
Abstract
Abstract
New daily persistent headache is described as an enigmatic condition with daily headache from onset. It has posed challenges diagnostically and therapeutically.
Keywords
Introduction
In 1986 Vanast reported on a new onset headache, daily from onset, with only 30% of his 45-patient cohort experiencing spontaneous resolution by three months (1). Fifty-three percent experienced nausea, 13% vomiting, 33% sensitivity to light and 40% to noise; 18% experienced additional episodes of vertigo. Age of onset ranged from 16–45 years, younger in females. Based upon this cohort, in the second (2004) International Classification of Headache Disorders (ICHD) New daily persistent headache (NDPH) was included in Part I: The Primary Headaches. The definition was of headache present for at least three months, daily and unremitting within three days of onset. The defined clinical syndrome that of tension-type headache.
Since that time there have been published cohorts in the paediatric population (2,3) and adults (Table 1) which show many patients clearly have additional migrainous features. In acknowledgement the 2018 classification redefined NDPH to a headache unremitting within 24 hours, with clear recollection of onset and without defined clinical syndrome (Table 2) (4).
Published Cohorts of New Daily Persistent Headache.

Abbreviations: ICHD-2 – International Classification of Headache Disorders, 2nd edition. ICHD-2R - Revised ICHD-2 criteria. ICHD-3 – 3rd edition. CTTH – Chronic Tension-Type Headache. TTH – Tension-Type Headache.
Treatments tried in the management of the New Daily Persistent Headache and responses.

1. One patient was lost to follow-up.
2. Three patients found the drug was helpful for headache, but they had severe side effects at doses of 50, 100 and 375 mg daily respectively. One patient stopped the medication because she became pregnant.
One patient benefited from the drug at the dosage of 2400 mg/daily but effectiveness was not maintained.
NDPH accounts for 1.7–10.8% tertiary clinic presentations in adults (5–7) and 13–36% in children and adolescents (2,3,8). Two sub-forms are recognised, a persistent intractable form and a self-limiting, sometimes relapsing and remitting form (9). Between 16 and 66% of patients enter remission without treatment. Although some patients report a trigger to the onset, the majority occur spontaneously. The disorder is notable for its resistance to treatment (10). The largest population-based study found the prevalence of NDPH to be 0.03% (11). This is in contrast to all chronic daily headache (CDH) which has a population prevalence of about 4% (12). The CDH population is largely comprised of patients with chronic tension-type headche (CTTH) and chronic migraine (CM), with about 1% overusing acute-relief medication. Over the years there has been debate about what is NDPH; is it a novel syndrome and thus disorder, does it have specific triggers, are these triggers more relevant to understand than the headache, how important is the clear recollection of the exact time of onset, now included in the ICHD and, how should these patients be managed (13)? The revised criteria are broader and accommodate a wider spectrum of syndromes. However, the diagnosis and management remain somewhat enigmatic and challenging for the practicing neurologist.
Apart from migraine and tension-type headache, most other primary and secondary headaches, with new daily persistent onset, are already accommodated elsewhere in the classification. If primary, they are classified according to syndrome and if secondary according to precipitating pathology. We report on an observational cohort of patients with NDPH to ascertain whether there is a distinct phenotype or whether NDPH would better serve as a mode of onset.
Methods
A retrospective study was carried out of 162 adult patients presenting with ICHD-3 defined NDPH to a headache specialist service based in Central and North-East London between 2005–2015. Medical records were reviewed to document: age, gender, age of onset, prior history of headache, family history of headache, possible antecedent triggers, treatments and responses, relevant test results, medical and psychiatric comorbidities, Headache Index Disability (HIT-6) and Hospital Anxiety and Depression scores (HAD), where available. In addition to the ICHD-3 diagnosis of NDPH, the ongoing daily headache was also phenotyped to see what proportion of symptoms were consistent with ICHD-3 criteria for migraine, tension-type headache or any other cohesive syndrome. This patient group was clearly differentiated from those with episodic headache rapidly evolving to daily.
