
Abstract
Introduction
The International Classification of Headache Disorders 3rd edition beta (ICHD-3 beta) gave alternative diagnostic criteria for 1.2 migraine with aura (MA) and 1.2.1 migraine with typical aura (MTA) in the appendix. The latter were presumed to better differentiate transient ischemic attacks (TIA) from MA. The aim of the present study was to field test that.
Methods
Soon after admission, a neurologist interviewed 120 consecutive patients diagnosed with TIA after MRI or CT. Semi-structured interview forms addressed all details of the TIA episode and all information necessary to apply the ICHD-3beta diagnostic criteria for 1.2, 1.2.1, A1.2 and A1.2.1.
Results
Requiring at least one identical previous attack, the main body and the appendix criteria performed almost equally well. But requiring only one attack, more than a quarter of TIA patients also fulfilled the main body criteria for 1.2. Specificity was as follows for one attack: 1.2: 0.73, A1.2: 0.91, 1.2.1: 0.88 and A1.2.1: 1.0. Sensitivity when tested against ICHD-2 criteria were 100% for the main body criteria (because they were unchanged), 96% for A1.2 and 94% for A1.2.1.
Conclusion
The appendix criteria performed much better than the main body criteria for 1.2 MA and 1.2.1 MTA when diagnosing one attack (probable MA). We recommend that the appendix criteria should replace the main body criteria in the ICHD-3.
Keywords
Introduction
The classification committee working on the International Classification of Headache Disorders 3rd edition beta (ICHD-3beta) realised that the criteria for migraine with aura (1.2 and 1.2.1) might pose a problem in relation to the differential diagnosis against transient ischemic attacks (TIA). For that reason, an alternative set of diagnostic criteria for migraine with aura 1.2 (MA) and for migraine with typical aura 1.2.1 (MTA) were developed based on expert opinion and published in the appendix (A 1.2 and A 1.2.1) (1). Although the supplemental diagnostic criteria were specifically designed to discriminate better between MA and TIA, they have never been field tested against a prospectively collected and directly interviewed material of TIA patients. In the present study we used a prospectively, consecutively collected material of patients diagnosed with TIA according to existing definitions. Patients also received an extensive neurologist conducted interview about their former headaches and about any headache or aura-like symptoms that might have occurred at the time of the TIA. The aim was thus to field test the appendix criteria as well as the main body criteria for migraine with aura against this material of patients with TIA. We hypothesised that the appendix criteria would fare better and therefore might be preferred for the forthcoming final version of the third edition of the international headache classification (ICHD-3).
Materials and methods
Study design
This was a cross-sectional study, which was conducted between September 2013 and May 2016.
Study population
Patients were eligible for enrollment if they had had a transient ischemic attack (TIA) within the 14 days before admission at the stroke unit of the New Hospital city hospital in Yekaterinburg, Russia. Eligible patients had focal brain or retinal ischemia with resolution of symptoms without presence of new infarction on MRI or CT. All patients were evaluated within one day of admission, usually within a few hours by a neurologist.
We consecutively included patients with TIA who agreed to be interviewed. The reasons for exclusion were: Previous stroke, subarachnoid haemorrhage, intracranial aneurysm, intracranial haemorrhage, brain tumour, any operation on the brain, multiple sclerosis, epilepsy, encephalitis, meningitis, dementia or memory problems, speech problems and other serious neurological or somatic disorder. A total of 131 patients were examined, 11 patients were excluded and 120 were included in the study.
Evaluation
One neurologist (NMG) collected patient data prospectively, using a standardised case-report form, during face-to-face interviews at the time of evaluation of the TIA after MRI or CT. MRI with DWI scans was performed in 112 patients with TIA and CT in eight patients. Sociodemographic characteristics of patients, medical history, clinical symptoms during TIA risk factors, past history of headache and headache around the time of TIA were recorded. Results of imaging and laboratory tests were also recorded in the case-report form as well as previous and current treatment. Two neurologists (ERL and NMG) performed a detailed interview about TIA versus MA. The interview form is presented in the supplementary material, Table 1.
Definitions and diagnostic criteria
Diagnostic criteria of ICHD-3beta and appendix for 1.2 and 1.2.1.

