
Abstract
Introduction
Olfactory hallucination during a migraine attack (OHM) is a rare phenomenon. At present, it is not considered a manifestation of migraine aura.
Material and methods
The clinical features of OHM were collected in 11 patients.
Results
Of the 11 patients, 10 had migraine without aura and one migraine with aura associated with OHM. Mean age at onset of headache and at appearance of OHM were respectively 17.8 and 32.3 years. Migraine average frequency was 3.9 attacks/month, 19% of them being associated with OHM. The temporal pattern of OHM maintained the same characteristics in the different attacks. OHM onset was described as sudden (n = 5), gradual (n = 3), initially sudden and then gradual (n = 2), or developing in a few seconds (n = 1). In most of the cases (n = 8) OHM lasted from 3 to 10 minutes; it persisted during the pain phase (2–24 hours) in only three patients. The type of the perceived smell was invariably constant in nine patients.
Conclusion
OHM features fulfilled the ICHD-III beta criteria for typical aura.
Keywords
Introduction
Olfactory hallucination or phantosmia is defined as the perception of a smell without the substantial existence of any physical odor. Phantosmia has been recognized since ancient times: In 131 AD, Aretaeus the Cappadocian reported the observations that has to be considered the first written description of cingulate seizures (“a heavy smell sometimes preceded the accession of a paroxysm” and “sometimes the smell of the gagate stone makes them fall down”) (1). On the contrary, the term “aura” (literally “a breath of air”) was introduced by Pelop, master of Galen, referring to the perception of an odor that precedes an epileptic seizure (2).
Although olfactory hallucinations can occur in several neurological and even non-neurological conditions, temporal lobe epilepsy is the most common cause of phantosmia. In contrast, olfactory hallucination during a migraine attack (OHM) is a rare but probably underestimated phenomenon. It is not considered a type of migraine aura according to the International Classification of Headache Disorders, third edition beta (ICHD-III beta) (3). OHM occurs in about 0.1% of adult migraineurs (4) and appears to be more frequent during childhood. In a recent study of pediatric headaches, the prevalence of OHM was 3.9% among migraineurs (6.5% in MA) (5). However, the true prevalence of OHM is unknown. Probably because of the different emotional impact on patients, olfactory hallucinations seem to be less noticeable than visual ones and therefore are not often mentioned during the medical evaluation, resulting in an underestimation of their frequency.
