
Abstract
Aim
The aim of this study was to evaluate the psychological factors associated with a negative outcome following detoxification in a 2-month follow-up in medication-overuse headache.
Methods
All consecutive patients entering the detoxification program were analysed in a prospective, non-randomised fashion. Psychiatric conditions and personality characteristics were assessed using the Structured Clinical Interview for DSM-IV Disorders (SCID-I) and the Minnesota Multiphasic Personality Inventory (MMPI)-2. χ2 tests, one-way analyses of variance, and odds ratios (ORs) were used.
Results
A total of 248 patients completed the follow-up: 156 stopped overuse and their headaches reverted to an episodic pattern (Group A); 23 kept overusing without any benefit on headache frequency (Group B); and 51 stopped overuse without any benefit on headache frequency (Group C). The prognostic factors for the outcome of Group B were higher scores on the correction (OR 1.128; p = 0.036), depression (OR 1.071; p = 0.05), hysteria (OR 1.106; p = 0.023), and overcontrolled hostility (OR 1.182; p = 0.04) MMPI-2 scales, whereas those for Group C were psychiatric comorbidities (OR 1.502; p = 0.021) and higher scores on the hysteria scale (OR 1.125; p = 0.004).
Conclusions
The outcome of detoxification is influenced by psychological factors that should be considered when considering treatment strategies.
Introduction
Chronic headache associated with regular overuse of symptomatic medications is classified as medication-overuse headache (MOH) in the International Headache Classification (ICDH-II, ICDH-III beta version) (1,2). MOH usually results from the progressive worsening of a primary episodic headache, generally migraine, in association with the increasing intake of symptomatic drugs. MOH is a transient diagnosis and drug withdrawal should be a necessary step for confirming the causal role of symptomatic drugs and/or for further refinement of diagnosis and treatment. Indeed, withdrawal from overused drug(s) has proved effective for reverting the headache pattern from chronic to episodic within 2 months in the majority of patients receiving a diagnosis of MOH before being detoxified (3), with a mean success rate of 72.4% in a time window of 1–6 months (17 studies, n = 1101 patients) (4). Withdrawal from overused drugs is considered successful when the patient stops overusing drugs for at least 2 months and the headache pattern reverts to episodic (1,2). In this situation, it is possible to properly diagnose the primary headache type according to existing classification criteria (1,2). Withdrawal from overused drugs can be achieved with different protocols, ranging from an ‘advice alone’ strategy (5) to proper detoxification according to outpatient or inpatient protocols (6). Inpatient detoxification seems to be more appropriate and effective for complicated MOH patients (4,7). Unfortunately, in a minority (although relevant) portion of patients, drug withdrawal is either unsuccessful because patients fail to stop drug overuse or overuse is ceased, but this is not associated with a parallel improvement of the clinical situation, even when performed according to the most stringent criteria (8–10). Two scenarios are thus possible: 1) the patient is still overusing drugs and the headache pattern is still chronic; and 2) the patient has stopped overusing, but headache persists in its chronic pattern (i.e. it keeps occurring on ≥15 days/month).
Understanding of the factors that are involved in the prognosis of MOH has become a topic of interest in the current debate. Compelling evidence has suggested a negative prognostic value for psychopathological disorders in all kinds of primary headaches in children or adolescents (11,12), as well as in adults (13). Psychopathological disorders are indeed more prevalent in patients with chronic headache and MOH (14).
Very few studies have, however, addressed the issue of personality characteristics and/or personality disorders in MOH. Some authors have detected specific personality characteristics such as obsessive–compulsive (15) or borderline personality disorders (16) in MOH patients, while others have suggested the occurrence of an addictive behaviour (17,18), although we detected a completely different personality structure in MOH subjects when compared to patients with addiction disorders (19,20).
