
Abstract
One hundred and one patients suffering from chronic daily headache (CDH) and medication overuse were treated, in an in-patient setting, with abrupt discontinuation of the medication overused, intravenous hydrating, and intravenous administration of benzodiazepines and ademetionine. The mean time to CDH resolution was 8.8 days. The in-patient withdrawal protocol used was effective, safe and well tolerated. There was a trend for a shorter time to CDH resolution in patients who overused triptans (P = 0.062). There was no correlation between time to CDH resolution and either the type of initial primary headache or duration of medication abuse, whereas time to CDH resolution was related to daily drug intake (P = 0.01). In multiple regression analysis, daily drug intake, age and type of medication overused were independent predictors of time to CDH resolution. At 3-months' follow-up, no patient had relapsed and was again overusing symptomatic medications.
Introduction
Diagnostic criteria of medication overuse headache (MOH) have been recently revised by the International Headache Society (IHS) as part of the new International Classification of Headache Disorders (1), i.e. the clinical characteristics; the duration of symptomatic medications overuse: ≥3 months; the types of medication overused: ergotamine, triptans, simple analgesics, combination analgesics, opioids and other medications; the frequency of days of medication overuse: ≥10 days/month for ergotamine and triptans, ≥15 days/month for simple analgesics and combination analgesics; the time to the daily headache resolution after drug discontinuation: ≤2 months.
MOH is a largely under-diagnosed health condition but its prevalence is increasing worldwide and it has become the third most frequent type of headache (2, 3). According to recent epidemiological studies, the prevalence in the general population is 1–1.4%, with a peak prevalence in women in their 50s. In this age range, in fact, 5% of women meet the diagnostic criteria of MOH (4, 5).
Both out-patient and in-patient detoxification are in use but, for patients with severe rebound headache and withdrawal symptoms or refractory to out-patient management, hospitalization is preferable. Various treatment protocols have been proposed including the use of repetitive intravenous (i.v.) dihydroergotamine (DHE) injections (6–8), oral prednisone (9), repetitive i.v. prochlorperazine (10), pharmacological therapy combined with biofeedback-assisted relaxation (11), behavioural treatment (12), i.v. lignocaine (lidocaine) infusion (13), and naratriptan (14). Although there is general consensus on the need of withdrawal therapy before the introduction of preventive treatment (2, 15–23), guidelines for the treatment of MOH are currently not available given the lack of comparative controlled studies on the efficacy of different therapeutic strategies (2, 15).
The aims of the present study were the evaluation of the efficacy of in-patient detoxification in a sample of MOH patients and the identification of possible predictors of treatment efficacy. To assess efficacy, the time to chronic daily headache resolution (TCDHR) and the number and percentage of patients who had relapsed and were again overusing symptomatic drugs at 3-months’ follow-up have been taken into account.
Patients and methods
We studied all patients referring to the Headache Centre of the Department of Clinical Medicine and Neurology of the University of Trieste, Italy, from January 1999 to December 2003, who fulfilled the IHS Diagnostic Criteria (1) for MOH (code 8.2), i.e. headache present on >15 days/month; ergotamine, triptan, and combination medication intake on ≥10 days/month or simple analgesics intake on ≥15 days/month on a regular basis for ≥3 months; and headache developed or markedly worsened during medication overuse. Patients with known severe psychiatric disorders (i.e. psychosis, major depression with suicidal purposes), alcoholic abuse and/or drug addiction were excluded. Of 111 patients who met the inclusion criteria, 10 (9%), eight women and two men, either refused detoxification (three patients) or declined hospitalization and were treated on an out-patient basis (seven patients). All participants underwent a structured psychiatric interview with a specialist (R.M.A.) to identify psychiatric comorbidity and, if needed, they were treated appropriately depending on their psychiatric condition. Therefore, 90 women (89%) and 11 men (11%), for a total of 101 patients, with a mean age of 55 (SD 13) years, participated in the study. Findings from general, neurological and radiological examinations excluded a secondary headache. According to the recently published IHS Diagnostic Criteria (1), the type of the primary headache from which the patients were suffering before the beginning of chronic daily headache (CDH), the medication(s) overused and the way(s) of administration, the duration of the daily abuse, and the daily drug intake (DDI), i.e. the average number of analgesics dose per day, including analgesics sold with medical prescription and over-the-counter pills, were studied. To compute DDI the minimum effective single dose of a commercially available analgesic drug in Italy was considered.