A recent review of 39 OHM cases has been published by Coleman et al., who describe many of the characteristics of olfactory hallucinations in their patients as well as those in the literature (6). However, some of the clinical features of OHM still need better clarification, especially with regard to frequency, onset and resolution of the symptoms.
Herein we report the clinical features of OHM prospectively collected via a detailed and structured anamnesis obtained in 11 patients who came into our outpatient clinic. They each spontaneously mentioned the presence of OHM associated with their headache attacks. In addition, we have recorded and detailed the efficacy of their preventive therapy.
Material and methods
Proposed questionnaire for the prospective study of OHM.
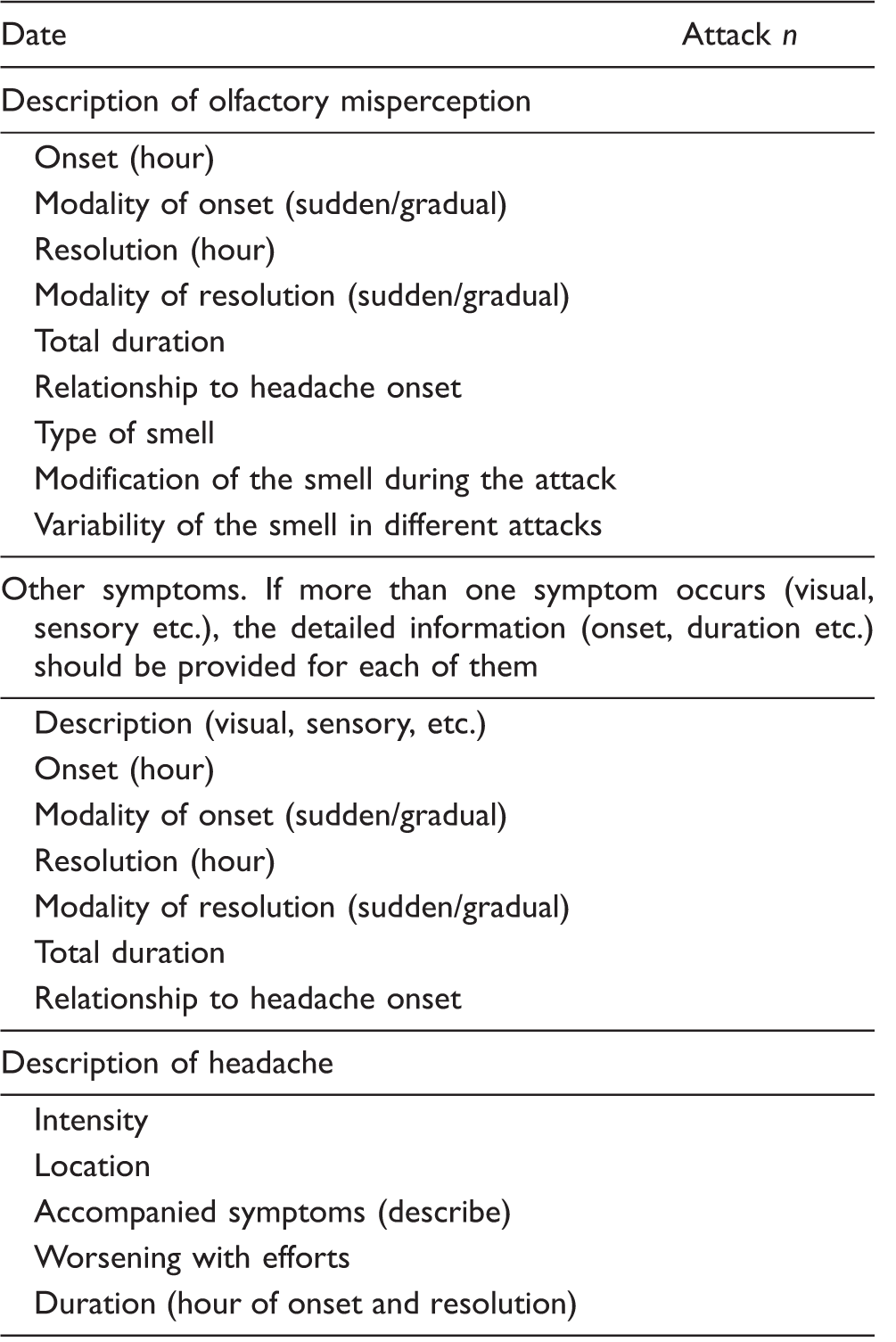
OHM: olfactory hallucination during a migraine attack.
Findings
The mean age at first evaluation was 40.0 years (range 25–56). The onset of the headache was at 17.8 years (range 5–31) while OHM appeared at a mean age of 32.3 years (range 5–54). All the patients but one received a diagnosis of migraine without aura (MO), while one patient complained of migraine with aura (MA) attacks. None of the patients had more than 14 days of headache per month. In six cases, a concomitant primary headache was diagnosed: three MA, two episodic tension-type headache and one primary stabbing headache. Each of the headache diagnoses fulfilled the ICHD-III beta criteria for the respective nosographic form. Physical and neurological examinations, routine blood tests, contrast-enhanced (CE) brain magnetic resonance imagings (MRIs) and electroencephalograms (EEGs) were unremarkable. In nine patients a control EEG performed after an average time of six months from the prior one showed no abnormal activity.
Relationship between onset of headaches and OHM appearance
Headache onset, mean frequency of headache attacks and occurrence of OHM on the total of the attacks.

Pt: patient; F: female; M: male;
OHM: olfactory hallucination during a migraine attack; MO: migraine without aura; MA: migraine with aura; ETTH: episodic tension-type headache; PSH: primary stabbing headache.
Migraine subtypes
In all but one patient, OHM occurred during an MO attack; only patient 1 complained of OHM exclusively during MA. Three patients (patients 2, 6 and 8) described OHM both in MO and, less frequently, in MA attacks. When associated with MA, OHM occurred during the visual aura in two patients, while in the remaining one it preceded the visual phenomena (patient 6). The average migraine (MO and MA) attack frequency is reported in Table 2.
Pain phase features
Clinical features of OHM.
