baseline: 60.9% n = 14, six months: 43.5% n = 10) (p = 0.13). The proportion of patients with anxiety at six months was also reduced in the non-relapser group when compared to baseline by 37.4%, from 198 (48.6%) to 124 (30.5%) (p < 0.001), whereas it was stable in the relapser group (baseline: 52.2% n = 12, six months: 43.5% n = 10) (p = 0.69).
When reasoning in terms of absolute values, in the whole group of 492 patients the HADS depression score was reduced from 6.4 ± 3.8 at baseline to 4.0 ± 3.6 at six months (p < 0.001), and the HADS anxiety score was reduced from 7.8 ± 4.1 at baseline to 6.0 ± 3.7 at six months (p < 0.001).
Hospital Anxiety and Depression Scale scores at baseline and at the follow-up, as a function of group.

Data are presented as means with standard deviations. HADS: Hospital Anxiety and Depression Scale. +Outcome based on the two-month follow-up; *Outcome based on the six-month follow-up.
Both responders and non-responders showed a reduction in their HADS depression and anxiety scores across the six-month period; however, the entity of change in both depression (−49.2% for responders and −27.9% for non-responders) and anxiety (−30.7% for responders and −11.0% for non-responders) scores were significantly more pronounced in the responder than in the non-responder group (p < 0.012).
Finally, in patients not relapsing, HADS depression and anxiety scores were significantly reduced from baseline to six months (−42.6% for depression and −24.7% for anxiety), whereas they were stable in the relapser group.
Given that some patients received a prophylaxis therapy at discharge, in some consisting in antidepressant drugs, we repeated analyses controlling for these variables. The same pattern of results was observed; hence we did not report these data.
Factors associated with the treatment outcome being ‘non-overuser’ at two months
Model fit of logistic regression equations to predict effects of treatment.
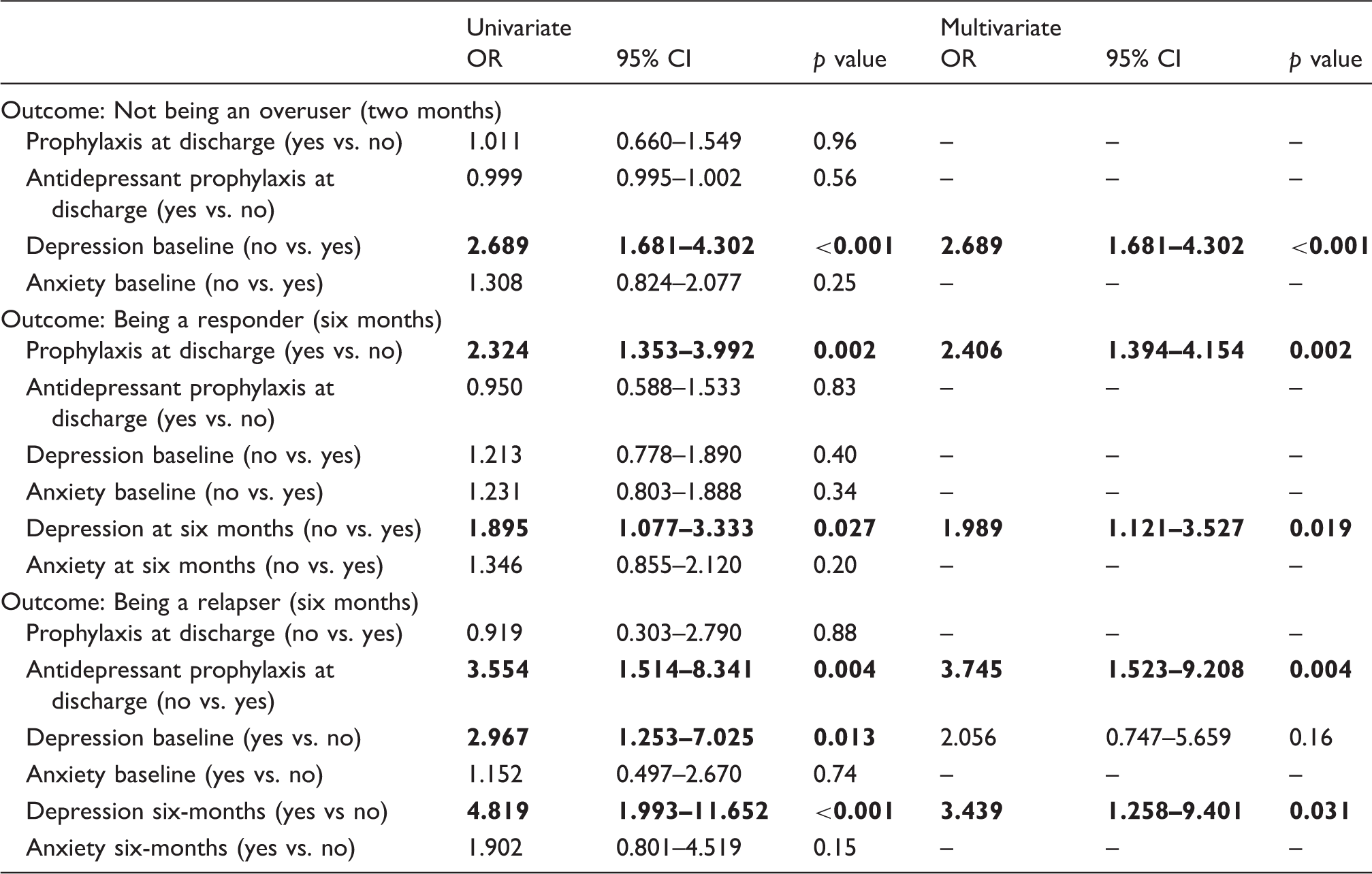
Significant OR are in bold.
Factors associated with the treatment outcome being ‘responder’ at six months
According to the results of the univariate analysis (Table 3), the factors involved in this outcome were: Having received a prophylaxis treatment at discharge (OR 2.324; 95% CI 1.353–3.992, p = 0.002) and not fulfilling the criteria for depression at six months (OR 1.895; 95% CI 1.077–3.333, p = 0.027). In a multivariate analysis, both factors emerged as associated with being a responder (prophylaxis treatment at discharge: OR 2.406; 95% CI 1.394–4.154, p = 0.002; not fulfilling the criteria for depression at six months: OR 1.989; 95% CI 1.121–3.527, p = 0.019). This logistic regression model was statistically significant, χ2(2) = 9.87 p = 0.007, and it explained 3.4% (Nagelkerke R2) of the variance of overuse persistence after six months from detoxification and correctly classified 70.5 % of cases.
Factors associated with the treatment outcome being ‘relapser’ at six months