The 101 study patients were admitted to the Inpatient Unit of the Headache Centre and treated with abrupt withdrawal of the overused medication, i.v. hydrating, i.v. sedative therapy with benzodiazepines (i.e. delorazepam, 2.5 mg b.i.d.), and i.v. ademetionine (S-adenosyl-L-methionine) 200 mg b.i.d. for 7–10 days. More frequent intramuscular administration of benzodiazepines, antiemetics (metoclopramide, 10 mg), and symptomatic medication (SM) different from overused medications was used only in case of severe rebound headache.
Ademetionine (S-adenosyl-L-methionine) is a physiological molecule that is almost ubiquitous in human tissues and fluids, where it influences important biological processes as methyl donor in various reactions of trans-methylation and as precursor of physiological sulphurated compounds in reactions of trans-sulphuration. In particular, the transfer of methyls to biological molecules such as hormones, neurotransmitters, nucleic acids, proteins and phospholipids is a fundamental stage in metabolic and detoxifying processes of the body. The reactions of trans-methylation are of peculiar importance in the brain, because they influence the metabolism of neurotransmitters, such as dopamine, noradrenaline, adrenaline and serotonin, and play a significant role in mood control. Ademetionine (S-adenosyl-L-methionine) has anti-inflammatory, antiprostaglandin, and antileukotriene effects and is also used in detoxification for its antidepressive effects.
During hospitalization, after the resolution of CDH, a personalized prophylactic treatment was started. To meet the patients’ needs for education and support, all patients received counselling sessions before and during the hospitalization. Furthermore, the nurses of the Headache Centre were adequately trained to cope with patients’ psychological problems.
The measure of efficacy of the therapeutic protocol used was the time elapsed from the beginning of the detoxification to the resolution of the CDH (TCDHR). At discharge, all patients were invited to fill in a headache diary and to return for a visit after 3 months in the Ambulatory Unit of the Headache Centre. No patient was lost to follow-up.
The Statistical Package for the Social Sciences (SPSS, version 11.5; SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Parametric and non-parametric tests were used as appropriate. All P-values were based on two-tailed tests and the minimum significance level was 0.05.
Results
The primary headache, pre-existing to CDH onset, was: migraine without aura (MoA) in 75 patients (74.3%), MoA and coexistent episodic tension-type headache (ETTH) in 11 patients (10.9%), migraine with aura (MA) and MoA in 10 patients (9.9%), and ETTH in five patients (4.9%). At hospitalization, the medications overused were: combination analgesics in 42 patients (41.6%), 52.4% by oral administration and 47.6% by rectal administration; simple analgesics in 38 patients (37.6%); triptans in 12 patients (11.9%), and ergotamine in nine patients (8.9%). No patient was taking narcotic analgesics (opioids). The medications overused, the way of administration and the number and percentage of patients according to medication overused are reported in Table 1. Eighty-two patients (81.2%) used to take only one type of medication, while 19 patients (18.8%) used a combination of different drugs. The latter patients were categorized according to the drug most frequently used.
Medications overused, number and percentage of patients, and way of administration in 101 patients with medication overuse headache

The mean length of stay in hospital was 10 (SD 4) days.