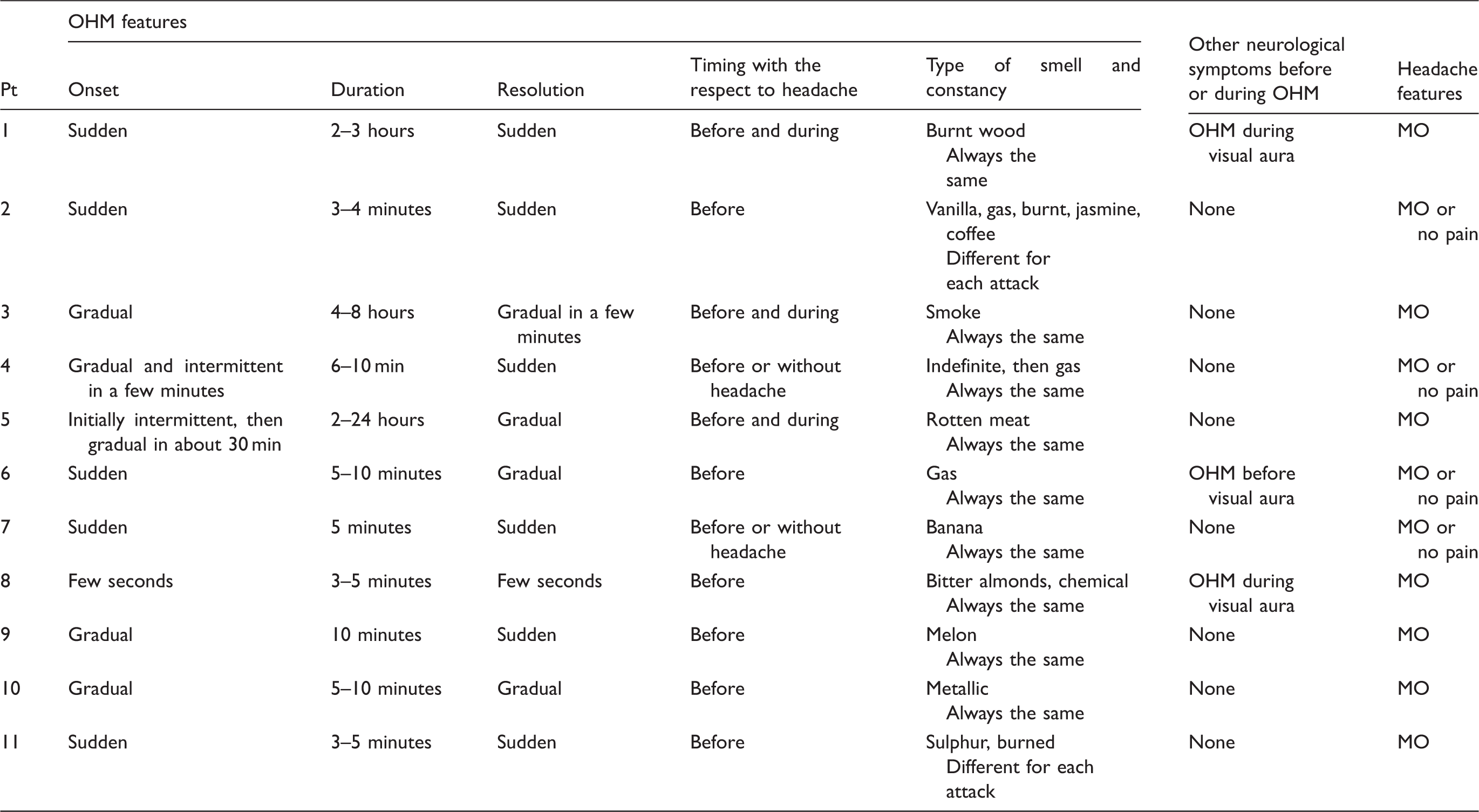
Pt: patient; OHM: olfactory hallucination during a migraine attack; MO: migraine without aura; MA: migraine with aura; ETTH: episodic tension-type headache; PSH: primary stabbing headache.
Migraine attacks and OHM frequencies
During the period of observation, a total number of 831 (MO: 728; MA: 103) migraine attacks were recorded by the patients, with an overall average frequency of 3.9 attacks per month for many months. Of these, 141 were OHM related (average: 0.75/month). The prospective average frequency of OHM- and non-OHM-associated migraine attacks recorded by the patients on their diary cards is reported in Table 2.