Patients with ICHD-3 defined acute-relief medication-overuse were advised to restrict intake to maximum eight days per month (14). Those with persistent daily headache, at least six months later, were included in the cohort. Response to preventative treatment was assessed in the absence of acute-relief medication overuse. Patients were asked to keep a headache diary. which was used to monitor disability and correlated with the HIT-6 score.
Statistical analysis
Data was tabulated and statistical analysis performed using Excel (Microsoft). Quantitative data were expressed as mean ± standard deviation (SD) when normally distributed. When non-parametric the median value and the inter-quartile range (IQR) was used.
In line with guidelines of the Health Research Authority (http://www.hra-decisiontools.org.uk/research/) the work was registered as service evaluation with the Clinical Effectiveness and Information Governance departments at each respective hospital.
Data availability
The data that support the findings of this study are available from the corresponding author, upon reasonable request.
Results
Demographics
The median onset age was 35 +/− 23 years, later in men than women (Figure 1). The male to female ratio was 1: 2.18 (51/111).

The distribution of age onset of NDPH in males and females.
Triggers
There was no obvious precipitating factor in 142 (85%). A ‘flu-like illness or other infective event was reported in 11 patients (7%) and a stressful life event in five (3%). Infrequent precipitants included systemic illness and pregnancy.
Clinical syndrome
Within this cohort, 136 patients experienced a single headache syndrome, most commonly CM in 122 (90%). Of the CM group 84 (62%) patients experienced aura (Figure 2). The proportion of other types of headache syndromes is shown in Figure 3.
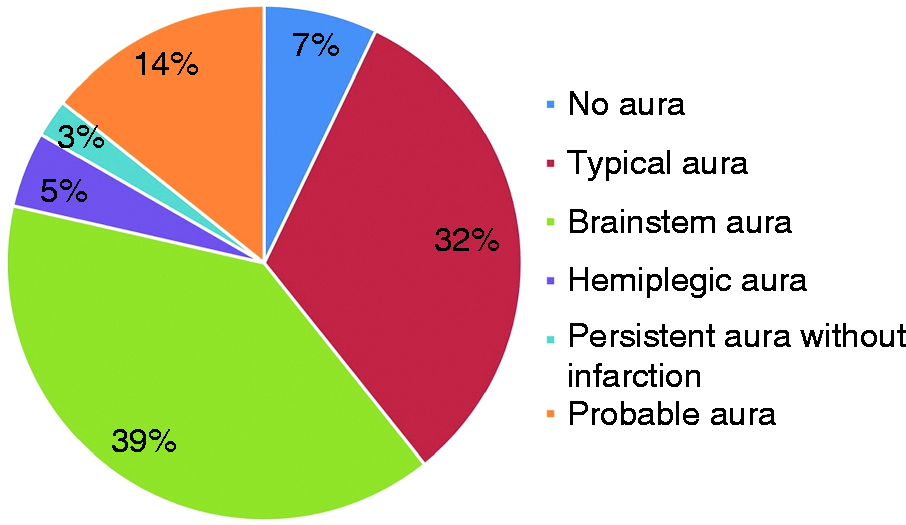
Distribution of aura symptoms in patients with NDPH and clinical syndrome daily headache consistent with chronic migraine (N = 84).