Prognosis after withdrawal therapy is another critical issue. Some studies have tried to analyse psychological factors as possible predictors of relapses after successful withdrawal therapy. For instance, anxiety, mood disorders, and dependency-like behaviours have been considered to be relapse-predicting factors. In a follow-up study, Hagen and colleagues (21) highlighted that anxiety and depression levels were predictors of being a responder after 4 years. In a previous 3-year follow-up study (10), we found that a specific personality profile (i.e. with high levels of hypochondriasis, depression, paranoia, fears, obsessiveness, bizarre mentation, repression, overcontrolled hostility, addiction admission, social responsibility and marital distress) predicted the persistence of overuse after withdrawal. Other authors failed to identify psychopathological factors that were capable of predicting the response to a detoxification program (22).
While these studies are interesting as they identify some possible psychological factors – such as dependency-like behaviours, anxiety, and mood symptoms – associated with relapse into MOH following drug withdrawal, data are missing on the possible role of personality characteristics in predicting the success or failure of detoxification programs.
In this frame, the aim of this study is the identification of personality variables that may be predictive of the outcome of a standard inpatient detoxification program in subjects with MOH. This is an underexplored area of clinical research that merits further attention. Awareness of the existence of such predicting factors would hopefully prompt optimisation of the management.
Method
Sample recruitment and treatment
This study was conducted at the Headache Center (a tertiary referral centre) of the National Neurological Institute C. Mondino in Pavia, Italy. All consecutive patients with chronic headache and medication overuse undergoing (for the first time) an inpatient detoxification program over a period of 18 months were enrolled and followed-up in a prospective study. The protocol consisted in a 2-month run-in period followed by inpatient detoxification and a 2-month follow-up. After detoxification, the majority of patients were prescribed a preventative therapy (137, 93%), while 15 patients (7%) were discharged without any prescription of prophylactic drugs. The prophylactic regimen was prescribed taking into account the patient’s history and comorbidities, using common preventative agents (calcium antagonists, beta-blockers, tricyclic antidepressants with or without neuroleptics, other antidepressants, and antiepileptic drugs). During the entire study duration, the patients kept a detailed headache diary (23), which was periodically reviewed by the physicians. One telephone contact was also scheduled for the first month after discharge. All patients signed an informed consent form before being enrolled into the study.
All of the patients underwent the standard CARE withdrawal protocol, described in a previous study (24). During hospitalization, all of the patients received educational and rehabilitation counselling, including instructions and treatment prescriptions for the post-discharge period (for details, see (10)). The diagnosis of MOH was made according to ICDH-III-beta criteria (2).
All of the participants were assessed by the same neurologist, who used an ad hoc patient record form. A comprehensive personal and family history of each patient was taken, paying particular attention to the patient’s headache history and profile of drug use. At the beginning of the study, subjects were examined by two clinical psychologists (FG and SP) with long-standing experience by means of the Structured Clinical Interview for DSM-IV Disorders (SCID-I) (25) in order to make diagnoses according to Axis I of the DSM-IV (26), and the Minnesota Multiphasic Personality Inventory (MMPI-2), one of the most widely used and validated tool for the evaluation of the personality profile (27). To this thorough psychological evaluation took part 86, 12 and 39 participants, labelled as Groups A, B, and C, respectively.
Definition of outcomes
We defined detoxification as successful when the patient was no longer overusing symptomatic medication and headache was present for fewer than 15 days/month. Detoxification was considered ineffective when: 1) the patient failed to stop overuse during the 2-month follow-up; or 2) overuse ceased but headache maintained a chronic pattern. Therefore, on the basis of the 2-month outcome, our population was subdivided into three groups as follows.
Group A: detoxification was effective for interrupting overuse and reverting the headache pattern to episodic during the 2-month observation period. The diagnosis in this group was ‘definite MOH’ plus the ‘episodic headache type’. Patients in this group were defined responders.
Group B: patients never stopped overusing drugs and headache persisted to be chronic in the 2-month observation. The diagnosis for this group was ‘probable MOH’.
Group C: patients stopped drug overuse but headache maintained a chronic pattern (≥15 days/month) during the 2-month observation period. MOH diagnosis was ruled out in these patients because overuse clearly did not influence headache pattern.
Patients in Groups B and C were considered non-responders.
Demographic and clinical characteristics of the three groups: Group A = responders; Group B = subjects who failed to stop overuse; Group C = patients who stopped overuse but maintained a chronic pattern of headache.