According to the results of a univariate analysis (Table 3), the factors involved in this outcome were: Not having received an antidepressant prophylaxis therapy at discharge (OR 3.554; 95% CI 1.514–8.341, p = 0.004), fulfilling the criteria for depression both at the baseline (OR 2.967; 95% CI 1.253–7.025, p = 0.013) and after six months (OR 4.819; 95% CI 1.993–11.652, p < 0.001). In a multivariate analysis, the risk factors associated with being relapser were: Not having received an antidepressant prophylaxis therapy at discharge (OR 3.745; 95% CI 1.523–9.208, p = 0.004) and fulfilling the criteria for depression at six months (OR 3.439; 95% CI 1.258–9.401, p = 0.031). This logistic regression model was statistically significant, χ2(3) = 22.07, p < 0.001 and it explained 15.1% (Nagelkerke R2) of the variance of overuse persistence at six months and correctly classified 94.9 % of cases.
Discussion
The main finding of this study is that symptoms of depression and anxiety in MOH patients are significantly reduced by the treatment proposed (drug withdrawal followed by optional prophylactic treatment) and that such reduction varies according to the type of outcome. Some authors (11,28,29) previously reported changes in psychiatric comorbidities after detoxification, but they did not differentiate this reduction as a function of the outcome. What is interesting in our study is that such a decrease is related to the success of the treatment itself. This suggests that not all MOH patients are equal. In particular, those patients with a positive outcome after treatment are those in whom depressive and anxious symptoms could also be reduced after the intervention, being probably the result of disabling headaches instead of a stable characteristic. This finding seems to suggest that the positive effects of the treatment program could be extended indirectly also to the psychological dimensions. The situation is different for those patients having a negative outcome after treatment. It is possible that they were more complicated patients (e.g. 30,31), in whom anxiety and depression might not be reactive to the chronic pain condition, but rather one of the causes. This group of patients might represent a group of subjects who are in need of specific treatments, more targeted for addressing psychopathological aspects (10). In this respect, Munskgaard and colleagues (11,31) demonstrated the efficacy of multidisciplinary treatments, including physicians, nurses, physiotherapists, and psychologists, tailored for treatment-resistant MOH patients. According to this line of reasoning, comorbidity with anxiety and even more so, depression, might be associated with the negative outcome and play a role in perpetuating medication overuse. In this regard, it is noteworthy that we recently found (32,33) that the failure of a detoxification program was related to specific psychological and personality disturbances.