The number and percentage of study patients with MOH and their gender, age, initial primary headache, duration of daily abuse, DDI and TCDHR, according to the medication overused, are shown in Table 2. Among abusers of different types of medication there were no differences in gender distribution and age, in the duration of daily abuse, or in DDI (
Characteristics of 101 patients suffering from medication overuse headache according to the medication overused
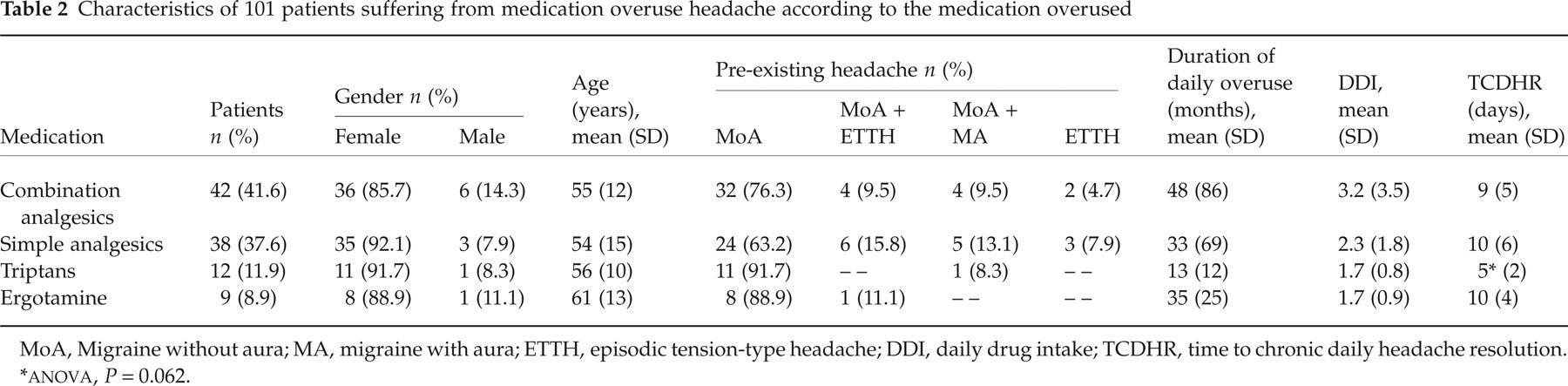
MoA, Migraine without aura; MA, migraine with aura; ETTH, episodic tension-type headache; DDI, daily drug intake; TCDHR, time to chronic daily headache resolution.
In the whole sample of patients, mean TCDHR was 8, 8 (SD 5) days.
Dividing patients according to the initial primary headache, no differences were found in TCDHR (
Time to chronic daily headache resolution (TCDHR) according to the pre-existing primary headache and the type of medication overuse
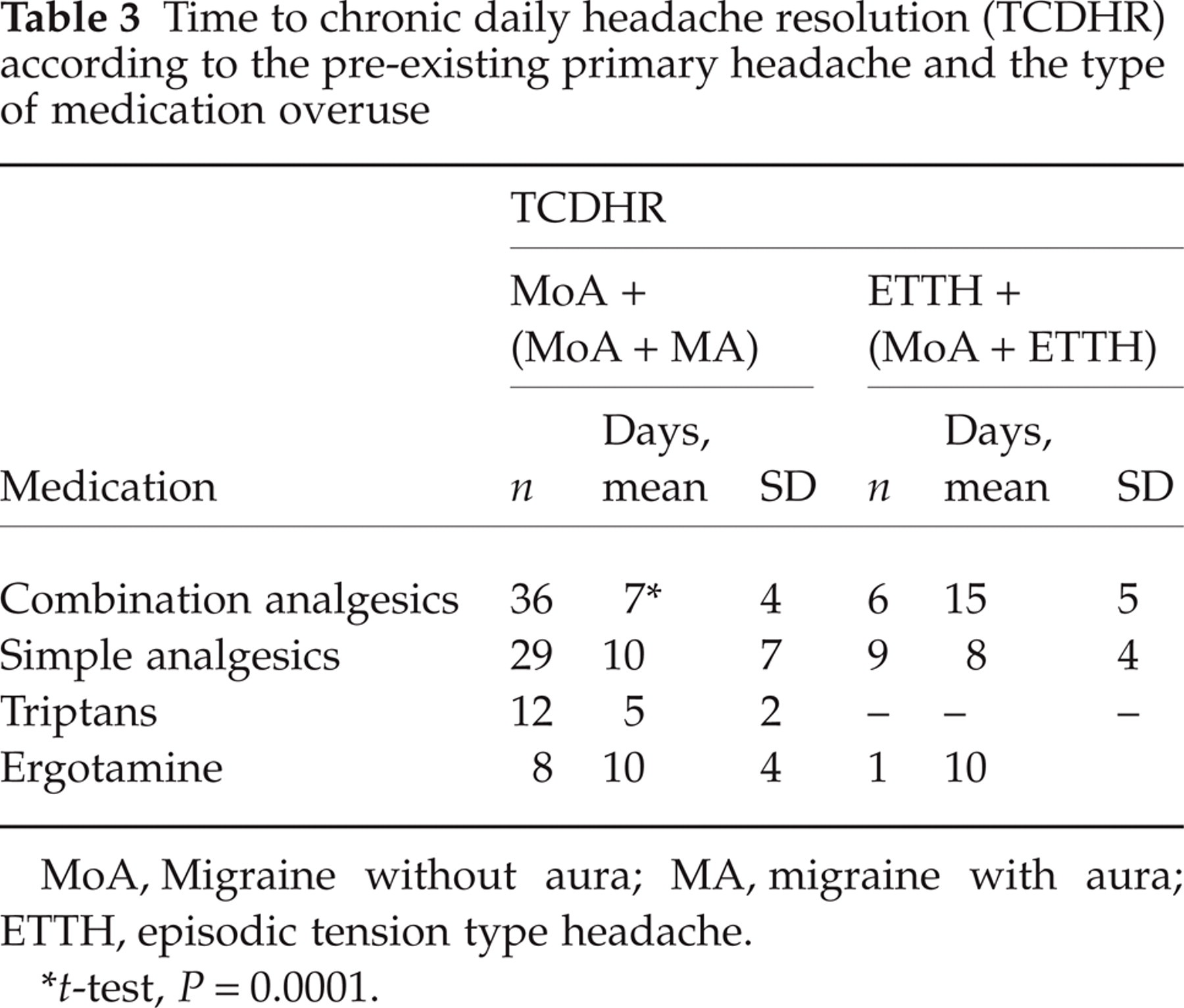
MoA, Migraine without aura; MA, migraine with aura; ETTH, episodic tension type headache.