Characteristics of OHM
OHM information prospectively recorded by each patient is summarized in Table 3. For each individual patient, the temporal pattern of OHM maintained the same characteristics in each of the different attacks. The onset of OHM was described as sudden in five patients, gradual in three, initially sudden and then gradual in two or in a few seconds in one. In most of the cases (n = 8), OHM lasted from 3 to 10 minutes. It persisted during the pain phase (2–24 hours) in only three patients in whom the pain occurred within 10 minutes from the onset of OHM. The disappearance of OHM was noted as sudden in six and gradual in four; one patient described both the onset and resolution of OHM in a few seconds. Interestingly, no modification of the perceived smell occurred in the course of the single attack; nevertheless, in two patients (patients 2 and 11) the type of odor could change from attack to attack. All the patients reported a possible modification in the intensity of perception, which could be mild or extremely intense. The quality of the smell was defined as consistently unlikeable in eight patients and quite pleasant in two (patients 1 and 9). In one of these cases (patient 1), the experienced smell changed for every attack.
Acute treatment
Acute treatment with triptans was suggested in all the patients, with an overall satisfactory efficacy. The reduction of pain intensity or a complete resolution of pain within two hours of taking the triptan was obtained in 78% and 53% of the treated attacks, respectively. The patients were told to get the triptan ready at the time of onset of OHM, just before the beginning of the painful phase. When this was accomplished, they had the additional advantage of early treatment, with an improvement both in pain relief (83%) and pain disappearance (57%) at two hours. The average monthly intake of medication was consistent in all patients and, therefore, none of them developed medication-overuse headache according to the ICHD-III beta criteria.
Preventive treatment
Preventive treatment: efficacy on the frequency of overall headache attacks and OHM-associated attacks.

Pt: patient; OHM: olfactory hallucination during a migraine attack; MO: migraine without aura; MA: migraine with aura; ETTH: episodic tension-type headache; PSH: primary stabbing headache.
Discussion
The exact prevalence of OHM is unknown. In a tertiary care study of 952 adult migraineurs, OHM occurred in about 0.1% of the cases (4). Its frequency appears to be higher during childhood. A total of 3.9% of the 537 patients with MO had OHM, a percentage that increases to 6.5% in those who had MA (5).
Worldwide diagnostic criteria of OHM have still not been proposed, nor has an unequivocal pathogenetic interpretation of this phenomenon been found. In a recent review (6), Coleman et al. retrospectively described 39 patients (14 new cases and 25 from the literature) complaining of OHM. As most of the data were obtained by a review of the literature, detailed information regarding the clinical aspects of OHM presentation are partially lacking and do not allow a global vision of the phenomena. In particular, the details concerning the modality of disappearance, the constancy of the perceived smell among different attacks and the frequency of its occurrence were not reported.
In the present case series, 11 patients presenting with OHM were prospectively followed with regular outpatient visits; their headache features, including of their OHM, were recorded on a headache diary card and described in detail by answering a specific questionnaire. The frequency of OHM episodes ranged widely from two attacks per year to three to four attacks per month. In all the cases, OHM began before the pain phase; in eight cases it resolved before the appearance of pain, and it persisted during the onset of the headache in the remaining. The onset of OHM was sudden in five cases, gradual in three cases, intermittent in two cases, while one patient described the development over a few seconds.
OHM duration ranged from only 3–5 minutes up to 24 hours. In six cases (patients 1, 2, 4, 7, 10 and 11) the resolution of OHM was sudden, in four patients gradual, and in one patient the symptom resolved in a few seconds. The perceived smell was reported as consistently unpleasant by eight patients, inconsistently pleasant by two. Only one patient (patient 7) reported a distinctly pleasant olfactory perception. Most patients described the same exact smell during the course of each individual attack; in nine cases the same odor occurred in every attack. Only two patients mentioned a change of smell for each individual attack. Osmophobia, as an accompanying symptom during a migraine attack, was preceded by OHM and reported by five patients. It has been clarified that OHM and osmophobia are two distinct clinical symptoms, the latter defined as an unbearable perception, during a migraine attack, of odors that are non-aversive or even pleasant outside the attack (7,8). Although we understand this distinction, the terms osmophobia and OHM could cause problems in differential diagnosis. A literary example of such difficulty can be found in the novel The Master and Margarita by the Russian medical doctor and writer Michail Bulgakov. In chapter 2, the unbearable perception of rose, which afflicts Pilate before and during his typical headache attack, could be initially interpreted as OHM since the source of this olfactory stimulus is apparently lacking. However, several pages later, the description of a rose garden is given. Therefore the symptom has to be interpreted as osmophobia rather than an OHM (9).
The headache associated with OHM presented with migraine features in all the cases. In four cases (patients 2, 4, 6 and 7) the pain phase could be absent and OHM occasionally presented as an isolated symptom (OHM without headache, analogous to visual aura without headache).