Psychological characteristics of the three groups: Group A = responders; Group B = subjects who failed to stop overuse; Group C = patients who stopped overuse but maintained a chronic pattern of headache.

SD: standard deviation; SCID-I: Structured Clinical Interview for DSM-IV Disorders; MMPI: Minnesota Multiphasic Personality Inventory; DOC: obsessive–compulsive disorder; L: lie; F: frequency; K: correction; HS: hypochondriasis; D: depression; HY: hysteria; PD: psychopathic deviate; MF: masculinity–femininity; PA: paranoia; PT: psychasthenia; SC: schizophrenia; MA: hypomania; SI: social introversion; ANX: anxiety; FRS: fears; OBS: obsessiveness; DEP: depression; HEA: health concerns; BIZ: bizarre mentation; ANG: anger; CYN: cynicism; ASP: antisocial practices; TPA: type A; LSE: low self-esteem; SOD: social discomfort; FAM: family problems; WRK: work interference; TRT: negative treatment indicators; A: anxiety; R: repression; ES: ego strength; MAC-R: MacAndrew Alcoholism Scale – Revised; FB: frequency back; OH: overcontrolled hostility; DO: dominance; RE: social responsibility; MT: college maladjustment; GM:masculine; GF: feminine; PSPK: post-traumatic stress disorder; MDS: marital distress scale; AAS: addiction admission scale; APS: addiction potential scale.
The following variables were analysed as possible predictors of the above outcomes: presence of psychiatric disorders as evaluated through SCID-I and personality characteristics as assessed using MMPI-2.
Patients not attending the scheduled follow-up appointments were considered drop-outs.
Statistical procedures
Data are presented as means ± standard deviations for continuous data and as n/% for frequency data. The differences between patients responding positively to the detoxification program (Group A) and patients still abusing (Group B) were examined with χ2 tests for categorical variables and one-way analysis of variance (ANOVA) for quantitative variables. Differences between groups in term of scores in each specific MMPI-2 scale and psychiatric diagnoses as detected by the SCID-I were analysed. Because the Italian version of the MMPI-2 was not validated for the special population under study, we preferred to make use of the approximate scores instead of the T-scores. Mean scores for the MMPI-2 scales were compared between groups using a series of one-way univariate ANOVAs. Univariate and multivariate logistic regression (forward method) were applied in order to determine the treatment failure at 2 months, as defined above. The criterion for variable inclusion in the univariate model was the existence of significant differences among groups in the ANOVAs, whereas variable inclusion in the multivariate model was based on statistical significance at the level of p ≤ 0.05 as obtained by univariate analysis. An alpha of 0.05 was used for all statistical tests. The same analyses were carried out comparing Group A with Group C. All analyses were conducted using SPSS.
Results
Patient population
Of a total of 248 patients, 230 completed the follow-up at 2 months (81.3% females, mean age 44.71 years). Of these, 156 patients (68%) stopped their drug overuse following detoxification and their headache reverted to an episodic form (Group A), 23 patients (10%) failed to stop their drug overuse (Group B) and 51 (22%) stopped their drug overuse following detoxification, but their headaches maintained a chronic pattern (Group C) (Figure 1).