t-test, P = 0.0001.
We did not find any correlation between TCDHR and duration of daily abuse when the whole sample of patients was analysed (Pearson correlation = 0.14, P = NS), whereas dividing patients according to the medication overused, a significant, albeit weak, direct correlation was found in simple analgesics abusers (Pearson correlation = 0.33, P = 0.043). A direct correlation was observed between TCDHR and DDI, both taking the patients as a whole (Pearson correlation = 0.25, P = 0.01) and combination analgesics abusers, when the patients were stratified according to medication overused (Pearson correlation = 0.41, P = 0.007).
In stepwise linear multiple regression, TCDHR was independently associated with DDI (P = 0.03), age (P = 0.044), and the type of medication overused (P = 0.045).
At 3-month follow-up no patient was suffering from CDH and nobody was overusing analgesics. All patients had reverted to their former primary headache with a mean rate of four (SD 2) attacks per month.
Discussion
MOH is a frequent and problematic medical condition, often difficult to manage owing to the long duration of CDH, development of withdrawal symptoms, occurrence of rebound headache, psychiatric comorbidity, psychological and physical dependence, low motivation and, consequently, poor compliance.
Withdrawal therapy is the mainstay of treatment in both the out-patient and in-patient settings. The use of i.v. DHE coadministered with metoclopramide was proven to be safe and effective in rapidly controlling intractable headache. Silberstein et al. (7) treated 214 patients affected by daily headache with rebound by means of the i.v. DHE protocol originally introduced by Raskin (6). Over 90% became headache free within 2–3 days with a mean length of stay in hospital of 7.3 days. In refractory patients i.v. neuroleptics such as chlorpromazine, droperidol and prochlorperazine, and/or corticosteroids were used to supplement i.v. DHE therapy. On a follow-up evaluation of 50 patients with CDH and drug overuse treated with repetitive i.v. DHE, most patients did not relapse after discharge, and at least 70% continued to show improvement at 2 years (24).
In a retrospective study of 174 patients with CDH and SM overuse admitted for the i.v. DHE treatment protocol during a brief (usually 48 h) in-patient stay, 132 were interviewed by phone and 56% showed a positive outcome at 3 months (8).
A short course of oral prednisone in tapering doses during 6 days, followed by the introduction of preventive treatment, was used in an out-patient setting in 400 patients with CDH due to medication overuse (9). Eighty-five percent of patients reported a reduction in headache frequency and no patient complained of severe rebound headache during the first 6 days. After 1 month, a significant decrease in headache frequency was observed and no patient had resumed drug overuse.
In a 3-year follow-up prospective study, 61 patients with transformed migraine and analgesic overuse were treated either with in-patient pharmacological therapy alone or with in-patient pharmacological therapy combined with biofeedback-assisted relaxation (11). The results of the study suggested that the combination of behavioural and pharmacological treatment was more effective than pharmacological treatment alone in the long term.
A retrospective study of 71 patients admitted for treatment of CDH with analgesic abuse demonstrated that i.v. lignocaine (lidocaine) infusion for an average of 8.7 days was useful in controlling rebound headache and that the benefits lasted for at least 6 months (13).
