
Abstract
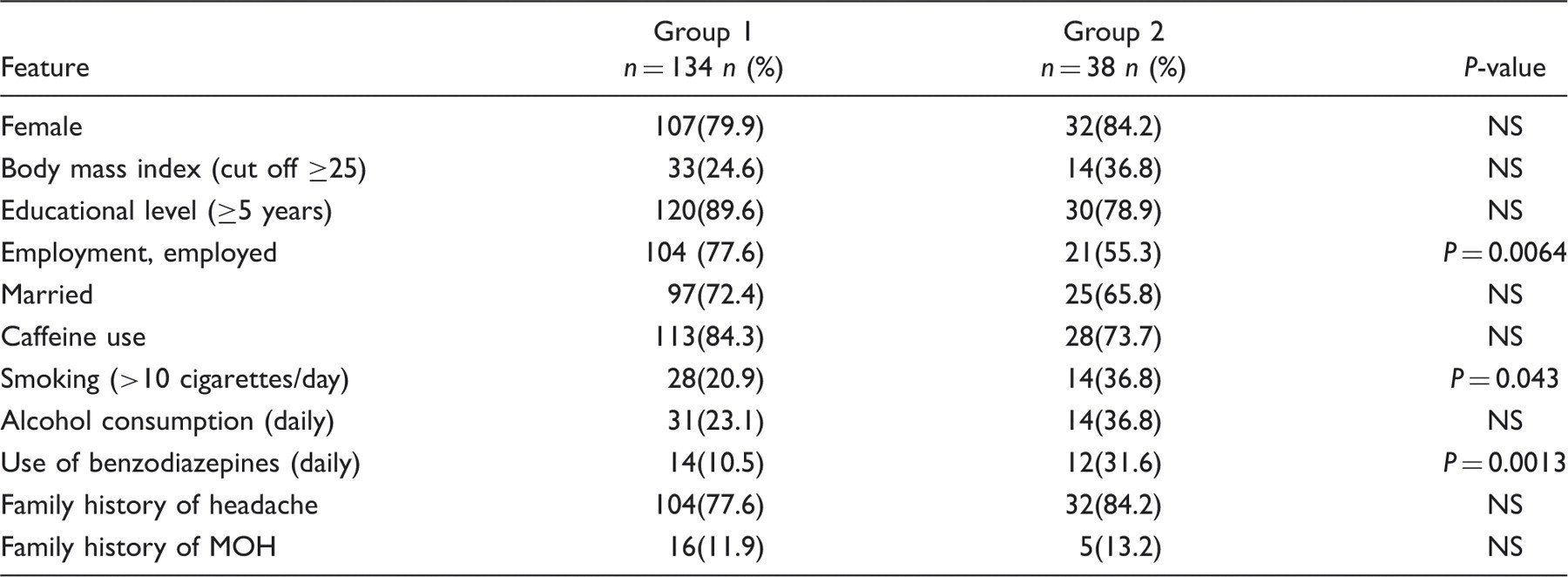
To investigate factors influencing prognosis in medication-overuse headache (MOH), we conducted a 12-month follow-up of patients with probable MOH. We recruited 215 patients consecutively admitted to our headache centre for an inpatient detoxification treatment. We analysed likely predictor factors for headache resolution (sex, age, primary headache, psychiatric comorbidity, type and timing of overuse). Mann–Whitney U-test and chi-squared test were used. One year after withdrawal, we had complete data on 172 patients (80%): 38 of these patients (22%) had relapsed into overuse and 134 (78%) had not. The negative prognostic factors for relapse were: intake of more than 30 doses/month (P = 0.004), smoking (P = 0.012), alcohol consumption (P = 0.037), non-confirmation of MOH diagnosis 2 months after detoxification (P = 0.000), and return to overused drug(s) (P = 0.000). The 1-year relapse rate was 22%. The existence of sub-groups of MOH patients with such risk factors could influence treatment strategies.
Introduction
Medication-overuse headache (MOH) is a growing problem and a challenge for headache specialists. It is crucial to identify the prognostic factors for MOH in order to clarify its aetiological and pathophysiological mechanisms and to achieve the best therapeutic approach, starting with the first step of drug withdrawal.