Clinical pattern at 2 months of follow-up.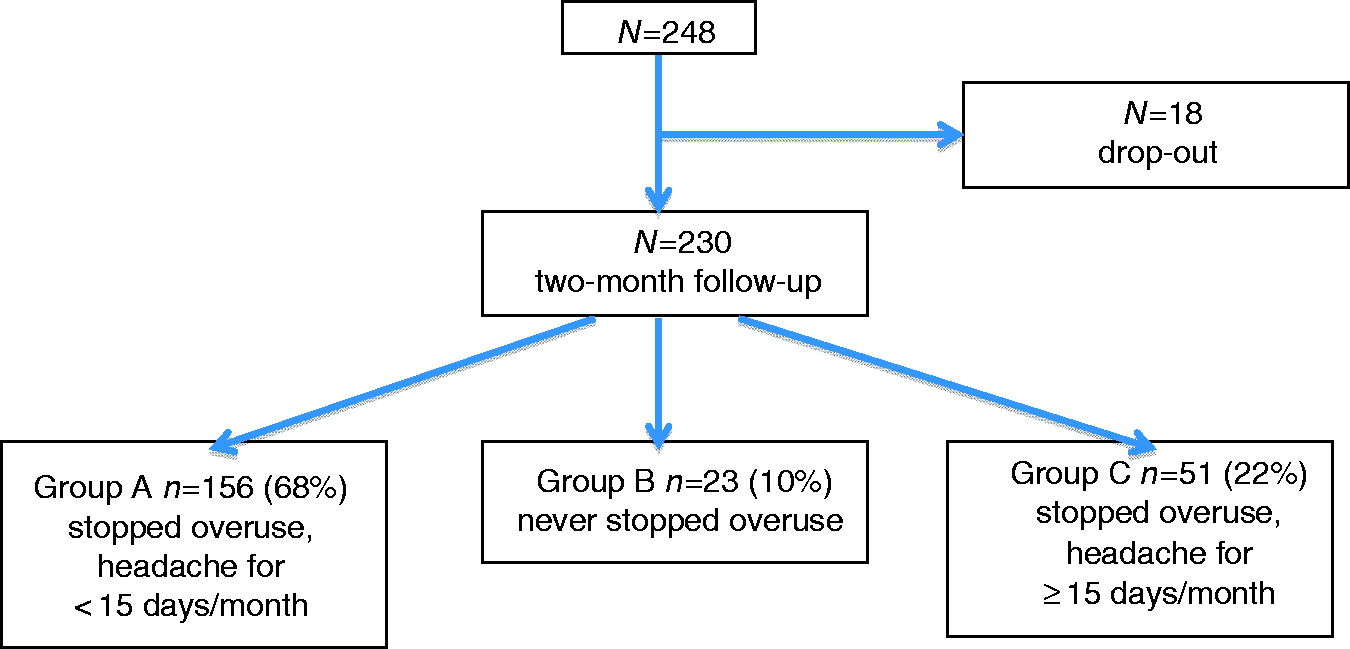
Comparison between Group A and Group B
When comparing demographic and clinical features between these two groups, we observed a higher number of drug doses per month (F(1, 177) = 20.18, p < 0.001) and days with intake per month (F(1, 177) = 5.67, p = 0.018) in Group B (Table 1). In addition, a significant association was found between group and prophylaxis therapy (χ2 = 16.29, d.f. = 6, p = 0.012), with Group A more frequently treated with tricyclics, whereas Group B received more polytherapies.
As regards psychological variables (Table 2), the two groups were similar in terms of psychological assets as measured via SCID-I. Conversely, the two groups differed significantly in several MMPI-2 scales, in which Group B scored significantly higher than Group A: lie (F(1, 96) = 10.01, p = 0.002), frequency (F(1, 96) = 6.03, p = 0.016), correction (F(1, 96) = 5.50, p = 0.021), hypochondriasis (F(1, 96) = 6.19, p = 0.015), depression (D) (F(1, 96) = 5.63, p = 0.02), hysteria (F(1, 96) = 7.31, p = 0.008), paranoia (F(1, 96) = 4.12, p = 0.045), fears (F(1, 96) = 7.80, p = 0.006), obsessiveness (F(1, 96) = 6.06, p = 0.016), depression (DEP) (F(1, 96) =5.81, p = 0.018), health concerns (F(1, 96) = 6.91, p = 0.01), anger (F(1, 96) = 4.35, p = 0.040), low self-esteem (F(1, 96) = 4.50, p = 0.036), social discomfort (F(1, 96) = 7.67, p = 0.007), negative treatment indicators (F(1, 96) = 6.22, p = 0.014), repression (F(1, 96) =8.35, p = 0.005), frequency back (F(1, 96) = 4.98, p = 0.028), overcontrolled hostility (F(1, 96) = 7.08, p = 0.009), marital distress (F(1, 96) = 5.06, p = 0.027) and addiction admission (F(1, 96) = 7.33, p = 0.008). No other differences were found between Group A and Group B in terms of clinical and psychological variables.