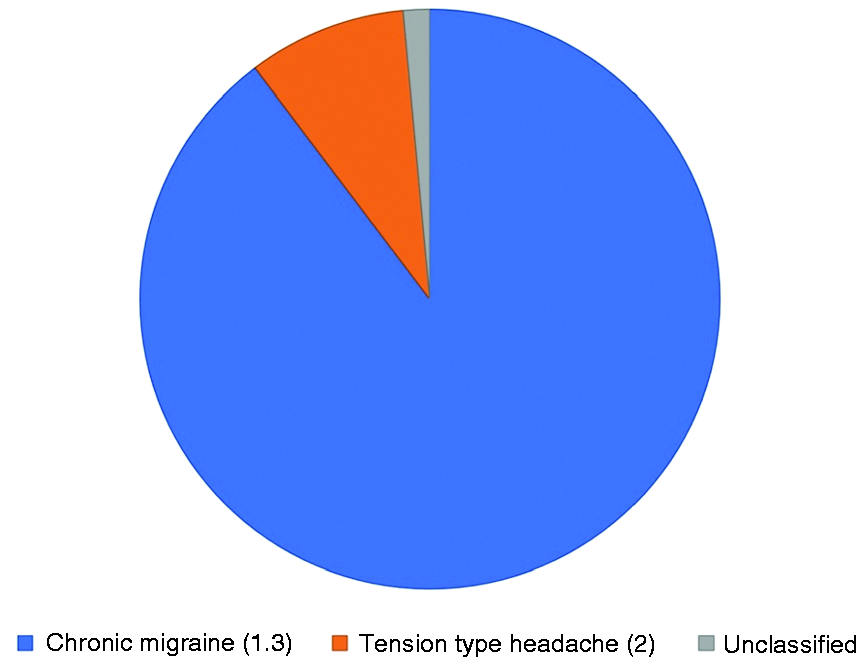
Proportion of patients with a single headache syndrome.
More than one headache syndrome was experienced in 25 (15%) patients. Twenty-two of this group presented with two headache syndromes; 21 had a diagnosis of chronic migraine and another headache phenotype, 13 with episodes of stabbing headache, 6 with thunderclap headache and once each with cough headache and headache associated with sexual activity. Only one patient had a combination of a tension type headache and hypnic headache.
Three patients suffered with three headache syndromes: chronic migraine and episodes of stabbing headache, in addition one each with exertional headache, thunderclap headache and cough headache.
Only 1.5% of patients could not be classified according to any syndrome (consistent with 14.1 of the ICHD-3).
Thunderclap Headache
Twenty-four patients (15%) had thunderclap headache at onset. One patient of this group reported a ‘flu-like precipitant. Incidental abnormalities were detected on imaging (CT or MRI) in seven patients; three had non-specific white matter lesions, one an arachnoid cyst, an asymptomatic undefined cystic lesion (right hemisphere and mid-brain), chronic small vessel disease, Arnold Chiari malformation (I) and “bulge” of the left anterior communicating artery but subsequent normal magntic resonance angiography (MRA).
Following the thunderclap headache, the subsequent persistent headache syndrome was similar to the NPDH group overall. Of 15 patients who had a single headache phenotype 13 had chronic migraine (87%) and two had tension type headache (13%). Seven patients suffered two headache syndromes: six had a diagnosis of chronic migraine and episodes of recurrent thunderclap headache and one patient had CM and episodes of stabbing headache. Two patients had three headache syndromes: CM, primary stabbing headache and, one with a cough headache, the other with recurrent thunderclap headache. Overall, seven (29%) patients developed episodes of recurrent thunderclap headache following the initial thunderclap onset.
Sub-forms of headache
Eighty-three (51%) patients had a persisting sub-form of NDPH, 20 (12%) had a relapsing and remitting course and 23 (14%) reported improvement. Thirty-two (20%) patients did not attend further follow-up. Four patients reported complete resolution of symptoms: one of these patients after five years with prior good response to nortriptyline. The time duration between remitting and relapsing episodes varied, from two months to eight years of remission.