The prevalence of MOH in the general population is about 1–2% (1). In headache-centre populations, this figure rises to 55–70% (2,3), underlining its impact in this clinical setting. Patients overusing symptomatic medications for diseases other than headache do not develop MOH, with the exception of some subjects with pre-existing migraine (4). Whereas migraine is recognized, in different studies, as the most prevalent primary diagnosis in MOH patients, opinion differs as regards the frequency (ranging from 14% to 38%) of ‘pure’ tension-type headache (TTH) in these patients (5–7).
The International Classification of Headache Disorders, 2nd Edition (ICHD-II) (8) incorporated the term medication-overuse headache (MOH) and introduced the sub-category of triptan-overuse headache. After the publication of ICHD-II, however, extensive debate on the classification of MOH soon led to some major changes: the elimination of headache characteristics, the introduction of a new sub-type (MOH attributed to combination of acute medications) (9), and the proposal of criteria for a broader concept of chronic migraine and MOH (10).
Treatment strategies, ranging from simple advice to withdrawing the overused drug or drugs according to structured inpatient care programmes, are also debated, even though abrupt drug withdrawal is accepted as the essential first step. The use of different treatment strategies in unselected populations of MOH patients makes it difficult to compare the different studies. Lake suggested that there are different kinds of MOH (11) and that treatment should be tailored accordingly. The adoption of an advice-only approach in patients with low medical needs and no psychiatric disorders gave good results (12) and strengthened the argument for stratification of patients. However, MOH is associated with the same high psychiatric comorbidity rate as other chronic headache patients (13–15); furthermore, because MOH shows similarities with addiction (16) and dependence-related behaviours (17,18), this situation may be complicated by the presence of certain personality traits. The presence of psychiatric comorbidity is a negative prognostic factor for headache improvement or resolution (19,20), and in MOH is suggested to be related to headache chronification (18). In short, in MOH, psychological factors may contribute to the progression from drug use to abuse, and from headache to rebound headache.
The possibility of relapse, estimated to occur (mainly in the first year) in 30–45% of patients with MOH (21–23), is another aspect that may influence the therapeutic approach. In a 4-year follow-up study, Katsarava et al. (21) found a lower relapse rate in patients with migraine (31.5%) than in those whose primary headache was TTH (91%) or a combination of migraine and TTH (70%). A second predictor of relapse is the type of abused drug: patients overusing triptans showed a lower relapse rate than patients overusing other analgesics. The vast majority (94%) of patients relapsed during the first year after withdrawal, and the other factors analysed (gender, age, duration of primary headache, drug abuse and intake of preventive medications) did not predict relapse rate.
Another issue to be examined is how to classify MOH patients who do not respond to drug withdrawal, or who initially respond but subsequently relapse. Are they ‘false’ MOH cases, or instead affected by a more complicated sub-form of MOH that is more difficult to treat? A study of selected patients with low medical needs and no psychiatric disorders showed a response rate of 85% in patients receiving only advice to withdraw the overused drug (12). Other studies not selecting patients with an initial diagnosis of probable-MOH found 30–36% of non-responders to different detoxification programmes (24,25).
We conducted a prospective, 12-month follow-up of MOH patients enrolled in our headache centre's CARE protocol. Our main aim was to identify factors related to the 1-year prognosis, by comparing sub-groups with and without resolution of chronic headache after inpatient detoxification.
Methods
This study was conducted at the headache unit (a tertiary referral centre) of the C. Mondino Institute of Neurology in Pavia, Italy. All consecutive patients participating, for the first time, in the centre's inpatient detoxification programme between May 2004 and October 2006 were analysed in a prospective, non-randomized way. They were enrolled as outpatients and gave their verbal informed consent to undergo the protocol, which consisted of an inpatient detoxification treatment and three follow-up visits over the following year. For the 2 months prior to the detoxification treatment, the patients kept a detailed headache diary (26), which was reviewed on their admission to hospital. All the patients underwent the standard CARE withdrawal protocol, described in a previous study (27), and continued to keep a headache diary during hospitalization.