Predictors of failure to cease overuse
Model fit of logistic regression equations in order to predict overusing at 2 months from detoxification.
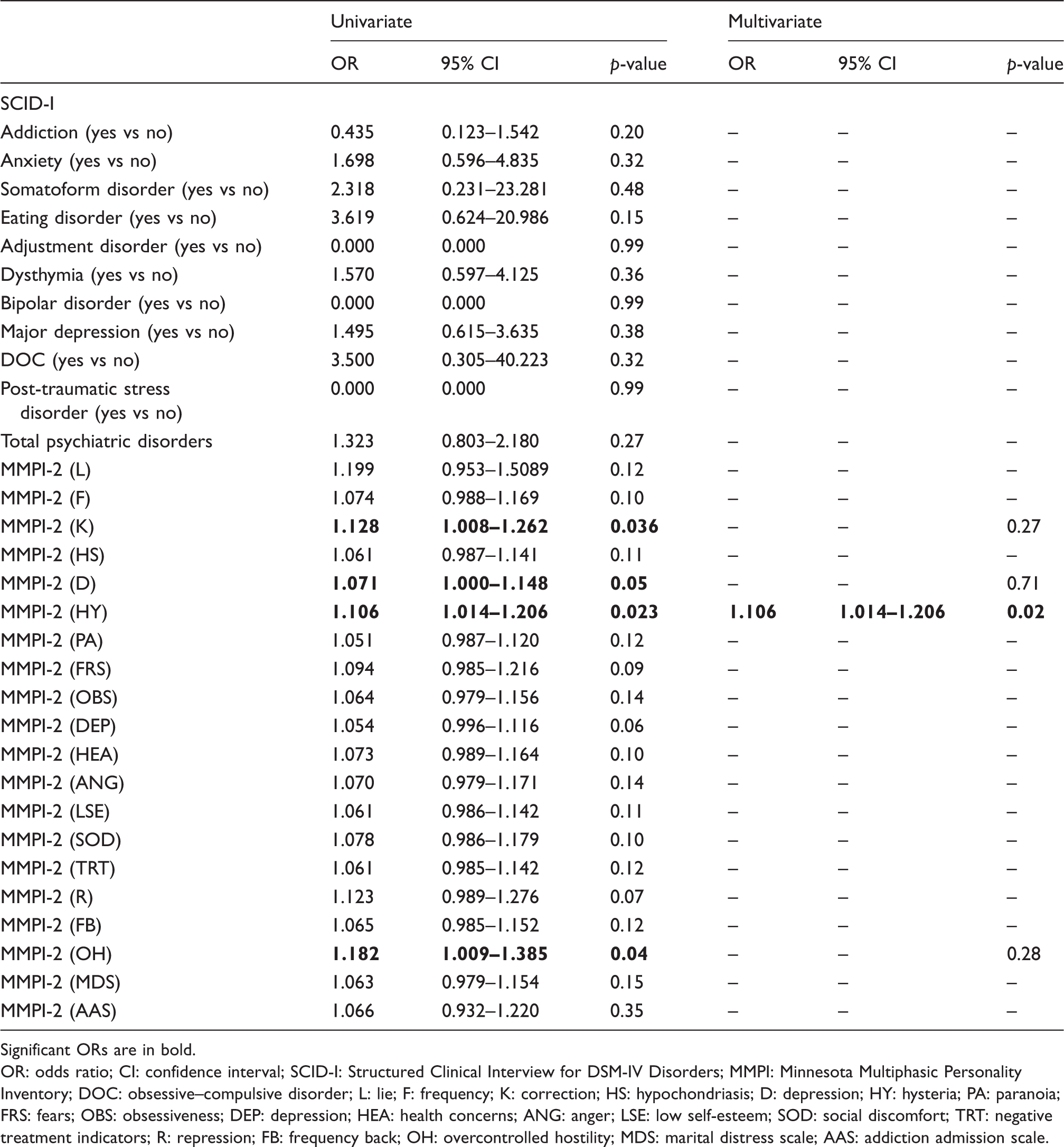
Significant ORs are in bold.