Past and family history of headache
Full dataset about past history of headache was available in 74 patients (46%). Two (3%) developed NDPH with a syndrome which could not be defined within the ICHD, one with a past history of migraine and one with a 9-month episode of cervicogenic headache precipitated by cervical manipulation. In 72 (97%) the NDPH had a headache phenotype consistent with chronic migraine and in one with chronic tension-type headache. In these 72 patients 71 had previously suffered an episodic headache syndrome. One had a history of daily but intermittent headache with pain free time and no change in pattern over 10 years nor acute-relief medication overuse; this patient hence developed daily persistent headache without pain-free time. Thirty-seven (51%) had the same headache syndrome in the past, 11 with migraine with aura in whom three had persistent aura coinciding with the NDPH and 26 without aura. Seven (10%) with a past history of migraine with aura developed daily migraine without aura, while six (8%) without a past history of aura developed episodes of aura with the NDPH. A further three patients (4%) developed a different aura to that previously experienced. In none of the patients was there an increase in headache frequency prior to the development of the NDPH. In all but three headache frequency was less than 8 days a month or in remission (defined as at least one or more years without headache). Only three had previously tried a preventative none of which had been effective in the past. One retried preventative treatment without any meaningful response. Seven (10%) developed a different headache syndrome with their NDPH than previously and 12 (17%) described non-specific headache (ICHD 14.2) where the patient could not recall the details, suffice to say that attacks had been non-disabling and settled readily with simple analgesics.
A family history of headache in a first-degree relative was noted in 41 (25%) of patients.
Medical co-morbidities
Forty-two patients presented with a pre-existing medical co-morbidity with mental health disorders being the most common in 15 patients (36%), followed by hypothyroidism in nine (6%), hypertension in six (14%) and asthma in five (12%).
Disability
Ninety-six patients had completed a HIT ± HAD questionnaire at their first visit. The mean score for HIT at the early stage of treatment was 66.4 +/− 0.7. The mean scores of HAD-A and HAD-D were 9.6 +/− 0.5 and 8.1+/− 0.5 respectively. The most prevalent psychiatric conditions were anxiety and depression. A proportion of patients had matched disability scores recorded on both their initial visit and final visits, attesting to intractability of medical treatment.
Investigations
A total of 145 (90%) patients underwent neuroimaging, either or both MRI and CT head. An MRI brain was done in 136 (84%) patients, and 56 of these patients had MRI with gadolinium. Thirteen patients had a CT head and nine as their only modality of imaging.
Ninety-four (69%) patients had a normal MRI head without contrast. Of those who had MRI with contrast, 38 (68%) were normal. All abnormalities were considered incidental. Non-specific white matter lesions were the most common in 18 patients. The other abnormalities include Arnold Chiari I malformations, spina bifida, mild tonsillar herniation, pineal cysts, arachnoid cysts, other benign cystic lesions, ischaemic lesions, arterio-venous malformations, a developmental cerebellar venous anomaly, a stable left parietal tumour, cerebral atrophy, sinus disease and minimal pachymeningeal enhancement without dural thickening associated with some ventricular dilatation and hypointense foci in the white matter. The latter patient had presented previously with thunderclap headache and found to have subarachnoid haemorrhage from rupture of a right posterior communicating artery aneurysm. Following successful endovascular coiling the associated headaches resolved after 4 weeks following which she was pain free. There was no evidence of recurrence until she presented with new daily persistent four years later. Repeat imaging was unchanged from that done previously.
Of 9 patients who underwent CT head only, one patient had an abnormal finding, an incidental subtle hyperdensity in the inferior cerebellum.
Cerebrospinal fluid (CSF) was measured in 31 patients. Only one patient had an abnormality, elevated red cell count with no xanthochromia. Twenty-two patients had CSF pressures recorded, the mean was 18.6 +/− 1.4 cmH20.
Treatment
Medication overuse
Patients with ongoing medication overuse in addition to symptoms fitting criteria of possible NDPH were excluded from the analysis. Some patients were able to successfully undergo acute-relief medication withdrawal. Twenty-nine patients met the criteria for medication overuse; of these only 10 (35%) were able to restrict their medication use with five patients improving, one feeling worse and four reporting no difference. The remaining patients did not re-present to clinic.