In an out-patient setting, Krymchantowski and Moreira (14) performed a prospective randomized open-label trial in 150 patients with chronic migraine and overuse of SM. All patients received education and orientation and were then abruptly withdrawn from all SM. After withdrawal, for the initial 6 days, 50 patients took oral prednisone (60 mg/day on days 1 and 2, 40 mg/day on days 3 and 4, 20 mg/day on days 5 and 6), 50 patients took naratriptan (2.5 mg b.i.d.), and 50 patients did not receive any regular medication. After 5 weeks, there were no differences between the three groups of treatment with regard to treatment adherence, headache frequency and severity, or number of days with headache, but the incidence of withdrawal symptoms and the consumption of rescue medication were higher among patients who did not take regular medication during the first 6 days. The authors concluded that patients with chronic migraine and moderate overuse of symptomatic drugs other than opioids may be detoxified on an out-patient basis regardless of the therapeutic strategy adopted, but also that prednisone and naratriptan may be useful for reducing withdrawal symptoms and rescue medication consumption.
For all patients who met the inclusion/exclusion criteria in the present study, hospitalization to follow a detoxification protocol was proposed. The patients who accepted were treated on an in-patient basis, to minimize withdrawal symptoms, for better control of pain, to establish an effective preventive treatment, and to ensure continuous support to patients and patient education, in agreement with many studies which report a good outcome with an in-patient withdrawal therapy (8, 10, 11, 17, 19, 20, 23–26). The Italian National Health Organization meets the hospitalization expenditure when detoxification from drug overuse is needed.
Since the patients were monitored frequently and therefore safely and adequately treated, even those who overused butalbital-containing analgesic combinations [6.9%, with a mean daily dosage of 271 (SD 211) mg], abruptly discontinued the overused drug.
The in-patient withdrawal protocol used in this study was effective, safe and well tolerated. The administration of rescue medications, though moderate and brief, was necessary in 72% of patients. No patient was treated with DHE, steroids or neuroleptics, as previously proposed (6, 7, 9, 10, 14).
In this sample of patients the pre-existing primary headache was MoA or MoA plus MA in more than 80% of patients (84.2%), at variance with that reported in other studies where migraine was slightly less common and ETTH much more frequent (19, 21, 27–29).
Taking the patients as a whole, mean TCDHR was 8 (SD 5) days, much shorter than the time limit established by the IHS Diagnostic Criteria for MOH (1), which state that the headache resolves or reverts to its previous pattern within 2 months after the discontinuation of the overused medication.
We observed a trend for a shorter TCDHR in patients who abused triptans (P = 0.062). This result may indicate a better outcome in these abusers, but, on the other hand, triptan abusers showed also the shortest duration of daily abuse and the lowest DDI, suggesting the possibility that triptans may induce MOH faster and at lower DDI, as previously reported (20).
TCDHR was not correlated with the initial primary headache when the entire population was analysed, but, when the study patients were stratified according to the medication overused, migraineurs who abused combination analgesics had significantly shorter TCDHR than patients who suffered from ETTH or ETTH plus MoA (P < 0.0001). TCDHR was independent of duration of daily abuse when patients who overused combination analgesics, simple analgesics, triptans or ergotamine were analysed all together, but, dividing them according to the overused medication, we found a direct correlation in simple analgesics abusers (P = 0.043). TCDHR was related to DDI (P = 0.01) in the whole group, and particularly in combination analgesics abusers (P = 0.007). It is worth mentioning that all combination analgesics medications contained caffeine with a mean daily dosage of 218 (SD 188) mg. The repetitive daily use of caffeine may have played a negative role in the outcome of MOH patients, especially in those who were originally suffering from ETTH or ETTH plus MoA.
Multiple regression analysis demonstrated that DDI, age and the type of medication overused were independent predictors of TCDHR. Therefore, it seems advisable to recommend a limitation in the daily use of SM, especially triptans, in patients with CDH.
At 3 months’ follow-up, no patient had relapsed and was again overusing SM, and the headache had reverted to its previous pattern in all patients.
The follow-up is clearly too short to draw firm conclusions on the long-term efficacy of the withdrawal therapy protocol used in the present study. Nevertheless, the results of this study show that all patients with CDH and medication overuse, including those with long-term duration of daily abuse and high DDI, may safely benefit from abrupt discontinuation of the overused medication with a reasonable length of admission.
Footnotes
Acknowledgements
The study has been supported by a grant of the University of Trieste, Italy Murst 60%.