Neurologists (NMG and ERL) also performed telephone interviews in difficult cases when we suspected that patients could have migraine with aura instead of TIA. This interview was undertaken 1–3 years after the first interview. Patients were asked about recurrent similar episodes, their characteristics and some other information about risk factors and headache was verified too.
Ethical considerations
The Medical Ethics Committee of the Urals State Medical University approved this study. All respondents were informed of the purpose of the survey. Written informed consent was obtained from all participants.
Statistical analysis
All 120 patients with TIA included in this study were submitted to testing of the criteria for 1.2 Migraine with aura, A1.2 Migraine with aura (alternative criteria), 1.2.1 Migraine with typical aura and A1.2.1 Migraine with typical aura (alternative criteria) in ICHD-3 beta. The number of patients fulfilling each criterion was recorded. The specificity of the four different sets of criteria was calculated as 120 minus the number with false positive diagnosis (fulfilling a set of criteria for MA) divided by 120. We likewise tested the sensitivity of the two sets of criteria in 1157 patients from a previous publication diagnosed with one of the subtypes of MA according to ICHD-2 (as this classification did not have criteria for 1.2 MA) (3).
Results
Distribution of patients with TIA by age and sex.

Sociodemographic characteristics of patients with TIA.

Fulfillment of diagnostic criteria for migraine with aura in patients with TIA
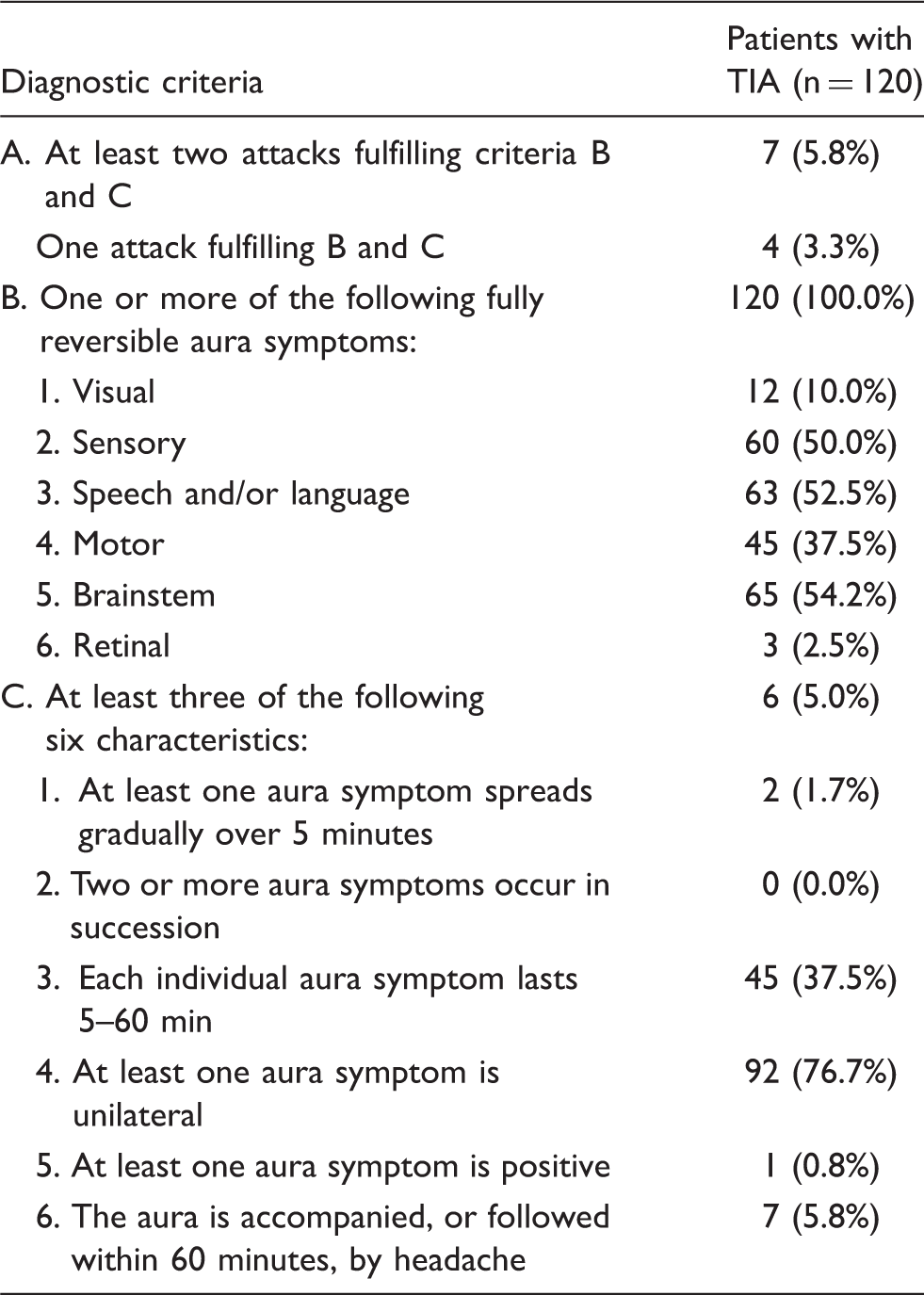
Distribution of patients with TIA according to diagnostic criteria of 1.2 Migraine with aura.