Of those who improved was a 59-year-old man who presented with a 20-year history of new onset daily persistent headache, with clinical syndrome consistent with CM. He had been on Tramadol since onset, taken for joint pain. Following withdrawal his headache disorder became episodic. Moreover, he reported a reduction in severity after starting preventative treatment (Figure 4). There was no clear trigger to the onset of the daily pain.
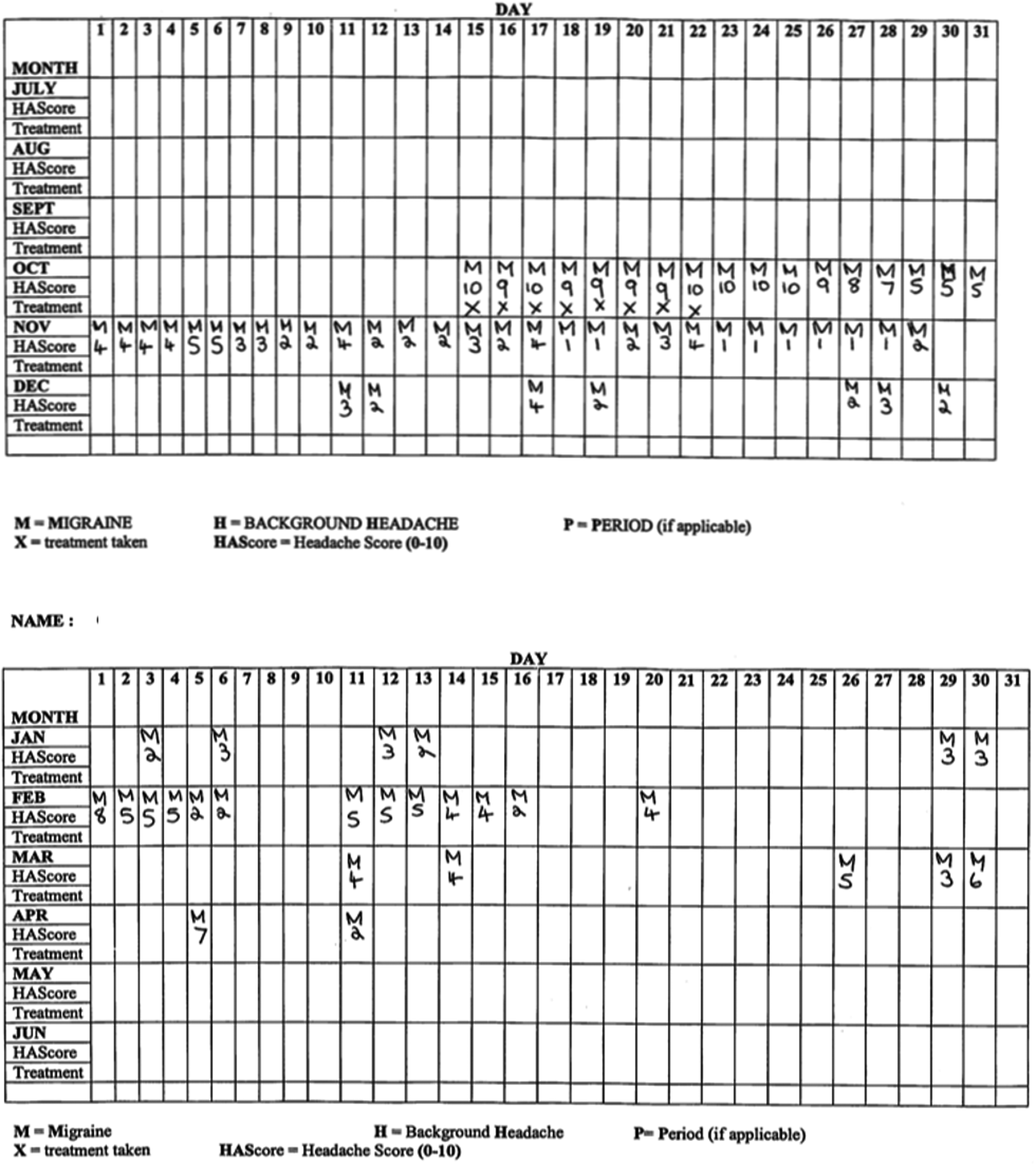
Daily headache diary of 59-year-old man with a 20-year history of NDPH associated with opioid overuse from onset.