The diagnosis of MOH was made according to the revised ICHD-II criteria (8).
All the participants were assessed by the same neurologist using an ad hoc data sheet. A comprehensive personal and family history of each patient was taken, paying particular attention to their headache history and profile of drugs used. Each subject was analysed by a psychologist, who used clinical interviews and the Structured Clinical Interview for DSM-IV Disorders (SCID-I) (28) to make diagnoses according to Axis I of the DSM-IV (29). During their hospital stay, all the patients received educational and rehabilitative counselling, including instructions for the post-discharge period. On discharge, we asked patients to continue keeping the headache diary and scheduled follow-up visits for 2, 6 and 12 months post-discharge. At each of these visits, the pattern of the headache reported by the patient was checked against the information reported in the diary. The first telephone contact was scheduled at 1 month after discharge, the second one after 9 months.
At the end of the follow-up period, we compared two groups: Group 1 (patients overuse-free 1 year after withdrawal) and Group 2 (failing to respond to detoxification or relapsed). We analysed the likely predictor factors of headache resolution, such as sex, age, type of primary headache, type of overused drug, timing of overuse (days and doses per month, duration of overuse in months, duration of chronic headache in months), psychiatric comorbidity, socio-demographic characteristics and past medical history. Patients overusing more than one class of drug were labelled ‘polyabusers’. Patients not presenting to the scheduled controls were considered as drop-outs.
For statistical purposes, we first analysed single risk factors using the Mann–Whitney U-test for quantitative variables and the chi-squared test for binary data. The level of significance was set at 5%. Subsequently, logistic regression analyses were carried out to estimate the strength of associations between likely risk factors, ascertained at the first examination, and relapse into overuse at 1-year follow-up. We used a logistic regression model based on the forward likelihood ratio method. The Statistical Package for the Social Sciences (SPSS, version 14.0; Chicago, IL, USA) was used for statistical analysis.
Results
Patient population
Two-hundred and fifteen patients (40 males, 175 females) with a mean age of 44.8 ± 11.3 years and a diagnosis of probable medication-overuse headache (p-MOH) according to the revised ICHD-II criteria (8) were included in the study.
One year after inpatient detoxification, we had complete follow-up data sets for 172 patients (80%). One-hundred and thirty-four (27 males, 107 females; mean age 45.6 ± 11.1 years) were still overuse-free at the 1-year follow-up (Group 1), while 38 (6 males, 32 females; mean age 45.6 ± 12.7) were still (or again) presenting medication overuse (Group 2).
Forty-three subjects were lost to follow-up (7 males, 36 females; mean age 41.2 ± 9.0). Seventeen patients dropped out at the 2-month follow-up and 26 at 1 year. We were able to contact 36 of these patients (83.7%): six had themselves decided not to return to the centre, while 30 had failed to comply with the protocol.
No significant differences in demographic data and clinical history were found between available patients and those lost to follow-up.
Analysis of risk factors at 1-year follow-up: overusing versus overuse-free patients
At 1 year, 78% (n = 134) of the patients were still overuse-free (Group 1: mean age at hospitalization, 45.6 ± 11.1) while the other 22% (n = 38) were found to be overusing medication (Group 2: mean age at hospitalization, 45.8 ± 12.7) (Fig. 1). Patients with confirmed MOH diagnosis at 2 months (true MOH) have smaller risk of showing persistent abuse or relapse at 1-year follow-up than patients without MOH diagnosis confirmed at 2 months (p-MOH without persistent overuse + p-MOH with persistent overuse) (16/123 vs. 22/49; P < 0.0001). Therefore MOH diagnosis confirmation at 2 months seems to have a positive prognostic value.
Clinical evolution of p-MOH at 2-month and 1-year follow-up.