OR: odds ratio; CI: confidence interval; SCID-I: Structured Clinical Interview for DSM-IV Disorders; MMPI: Minnesota Multiphasic Personality Inventory; DOC: obsessive–compulsive disorder; L: lie; F: frequency; K: correction; HS: hypochondriasis; D: depression; HY: hysteria; PA: paranoia; FRS: fears; OBS: obsessiveness; DEP: depression; HEA: health concerns; ANG: anger; LSE: low self-esteem; SOD: social discomfort; TRT: negative treatment indicators; R: repression; FB: frequency back; OH: overcontrolled hostility; MDS: marital distress scale; AAS: addiction admission scale.
In a multivariate analysis, the only factor that emerged as a predictor of failure to cease overuse was having higher scores in the MMPI-2 hysteria scale (OR 1.106, 95% CI 1.014–1.206, p = 0.023). This logistic regression model was statistically significant (χ2(1) =5.90, p = 0.015) and it explained 11.1% (Nagelkerke R2) of the variance of overuse persistence after 2 months from detoxification and correctly classified 88.8% of cases.
Comparison between Group A and Group C
Analysis of demographic and social features showed a significant association between group and primary headache diagnosis (χ2 = 25.03, d.f. = 2, p < 0.001), with patients in Group A tending to suffer more frequently from migraine, whereas patients in Group C suffered more frequently from combined migraine and tension-type headaches.
As regards psychological variables (Table 2), a significant association was found between group and eating disorder (χ2 = 4.84, d.f. = 1, p = 0.028), with a higher prevalence of this kind of disorder in Group C. Moreover, a significant association was found between group and psychiatric comorbidities (χ2 = 4.84, d.f. = 1, p = 0.028), with a larger number of persons affected by psychiatric conditions according to SCID-I in Group C than in Group A.
As regards data collected by using the MMPI-2, patients in Group C showed significantly higher scores than subjects in Group A in the hysteria scale (F(1, 111) = 9.60, p = 0.002). No other significant differences in the clinical and psychological variables were found between these two groups of patients.
Predictors of persistence of chronic headache