Oral preventatives
All patients received treatment in the absence of medication overuse. This included oral pharmaceutical agents, intravenous dihydroergotamine, peripheral nerve blocks and peripheral nerve stimulation. Most patients tried two or more preventative drugs. The percentage of patients who received each of these drugs and their corresponding responses are listed in Table 2. One patient trialled theophylline 800 mg daily dose (empirically for possible low CSF volume headache) and two pregabalin with meaningful response.
One patient tried indomethacin for recurrent thunderclap headache with reduced frequency of attacks but not resolution. One patient with stabbing headache responded to indomethacin while two did not. One patient with sexual headache did not find pre-emptive indomethacin effective.
Intravenous dihydroergotamine
Thirty patients (20%) received intravenous dihydroergotamine; three had dose-dependent side effects thus treatment was discontinued. Ten (33%) described improvement after the first treatment, with a median duration of effect of 4 weeks (range 1 to 20 weeks). Seven patients continued to have a second course, with four reporting benefit with median duration of effect 8 weeks (range 2 to 8 weeks). One patient had five courses of dihydroergotamine (DHE) with effect duration varying from two to 13 weeks.
Greater occipital nerve blocks
Seventy-two patients received greater occipital nerve (GON) blocks. Most patients had a combination of 2% lidocaine and 80mg of methylprednisolone. After the first injection, 28 (39%) patients reported benefit with 21 (13%) having a documented duration, median of 3 weeks (range 1 to 24 weeks). Thirty patients (42%) had no benefit with fourteen reporting they felt worse following the injection. One patient had 2% lidocaine only and failed to gain any benefit.
Thirty-three (46%) patients had multiple GON blocks, with two patients on regular cycles of injections. Excluding those on regular injection cycles, after their second injection fifteen patients reported some benefit, with fifteen having no effect and three feeling worse. Twelve of this group with benefit had recorded durations of benefit, median of 4 weeks (range 1 to 20 weeks). Ten patients had a third GON block, with six reporting benefit (median 8.5 weeks, range 2 to 24 weeks) and four no benefit. Six patients had a fourth injection, four reporting benefit and two without. Two with benefit had documented durations of effect, 4 and 6 weeks.
Of the two patients on a regular GON injection cycle, the first patient received three to six monthly injections over a four-year period, with a variable response to treatment up to two weeks of benefit. The second received biannual to yearly injections over 6 years with consistently meaningful effect.
Supraorbital nerve block
One patient received a supraorbital nerve (SON) block, in combination with GON block. This patient had a good response to a SON block being pain free for two years; the second injection provided greater therapeutic benefit, lasting over three years. This effect was maintained until the patient was last seen in clinic.
Peripheral nerve stimulation
One patient trialled the external vagal nerve stimulator for four weeks and found it ineffective. One other patient had an occipital nerve stimulator and reported improvements in disability score and headache severity lasting 10 months only.
Discussion
The supplementary commentary of the ICHD-3 acknowledges that individuals with NDPH can have pre-existing migraine or tension-type headache, but chronicity should not be that evolving from an episodic pattern, nor in association with acute-relief medication overuse. Furthermore, even though the criteria for CM or CTTH may also be met, the hierarchy dictates that if the onset is new, daily and persistent, the disorder is classified as NDPH and not CM or CTTH. In contrast if both criteria for NDPH and hemicrania continua are met, then the default diagnosis is the latter. Likewise, if the clinical syndrome is that of any other primary headache, then criterion ‘D’ dictates that the diagnosis is of that primary headache, for example, chronic cluster headache. If precipitated by a secondary pathology, then the headache is classified according to the precipitant in Part 2, the Secondary Headaches.