Distribution of patients with TIA according to diagnostic criteria of 1.2.1 Migraine with typical aura.

Distribution of patients with TIA according to diagnostic criteria of A1.2 Migraine with aura (alternative criteria).
Distribution of patients with TIA according to diagnostic criteria of A1.2.1 Migraine with typical aura (alternative criteria).

It is important to also be able to distinguish MA from TIA at the first ever attack of MA, a common problem in the emergency room of hospitals with a neurological department and a stroke unit. Requiring at least one attack, the main body criteria for 1.2 were fulfilled by 32 out of 120 TIA patients, specificity 0.73. The appendix criteria performed much better, with 11 patients fulfilling A 1.2 at a specificity of 0.91. In the main body 1.2.1 was fulfilled by 15 patients, specificity 0.88, and the appendix criteria by 0 patients, specificity 1.0.
For the patients fulfilling MA criteria, we tried to apply criterion D: Not better accounted for by another ICHD-3beta diagnosis. In this case, we tried to see if patients with TIA also fulfilling MA criteria had other reasons to prefer the TIA diagnosis. This proved difficult, however, because imaging according to the definition of TIA was required to be normal. Risk factors for TIA, family history of stroke or migraine and age of patients, are difficult to use because there is no absolute difference between TIA and migraine. We re-interviewed all 11 patients who fulfilled the appendix criteria. None had had an identical episode after the TIA. Thus it seems likely that the patients with TIA who fulfilled the criteria for MA really had had a TIA.
We used 1157 patients from a previous publication (3) to test the specificity of the main body and appendix criteria. They were all diagnosed with one of the subforms of MA, as ICHD-2 did not have diagnostic criteria for 1.2 migraine with aura. The criterion C in the ICHD-3beta main body was essentially unchanged compared to ICHD 2. Therefore the sensitivity of the main body criteria was 100% for both 1.2 and 1.2.1. The criteria in the appendix were changed, but nevertheless sensitivity against ICHD-2 diagnosis was 96% for A1.2 and 94% for A1.2.1
Discussion
The main result of the present study was that the diagnostic criteria for migraine with aura (1.2) and migraine with typical aura (1.2.1) in the main body of ICHD-3beta had lower specificity than the appendix criteria when tested against a large, prospectively studied material of patients with TIA. Since sensitivity tested against a migraine material was excellent, the appendix criteria are preferable.
The reason why the main body criteria performed relatively poorly is that criterion B is fulfilled by all patients with TIA, so that only criterion C has distinguishing power. It requires two or more out of the following subcriteria: Gradual spread or symptoms occurring in succession, duration 5–60 minutes, closely related headache, half-sided symptoms. It is obvious that many TIA patients have symptoms lasting 5–60 minutes and symptoms are almost always unilateral. Such patients fulfill the diagnostic criteria for one MA attack i.e. for probable MA. The same applies to migraine with typical aura, but here almost half of the TIA patients do not fulfill criterion B because it rules out motor symptoms. The appendix criteria for 1.2 have the same criterion B, which is fulfilled by all TIA patients, but criterion C is different, requiring at least three out of the following: Gradual spread, symptoms occur in succession, duration 5–60 minutes, half-sidedness, at least one positive symptom closely related to headache. While a lot of patients exhibit a duration of 5–60 minutes and unilaterality, very few of these fulfill any of the other symptoms. Slow spread of symptoms and succession of symptoms were the best discriminating features. Therefore, criterion C distinguishes accurately between MA and TIA. Precisely the same applies to A 1.2.1.