Model fit of logistic regression equations in order to predict chronic headache at 2 months from detoxification.
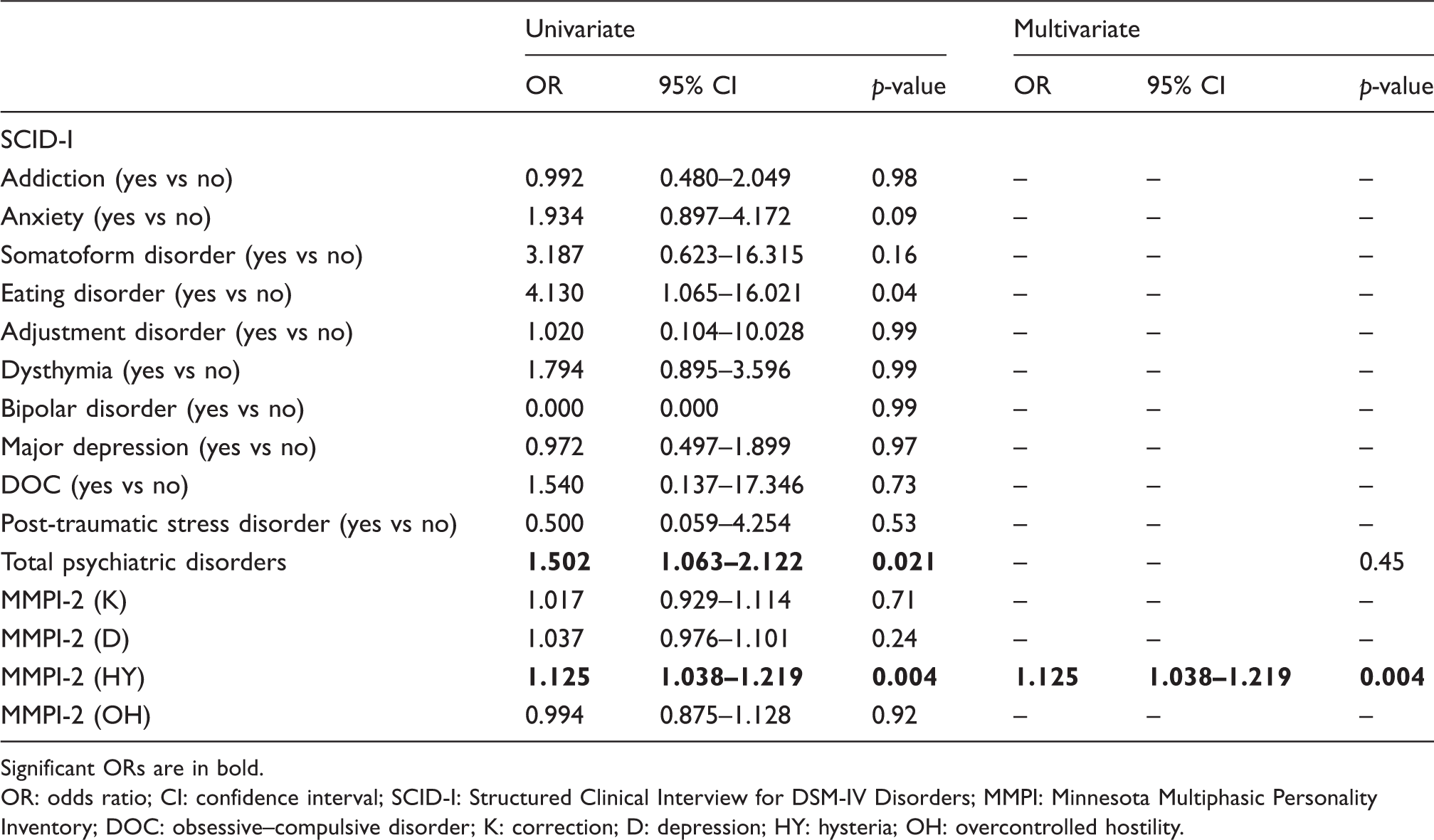
Significant ORs are in bold.
OR: odds ratio; CI: confidence interval; SCID-I: Structured Clinical Interview for DSM-IV Disorders; MMPI: Minnesota Multiphasic Personality Inventory; DOC: obsessive–compulsive disorder; K: correction; D: depression; HY: hysteria; OH: overcontrolled hostility.
In a multivariate analysis, the only factor emerging as predictor of the persistence of the chronic pattern of headache was having higher scores on the MMPI-2 hysteria scale (OR 1.125, 95% CI 1.038–1.219, p = 0.004). This logistic regression model was statistically significant (χ2(1) = 9.20, p = 0.002) and it explained 11.1% (Nagelkerke R2) of the variance in the persistence of the chronic pattern of headache after 2 months from detoxification and correctly classified 74.3% of cases.
Comparison between Group B and Group C
When comparing demographic and clinical features between Group B and Group C, we observed a significantly higher number of drug doses per month (F(1, 72) = 6.99, p = 0.01) in patients who failed to cease overuse. No other significant difference emerged when comparing the two groups of non-responders as regards demographic, clinical, psychological, and personality characteristics.
Discussion
Withdrawal from overused drug(s) is the first objective in the management of MOH (3). A psychological assessment of patients may provide critical information on the outcome before planning the most adequate withdrawal treatment.
Patients who failed to cease overuse showed more pathological personality characteristics (i.e. as measured on the hypochondriasis, depression, hysteria, paranoia, fears, obsessiveness, depression, health concerns, anger, social discomfort, negative treatment indicators, repression, frequency back, overcontrolled hostility, marital distress, and addiction admission MMPI-2 scales) than responders, even if no differences emerged between these two groups in terms of psychiatric conditions (SCID-I). Nevertheless, a form of ‘emotionally overwhelmed’ profile (28) seems to emerge in overusers, characterised by increased scores on the scales detecting neurotic symptomatology and emotional disturbances.