The question is what is the rationale for this distinction?
Clinical syndrome of NDPH
In NDPH the most common symptoms reported are ‘migrainous’. Such terminology continues to be used despite having a classification which allows the syndrome to be determined as migraine, probable migraine, another ICHD defined syndrome or, a completely novel syndrome (classified as 14.1). In our cohort most patients experienced a headache syndrome classifiable as CM with or without aura.
A general oversight of the ICHD-3 is lack of clarity about defining patients with a chronic daily headache syndrome and aura. The most common type of aura in episodic migraine is aura of reversible visual, sensory and dysphasic symptoms (15). In our cohort the most common was brainstem aura. Although true brainstem aura is rare, that with vestibular symptoms only is more prevalent and accepted within the Appendix of the classification (4,16). We confirm that, as noted in cohorts detailing aura, brainstem aura is most frequently reported in NDPH.
There have been case series of both thunderclap headache and valsalva headache as the initial events to the subsequent persistent daily headache (17,18). We found 15% reported a thunderclap onset and almost a third experienced recurrent thunderclap headache, in most self-limiting. Only one patient had recurrent episodes warranting prevention.
Exact recollection of onset
The reason for the criterion of exact recollection of onset is not elaborated on in the ICHD-3. It may be to ensure a new daily persistent onset, although precise recollection has been reported as low as 20% in some cohorts (10,19). If thought to be syndromically unique, there appears no clear difference between headache phenotypes with new daily persistent onset compared with their counterparts episodic-evolving-to-daily. In 1170 adolescents with continuous daily headache, 84.3% were diagnosed with CM and 13.2% with NDPH (20). The remaining 2.5% were diagnosed with another primary ICHD diagnosis (CTTH, post-traumatic headache and probable migraine). There were no subgroup differences between the group with CM and those with NDPH on comparing clinical syndrome except that those with CM were more likely to experience photophobia. Those with NDPH experienced their first headache at a slightly later age. Those with CM were more likely to be diagnosed with medication overuse.
Characteristic of specific recollection appears to be more likely the consequence of the impact of an event which alters quality of life from ability to significant disability within 24 hours. In contrast, the recollection following a secondary precipitant is an accepted norm. Moreover, there appears to be no clear phenotypic difference between the modes of onset of the same syndrome.
Treatment response
Our patients behaved similarly to patients with migraine in response to treatment and exacerbation by acute-relief medication overuse. This supports the inclusion in the ICHD-3 that a diagnosis of primary NDPH cannot be made in the presence of medication overuse.
It is more difficult to ascertain whether migraine or tension-type headache of new daily persistent onset is more intractable to that evolving from an episodic pattern. There are very few randomised-controlled treatment trials in CM compared to episodic, despite the greater burden (21). Evidence exists for topiramate, OnabotulinumtoxinA and the calcitonin-gene-related peptide monoclonal antibody preparations (22). There are reported benefits for topiramate and OnabotulinumtoxinA (10) in NDPH, albeit open label. Thus, as yet there remains little to support that NDPH with CM phenotype behaves therapeutically differently to its episodic-evolving-to-chronic counterpart, in particular those evolving rapidly within weeks or months.
Comorbidities
Recent decades have focused largely on the biological processes in headache disorders. This has resulted in the development of successful target-specific treatments in migraine, from the triptans to the CGRP monoclonal antibody preparations (22). Yet, the persistence and intractability of pain may be driven by the contribution of the additional psychological (behavioural), and social (environmental) factors (23) as has been shown for CM (24–28). Anxiety, depression, somatisation and pain catastrophising have been shown to be significantly more prevalent in NDPH compared to controls and patients with chronic low back pain (19). Psychiatric comorbidity was confirmed in our cohort. It has been proposed that these factors may contribute to the refractory nature of the disorder. Data on NDPH in adolescents shows that the peak months of onset coincide with the start of the school year, a time of heightened psychosocial stress (20). Thus, the onset of NDPH may occur in those with personality traits which alter the threshold for precipitation and perpetuation of the daily headache. This would be consistent with stress as one of the most consistently reported triggers to the onset of NDPH.