The main features of OHM in our case series are reported in Tables 2 and 3. The modality of presentation, the length and the resolution of the transitory neurological deficit could be considered as the most important features, suggesting that OHM may be similar to typical aura symptoms rather than other unpleasant olfactory perceptions that may appear in different conditions, such as vascular, epileptic or psychiatric disorders; therefore, this new entity should be considered for inclusion in the appendix of the next ICHD. Although none of the patients were examined during an OHM episode in our case series, interictal EEG as well as 24-hour ambulatory EEG recording resulted in normal findings and olfactory hallucination secondary to temporal lobe epilepsy has been reasonably excluded.
All but one of the patients received a preventive migraine treatment and reported an overall improvement in the frequency of their attacks. The reduction of OHM-associated and non-OHM-associated attacks was substantially proportional in six cases, while in four (patients 1, 4, 7 and 10) OHM completely disappeared and non-OHM attacks improved at least 50%. Interestingly, they were treated with antiepileptic drugs, three with topiramate and one with lamotrigine.
Despite several pathogenetic hypotheses that have been advanced, the real mechanisms of OHM remain uncertain. Cortical spreading depression (CSD) should be the common denominator that links the typical aura symptoms to OHM: This hypothesis should find confirmation in the affinity between the clinical features of the two phenomena, as previously remarked by Coleman et al. (6) and confirmed by our data. In addition, the presentation of OHM together with typical visual aura in most of our patients supports this theory. Moreover, topiramate, valproate, amitriptyline and DL-propranolol, considered first-line drugs in the preventive treatment of MO and MA, suppressed CSD generation in experimental animals (10). From this perspective, OHM, which precedes an MO attack, should be sustained by a CSD, involving the piriform cortex, the olfactory cortex in the temporal lobe and orbito-frontal cortex, as previously proposed (6), and, at the same time, inducing a sterile inflammatory response by the activation of the trigeminovascular system. The aura-like temporal pattern of the OHM clinical expression reflects the neuro-vascular phenomena at the basis of the CSD. From this perspective, it could be assumed that the same mechanism should involve leading to OHM.
Furthermore, the role of the piriform cortex and its connection with the trigeminovascular system has been supported by neuroimaging (11,12).
From a clinical perspective, an appropriate study of OHM should consider the qualitative features (type of smell, constancy with regard to different episodes of headache) as well as information regarding the modalities of onset and resolution, duration, relation to the pain phase and characteristics of the headache. If adequately investigated, the clinical manifestations of OHM may well fulfill the ICHD-III beta definition for aura symptoms, as it appears in our case series. A proposal of a possible prospective questionnaire is reported in Table 1. The presence of OHM is uncommonly investigated by physicians and, at the same time, the patient might consider it as a non-important element to be mentioned. The real prevalence of OHM phenomena may be low in the same way that isolated motor, sensory or aphasic aura is infrequent (13); but the lack of awareness by physicians may cause many to miss this phenomenon.
Conclusion
OHM is an uncommonly reported event, most likely because it is rarely spontaneously mentioned or asked about during the clinical interview. It presents with some characteristics of typical aura, but with a wide range of variability. When properly asked about it during the history, patients are able to describe in detail the features of their olfactory hallucinations. This type of information should be collected in prospective studies, with the aim of reaching a more accurate description of the clinical pattern of OHM. We propose a questionnaire model (Table 1) for the collection of prospective data that could allow for its better characterization, which will lead us to learn its true prevalence. This could eventually lead to the recognition of OHM as a manifestation of aura. If this is the case, it could be inserted among the diagnostic criteria of MA, in the appendix section of the next ICHD.
Key findings
Although olfactory hallucination is a well-recognized phenomenon, its prevalence in association with a migraine attack is not known. Probably because of the different emotional impact on patients, hallucinations of smell may be less noticeable than visual ones, and therefore are not uncovered during the medical evaluation; this results in an underestimation of the phenomenon. The clinical manifestation of olfactory hallucination during a migraine attack (OHM) may fulfill the International Classification of Headache Disorders, third edition beta (ICHD-III beta) definition of aura. We hypothesize that OHM may be sustained by spreading depression that involves the piriform cortex and activates the trigeminovascular system. Prospective studies involving a large, multisite sample of patients could clarify the prevalence of OHM and lead to a more accurate description of its clinical features. If this study corroborates the fact that the clinical features of OHM fit the criteria of migraine aura, then OHM should be listed among the other typical aura symptoms in the appendix of the next ICHD.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.