Two important considerations can be made with regards to these results. First, patients who failed to cease overuse (Group B) showed higher scores in the so-called ‘neurotic triad’: depression, hypochondria, and hysteria scales (29,30). This seems in line with what has been found in other studies (e.g., (20,31)) and suggests an excessive concentration on somatic health status, frequent complaints of physical ailments, lack of energy, sleep problems, impaired attention, concentration and low self-esteem, diffidence and pessimism in these patients. All of these conditions together may have contributed to the failure of stopping overusing, even though it is still unclear whether these characteristics represent specific features of people suffering from MOH or whether they should be more broadly attributed to the presence of chronic pain. Other studies have indeed demonstrated the existence of the same neurotic triad in patients with other kinds of chronic pain (e.g. (32)). Thus, it could be hypothesised that this pattern of personality disturbance may belong to chronic pain disorders rather than being specific to MOH. Second, the patients who were still overusing took a higher number of drug doses per month and had more days with intake per month than the responders. Therefore, it is possible that they failed to stop overuse simply because they had more severe levels of drug dependence or a more aggressive type of primary headache. The fact that these patients recorded significantly higher scores on the addiction admission scale seems to supports the former hypothesis. In their 3-year follow-up study, Sances and colleagues (10) found addiction-related personalities in patients who were characterised by overuse behaviour (i.e. patients who never stopped their drug abuse). Hence, it is possible to consider the existence of a small subgroup of patients with symptomatic medication overuse in whom addiction-related personalities may strongly influence the maintenance of the medication overuse after detoxification. In agreement with Lake (7), we therefore suggest the existence of a small group of complicated MOH patients – characterised by multiple psychiatric comorbidities (including Axis II personality disorders) – needing specific interventions that are tailored to their clinical needs.
On the other hand, when comparing responders and patients who are no longer overusing but with a chronic pattern of headache (which, in most cases, satisfied the criteria for chronic migraines), the pattern of findings is different. In terms of personality, these patients differed from responders only by higher hysteria levels. Therefore, in line with the hypothesis of Galli and colleagues (19), they do not show an addiction-related personality, as it is also suggested by the lack of significant differences in terms of medication doses and days with intake. However, these patients were characterised by the presence of a higher number of psychiatric comorbidities. Psychiatric comorbidities indeed represent some of the risk factors that are most widely investigated for headache chronification due the significant roles they may play in this process (11). Psychiatric comorbidity can be both a cause of chronic headache and a consequence of the daily experience of pain (33). Taken together, all of these results are interesting as they point to specific psychological and personality characteristics that could differentiate responders from non-responders.
The pathophysiology of migraine is far from being fully understood, and a complex interplay of several different factors is at the basis of the so-called migraine brain that is altered structurally and functionally (34). The shift from episodic to chronic migraine is uncommon (34), and causative factors other than medication overuse need further study. In our opinion, a pivotal role should be attributed to psychological factors, considering the long-standing evidence on this topic (13), together with shift the focus on the role of personality characteristics. Interestingly, the multivariate analysis identified higher scores on the MMPI-2 hysteria scale as a psychological predictor of detoxification program failure in both types of non-responders (Groups B and C). Hysteria, also known as conversion disorder, refers to the presence of neurological symptoms in the absence of a neurological disease. As a consequence, it is tempting to hypothesise that hysteria might have participated in influencing, on the one hand, the development of chronic migraine (Group C), while on the other hand influencing the failure to cease overuse (Group B). Future studies should better explore and clarify this argument.
In summary, the fact that psychological and personality characteristics seem to be able to predict those patients who will respond to detoxification is quite interesting. This study offers a contribution to the analysis of the risk factors of detoxification failure and some pointers with regards to the optimisation of clinical interventions in patients with MOH, starting with the collection of a complete psychological history. In particular, these patients should be treated with combined pharmacological and psychotherapeutic approaches. We suggest that patients who fit with these psychological and personality characteristics should, from referral, receive special ‘care’, because they might represent a subgroup of MOH that is particularly challenging.
Clinical implications
Personality characteristics differently predicted the detoxification failure/ineffectiveness in cases of failure to cease overuse or stop overuse, with the persistence of a chronic pattern of headache. Personality should be assessed when designing treatment strategies.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This study was supported by a grant from the Italian Ministry of Health to the C. Mondino National Neurological Institute (Current Research 2011–2013).