Triggers of NDPH
The triggers of NDPH have garnered interest as to their particular relevance. Our cohort had a lower proportion of triggering events, which may have been elucidated with more in-depth scrutiny (29).
There are a number of relatively consistent and some novel triggers. Typical examples include stress, post-surgery, ‘flu-like illness and serology supported viral infection (7,30). More recently reported is COVID-19 related persistent headache (31) and, not unsurprisingly, there were similar reports during the 1890 pandemic (32). Other single reports include terbinafine, an antibiotic, pesticides or post-syncope (33). However, this is in fact no different to the concept of the secondary headaches. Currently the secondary headaches are defined by precipitant. The diagnosis is presumptive based upon a temporal association (4). Until the most recent classification, another pre-requisite was resolution of the headache within three months following treatment or resolution of the offending pathology. ICHD-3 has now recognised that once a pathology has been adequately treated, the precipitated headache does not necessarily resolve. These cases are fundamentally new daily persistent headache precipitated by another pathological trigger.
At least 50% of NDPH cases do not identify a trigger. This is relevant to the concept of primary and precipitated NDPH, because those where a secondary cause or a ‘trigger’ has been identified are currently classified as a secondary headache, which is synonymous with ‘triggered’ new daily onset headache.
There does seem to be a higher prevalence in NDPH of prior migraine than one would expect in the population, suggesting that these individuals are predisposed to developing a headache disorder. This is consistent with the increased prior history of headache in other persistent secondary headaches, such as post-traumatic headache (34). It remains to be seen whether in the non-triggered group there are subclinical and epigenetic precipitants which cannot be so readily identified.
Conclusion
Thus, the question arises as to why new onset daily persistent migraine or tension-type headache warrant a separate definition within the rubric of ‘NDPH’. The same rationale is not applied to other primary headaches, in fact the converse, as stated in the supplementary commentary of the ICHD-3. There appears to be no clear difference in clinical syndrome of CM or CTTH with new daily persistent onset compared to episodic-evolving-to-daily. Only 1.5% of our cohort could not be classified within the ICHD-3. Treatment responses are consistent with current evidence as per clinical syndrome. Those cases precipitated are consistent with triggers currently classified as a secondary headache, and as seen with the latter, in the NDPH group there is a higher proportion of patients with a predisposition to headache, suggesting lowered threshold for developing the headache.
Key Findings
The majority of patients in our cohort experienced a syndrome consistent with ICHD-3 chronic migraine with similarities in demographics, comorbidities and treatment responses. Almost half had a past history of headache suggesting an inherent predisposition. Only 1.5% could not be defined by another ICHD-3 syndrome supporting that the new-persistent aspect of the disorder is a mode of onset rather than a unique phenotype and thus disorder. Chronic primary headaches with other ICHD-consistent syndromes, with new daily persistent onset, are classified as per syndrome, e.g the trigeminal autonomic cephalalgias. In these disorders the clinical syndrome and not mode of onset, guides treatment responses. We therefore propose that NDPH with migraine or tension-type headache phenotype is classified in the respective sections of the ICHD. Whether different to chronic migraine or tension-type headache evolving from episodic remains to be evaluated.
Footnotes
Acknowledgments
We would like to acknowledge the contribution of Dr Elisabetta Cittadini in advising on the differential diagnosis between NDPH and hemicrania continua.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Anish Bahra has participated in fee-based services on advisory boards and lecturing for Teva, Eli Lilly and Novartis Pharmaceuticals
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.