When considering the outcome of ceasing overuse at the two-month follow up, the existence of mood disorders at baseline resulted as a risk factor, in line with other studies (e.g. 21). What is interesting here is that the pattern of findings was different when we considered data from the six-month follow up, showing a more predominant association between the outcome and the affective state after than before treatment. In particular, we found that the affective state after six months – together with the pharmacological regimen at discharge – were associated with the positive outcomes. In contrast, we did not find any role of anxiety as regards the three possible outcomes (overuse, responder, relapser). These data are particularly interesting as they highlight the combined relevance of the therapeutic regimen at discharge together with the patients’ psychological state.
To the best of our knowledge, only a few studies (28,34,35) have evaluated changes in terms of depression and anxiety after a detoxification program according to the outcome. However, two main differences can be observed between those studies and the present one. First, our study comprised a larger population of patients (492 patients vs 100 or fewer patients). Second, we focused on three different outcomes. The fact that slight differences resulted across these three outcomes highlights the importance and the necessity for considering the outcome of detoxification programs from different points of view. Hence, for all these reasons, we strongly believe that our results can add further important information to existing evidence.
Migraine is a complex interplay of several different factors, the so-called migraine brain being altered structurally and functionally (36). Neuroimaging studies have shown abnormalities in several brain areas involved in pain processing that normalise their activity after detoxification, and that could be related to the predisposition of patients to different therapeutic responses and to possible relapse in drug abuse (37). Future studies should better explore and clarify this argument also in the light of patients’ psychological state.
The limitations of our study should be acknowledged. First, we assessed mood disorders and anxiety via a self-report questionnaire. Even if this methodology has been adopted in many studies (11,21,26,28), it admittedly does not allow an in-depth evaluation of the psychological state of our patients. Second, we excluded patients with major psychiatric disorders. Both these reasons could explain why the prevalence of mood disorders and anxiety was lower than in other studies using psychiatric evaluations (e.g. 12) based on DSM-IV criteria (38). However, it is important to note that the seven items of the depression subscale of HADS are related to diagnostic criteria of depression in DSM-IV (38), as are six of the seven items of the anxiety subscale. Third, a proportion of our patients received a prophylaxis regimen at discharge. Hence, it could be that changes in psychiatric symptoms are related to psychotropic medications used. We controlled for this factor in our analysis, but the results obtained at the multivariate were not univocal (no effect of antidepressants in the outcome ‘responder’, but possible in the outcome ‘relapsers’), therefore we cannot exclude with absolute certainty a partial role.
In conclusion, our findings suggest that the successful treatment of medication overuse has a significant impact on symptoms of mood disorders and anxiety. The impact varies with the outcome of treatment. A careful psychopathological assessment of patients at baseline, particularly as regards depression levels, may give critical information on the outcome of withdrawal treatment. A psychopathological evaluation also seems important in the follow-up. Indeed, patients who fail to respond to the treatment and show persisting depression at six months should receive targeted care, because they likely represent a sub-group of subjects where chronic pain and depression are strictly intertwined and more difficult to eradicate.
Clinical implications
The successful management of medication overuse has a significant impact on the affective state of patients with medication overuse headache. Baseline levels of depression and anxiety do not predict the outcome at six months, but their persistence represents a risk factor for a negative outcome.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by COMOESTAS Project – EC contract number 215366 (COMOESTAS) FP7 – Thematic priority ICT and by a grant from the Italian Ministry of Health to National Neurological Institute C. Mondino, years 2013–2015.