Demographic and social features of patients without overuse (Group 1) and patients with overuse (Group 2) at 1-year follow-up. Chi-squared test
Past medical history
No aspect of the patients' past medical history (the investigation covered cardiovascular and cerebrovascular disorders, arterial hypertension, snoring, obstructive sleep apnoea, sinusitis, insomnia, head and neck traumas, mandibular joint dysfunction, cervical spine diseases (arthrosis, hernias), thyroid diseases (hypothyroidism, hyperthyroidism, disthyroidism), allergopathies, gastroenterological diseases, previously diagnosed psychiatric disorders and epilepsy) was found to differentiate between the two groups.
Psychological profile
Analysis of DSM-IV axis I disorders in the sample revealed a higher prevalence of dependence disorder in the Group 2 (overusing) than in the Group 1 (overuse-free) patients (26% vs. 11%) (P < 0.05). No other differences were found, with the exception of a trend towards higher percentages of comorbid psychiatric disorders in the overusing compared with the overuse-free group. The relapse rate was 12% in patients without or with only one psychiatric disorder, and 25% in those with multiple psychiatric disorders. However, due to the small size of the sample this difference could not be tested for statistical significance.
Headache history and profile of symptomatic drug overuse
Headache history in the relapsing and non-relapsing groups: t-test for independent samples

Model fit of logistic regression equations to predict relapse at 1 year from likely risks factors (P < 0.5 for all analyses; 2-sided test; R 2 of Nagelkerke = 0.596; -2loglikelihood = 136.659)

The abused drug or drugs
Abused drug and 1-year evolution. Chi-squared test (P < 0.05)

Patients overusing more than one of the above classes of drug, i.e. fulfilling the ICHD-II criteria (from 8.2.1 to 8.2.5) for more than MOH subtype.
Opioids alone, NSAIDs combined with barbiturates or opioids and NSAIDs combined with caffeine.
Discussion
In MOH, there are many factors that may have contributed to the transition from medication use to overuse, and from headache to rebound headache. The diagnosis of MOH is clinically important because patients ‘rarely respond to preventative medication whilst overusing acute medications’ (8).
Zeeberg et al. (24) excluded over a third (121/337, 35.9%) of the patients in their initial sample because they did not stay medication-free; in the resulting study group, the clinical picture remained unchanged in 48% of the patients, and worsened in 7%; the other 45% obtained an improvement simply by discontinuing the offending drug. In a study by Bigal et al. (25), 30.3% of the patients assessed at 1 year were detoxification failures or had relapsed into overuse. In our sample, 28.5% (49/172) of the patients still had chronic headache 1 year after detoxification and could be sub-divided into: (i) patients with chronic overuse and chronic headache; (ii) patients with relapse into overuse and chronic headache; and (iii) patients without overuse but with persistence of chronic headache. We cannot, as yet, explain this failure of almost 30% of the patients to show an improvement at 1 year, and this group warrants particular clinical and research attention. The role of psychiatric comorbidity needs attention as well. The prevalence of psychopathology does not differ statistically between groups, but the trend is towards the increase with increasing severity of headache and the worst prognosis. This fact needs further studies in order to understand the likely mechanisms and their role in the chronification process.
It is hypothesized that MOH patients can be divided into sub-groups with different profiles. According to this suggestion, the first is made up of patients who are responders 2 months after drug withdrawal, who have no or one comorbid psychiatric disorder, who are triptan overusers and/or have a lower intake (doses per month) and fewer days with drug intake and/or headache (≤20), and do not smoke cigarettes or consume alcohol. The second instead comprises patients who are non-responders at 2 months, who record a higher number of doses per month and more days with drug intake and/or headache (≥20), who have comorbid psychiatric disorders (mainly dependence disorder), often associated with overuse of symptomatic drugs with psychotropic effects or NSAIDs in combination with caffeine, and/or daily use of benzodiazepines; these patients are more likely to be unemployed, smokers and alcohol consumers. The first group may benefit from simple, strong advice to withdraw the overused drug, without inpatient detoxification, even though an adequate strategy of care is recommended. The members of the second group would be candidates for inpatient detoxification, integrated with a schedule of follow-ups and psychological treatment tailored to their specific characteristics. A small percentage of patients (6.9% of our sample) did not respond to treatment at all, not even managing to withdraw the overused drug. Further studies are needed in order to verify whether these patients (for headache centres, they are the really difficult nut to crack) in fact constitute a separate, third sub-group of MOH patients. The idea that there are different MOH sub-groups received indirect support in a consensus paper by the German Migraine Society (30), which suggested that inpatient treatment should be restricted to patients who take tranquillizers, codeine or barbiturates, who failed to withdraw the offending drugs as outpatients, or who have high depression scores.