It might be argued that specificity becomes quite good for the main body if at least two identical attacks are required. It is important, however, that the criteria are able to distinguish MA and TIA even if only one attack has been present. These are patients who may be having their first ever attack of MA or patients who have a new feature different from their previous attacks who need to be re-diagnosed. The problem is not trivial. Up to about 20% of patients with suspected TIA have migraine aura (4,5). In the neurological department at Rigshospitalet-Glostrup, Copenhagen, Denmark, the differential diagnosis between MA and TIA in patients with their first attack or with attacks presenting new symptomatology has to be made at least once a week. Misdiagnosis of MA as TIA has grave consequences. It leads to an unnecessarily extensive work up, but more importantly, it is serious to give a patient a TIA diagnosis. It leads to lifelong antiplatelet therapy, with a risk of bleeding, and it scares patients who know that a TIA is often followed by a stroke. It also has severe implications in relation to health insurance and sometimes in relation to job opportunities. Conversely, it is perhaps even more serious if a TIA patient receives a diagnosis of MA, which would happen often if the main body criteria were applied to the letter. Necessary work up would not be performed, prophylactic treatment would not be given and life style changes would not be encouraged. This might lead to a stroke that could have been avoided.
Should the appendix criteria then replace the current criteria in the main body of the classification? Before answering that, it is important to also look at the sensitivity of the two sets of criteria. This is, however, a difficult issue. It can only be done by comparing with migraine patients diagnosed according to ICHD-2 diagnostic criteria, which are not a gold standard but the best criteria available in 2004. Any change of such criteria will always result in a sensitivity of less than 100%. This is illustrated by our findings. The sensitivity of the main body ICHD-3beta criteria for 1.2 and 1.2.1 was 100% because they were essentially unchanged. For the appendix criteria, the sensitivity was 96% for A1.2 and 94% for A1.2.1, because the criteria were changed. The appendix criteria thus achieve much better separation from TIA with no compromise of sensitivity. Most of the reasons to prefer the appendix criteria have just been presented above, but there is a more general reason. The virtue of the ICHD classifications is that diagnostic criteria are explicit and invite field testing. When appropriate field testing is done, the results should also be implemented in the classification. Where would we be otherwise? Nobody would wish to field test anything in the future. This is the opposite situation to proposals to change the classification based on feelings and ideas in the absence of new data. The classification should not be changed because of the latter, but it is equally wrong not to change when good field testing suggests it.
One limitation of this study is the quick disappearance of clinical symptoms in TIA patients before admission to hospital. Some of the patients could not remember details that are important in the differential diagnosis of TIA and MA. For example, some patients could have missed the gradual spread of symptoms or presence of a succession of symptoms. Some patients could not describe the characteristics of the headache during TIA very well. Therefore, some cases of MA could have been missed. One might also argue that 120 TIA patients is not a large material. It is, however, very demanding to prospectively interview patients in the acute phase after TIA using a neurologist-conducted semi-structured interview about both the previous and actual headache history and about the characteristics of the cerebrovascular event. Replication of these results would of course be important, but is not customary in field test studies due to the lack of resources. This type of research is usually very difficult to fund, unlike, for example, genetic studies. On the positive side, this study was done with the best possible methodology, using specifically designed extensive semi-structured interview forms. Also the fact that it was undertaken by fully trained neurologists in the acute phase after admission was a strength of the study.
Conclusions
Thorough field testing of the criteria for migraine with aura and migraine with typical aura have shown that the criteria in the main body have poor specificity in distinguishing one attack of migraine with aura from a transient ischemic attack. The criteria in the appendix perform better, and we suggest replacing the main body criteria with the appendix criteria.
Clinical implications
Differential diagnosis between migraine with aura and transient ischemic attacks is a common problem in the emergency room. It is important to make the diagnosis based on the symptoms of the patients. Therefore, the explicit diagnostic criteria for migraine with aura and its subforms are very important. We show that the appendix criteria of the International Classification of Headache Disorders 3rd edition beta differentiate excellently between these disorders.
Footnotes
Acknowledgement
We gratefully acknowledge the following doctors who participated in this study: Tsypushkina TS and Filimonova PA.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.