The greater consumption of alcohol and cigarettes in the relapsed patients vs. the non-relapsed ones may be linked to dependence-related behaviour (17).
Surprisingly, we did not find a relationship between the primary headache diagnoses and the 1-year clinical situation. Our p-MOH sample did not include any patients with ‘pure’ chronic TTH, which Zeeberg et al. found to be related to an unchanging or a worse prognosis (31). However, other studies (1,21) found a higher relapse rate when migraine and TTH co-occur (primary headache diagnosis) than in patients with migraine alone. At 1-year follow-up, patients with higher numbers of doses and days with drug intake per month (see Table 2), and enduring headache at second examination (Table 3), had a greater relapse rate than patients with episodic headache at 2 months. Hence, the longer the duration of overuse and the greater the drug intake, the worse the prognosis will be, irrespective of the primary diagnosis or diagnoses.
Unlike Katsarava et al. (21), we did not find an increased risk of relapse related to the consumption of analgesics considered singly, whereas combinations of analgesics did seem to increase the risk. Moreover, analgesics with psychotropic effects and NSAIDs combined with caffeine were associated with the highest relapse rate. In accordance with other studies (21,31), triptans (and ergots) seemed to be related to the best outcome.
Other studies have highlighted the role of psychotropic drugs in the development of MOH and the risk of relapse (21,22,32). Moreover, Smith and Stoneman showed that patients taking combination analgesics containing barbiturates or caffeine are the most difficult to treat (33). Interestingly, Bigal et al. (34) evidenced that the use of opiates and barbiturates was associated with an increased risk of developing transformed migraine, as well as combinations containing acetaminophen or NSAIDs. In line with the literature, we found that the profile of overused drugs influenced outcome: relapsed patients overused symptomatic drugs with psychotropic effects and combinations of analgesics significantly more than patients with a good outcome.
Almost 70% of the patients showed long-term benefits of detoxification and preventive medication. This result was very similar to the 73% reported by Bigal et al. (25). This finding indirectly supports the efficacy of detoxification in the treatment of MOH, as suggested by Bigal et al. (35).
In our study, the 1-year relapse rate was 15.1%, lower than the 41% reported by Katsarava et al. (21), who stressed that the first year after withdrawal is associated with the highest risk of relapse (94% of their patients relapsed within 12 months). Other studies reported relapse rates of between 22 and 44% during the first year of follow-up (36–40). However, studies are not always comparable due to the use of different headache classification systems, different strategies for withdrawal, detoxification and prophylaxis, and different criteria for evaluating improvement. Therefore, the pressing question is what is the best way of managing these difficult cases? The very low relapse rate that we found at 1-year follow-up strongly supports our ‘CARE’ strategy. Based on a strong doctor–patient alliance, ‘CARE’ is a therapeutic approach in which both medical and psychological needs are taken into consideration.
This study offers a contribution to the analysis of risk factors for MOH relapse and some pointers as regards appropriate clinical intervention in patients with MOH, starting with the collection of a complete clinical history. We found, in particular, that patients with an increased rate of relapse at 1 year were those taking greater numbers of doses per month, consuming significant quantities of alcohol or cigarettes, or both, failing to show headache improvement/resolution 2 months after detoxification, and returning to the overused drug(s) after withdrawal. We suggest that patients who fit this profile should, from referral, receive special ‘care’, because they might represent a sub-group of MOH that is particularly difficult to treat.
Footnotes
Acknowledgements
This study was supported by a grant from the Italian Ministry of Health (RC2004-2007) and EC contract Number 215366 (COMOESTAS FP7/thematic priority ICT).