
Abstract
Background
The long-term consequences of paediatric headache can involve functional disabilities and mental health problems in adulthood.
Objective
To analyse the predictive power of paediatric headache trajectory classes for headache and related outcomes in adulthood.
Methods
In a previous study, a population-based sample (N = 3227, 9–14 years of age at first assessment) was followed across four annual assessment points, and sex-specific headache trajectory classes were identified (girls: “no pain”, “moderate pain”, “increasing pain”, “high pain”; boys: “no pain”, “moderate pain”). These trajectory classes were used to predict headache frequency, functional disability, depression, quality of life and self-efficacy nine years later (N = 994). Negative binomial regression analyses and pairwise comparisons were computed.
Results
Women showing an elevated trajectory (“increasing pain” or “high pain”) had a higher adult headache frequency and a poorer outcome on associated variables (functional disability, depression, quality of life, and self-efficacy) than women having a lower-level trajectory. Men of the “no pain” and “moderate pain” trajectory classes differed significantly from one another in their headache frequency and related variables.
Conclusion
Belonging to an elevated paediatric headache trajectory class involves a considerable risk for headache and headache-related problems in adulthood.
Keywords
Background
Headache constitutes a frequent pain syndrome in children and adolescents (1,2). In population-based studies, the prevalence rates differ depending on the study sample, the diagnostic criteria and the method used to assess headache (1,3). In a review of the epidemiology of paediatric headache (4), the overall mean prevalence of headache was 54.4% (95% CI 43.1–65.8), referring to time periods between one month and an entire lifetime. Prevalence rates increase with age and seem to reach their peak at the age of 13 (2,5). From adolescence onwards, girls report headache significantly more often than boys (3,6,7). This sex difference remains stable throughout adulthood (8–10).
Paediatric headache can be associated with psychological symptoms such as depression and anxiety (5,11). It may also be related to functional disabilities, including school absence and impaired family activities (1,12). In particular, very early occurring and severe paediatric headache that remains untreated predicts headache in adulthood (5,13,14).
Adult headache is often associated with impairments in many areas of life (15–20). For example, adult headache is related to disabilities in social and work life as well as leisure activities (16,21,22). This not only implies a burden on the healthcare system but may also contribute to unfavourable affective states, lower quality of life, and self-efficacy as well as social withdrawal. These factors may in turn lead to further aggravation of pain symptoms (8,15,16,23).
Furthermore, adult headache can be associated with major depression and dysthymia – two of the most common psychiatric diagnoses in headache patients (8,24). However, the causality of this relationship still remains unclear (24). Some authors assume a bidirectional influence (25,26).
Research on developmental courses of headache from childhood to adulthood is highly relevant in order to determine changes of headache frequency across a broader life span and to identify related psychological and psychosocial factors. However, until now, only a few population-based studies have focused on a longitudinal perspective. In a study of 100 adolescent patients, 79% showed an improvement or were headache-free eight years later (27). Males showed a higher remission rate than females (52% vs. 21%). In contrast, Brna, Dooley, Gordon and Dewan (13) examined a sample of 95 children with paediatric headache and found that 73% still suffered from migraine and/or tension-type headache after 20 years. Bille (28) followed a group of 73 children and reported that the majority of them suffered from headache after 40 years. Carasco and Kröner-Herwig (29) examined a sample of 509 children and adolescents with migraine, tension-type headache, or non-categorizable headache, and found a remission rate of 23.9% two years after the baseline assessment.
These longitudinal studies, however, have limited informative value since the statistical methods did not consider a potential heterogeneity in the samples and did not allow researchers to model patterns of change across time in an adequate manner.
In a previous study, our research group used Latent Class Growth Analysis (LCGA) (30,31) to identify sex-specific headache trajectories of 3227 children and adolescents (9–14 years old at first assessment) from a population-based sample who completed four annual assessments (32). In order to find the best-fitting model, statistical fit indices (e.g. BIC, entropy), theoretical implications as well as considerations on the usefulness and validity of the classes were used to support the decision process.
Four different trajectory classes were identified for girls and two trajectory classes for boys. Our results showed that headache developed differently between boys and girls, with a higher heterogeneity in the female subsample. In women, a trajectory class with a high headache frequency across all time points was found (“high pain”), as well as a trajectory class with an increasing headache level that stabilised by the time of the fourth wave (“increasing pain”). Besides that, we also identified a trajectory class that was defined by a moderate headache frequency at the starting level, with a significant decrease that accelerated over time (“moderate decreasing pain”). The fourth trajectory class of the female subsample included individuals with a very low level of headache frequency across all four time points (“no pain”). A similar trajectory class could be found in the boys’ data set (“no pain”). Moreover, we identified a class with a moderate number of headache days across all time points (“moderate stable pain”) in the male subsample. The different trajectories are presented in Figure 1.
Trajectory classes for girls and boys, after Isensee et al. (2016).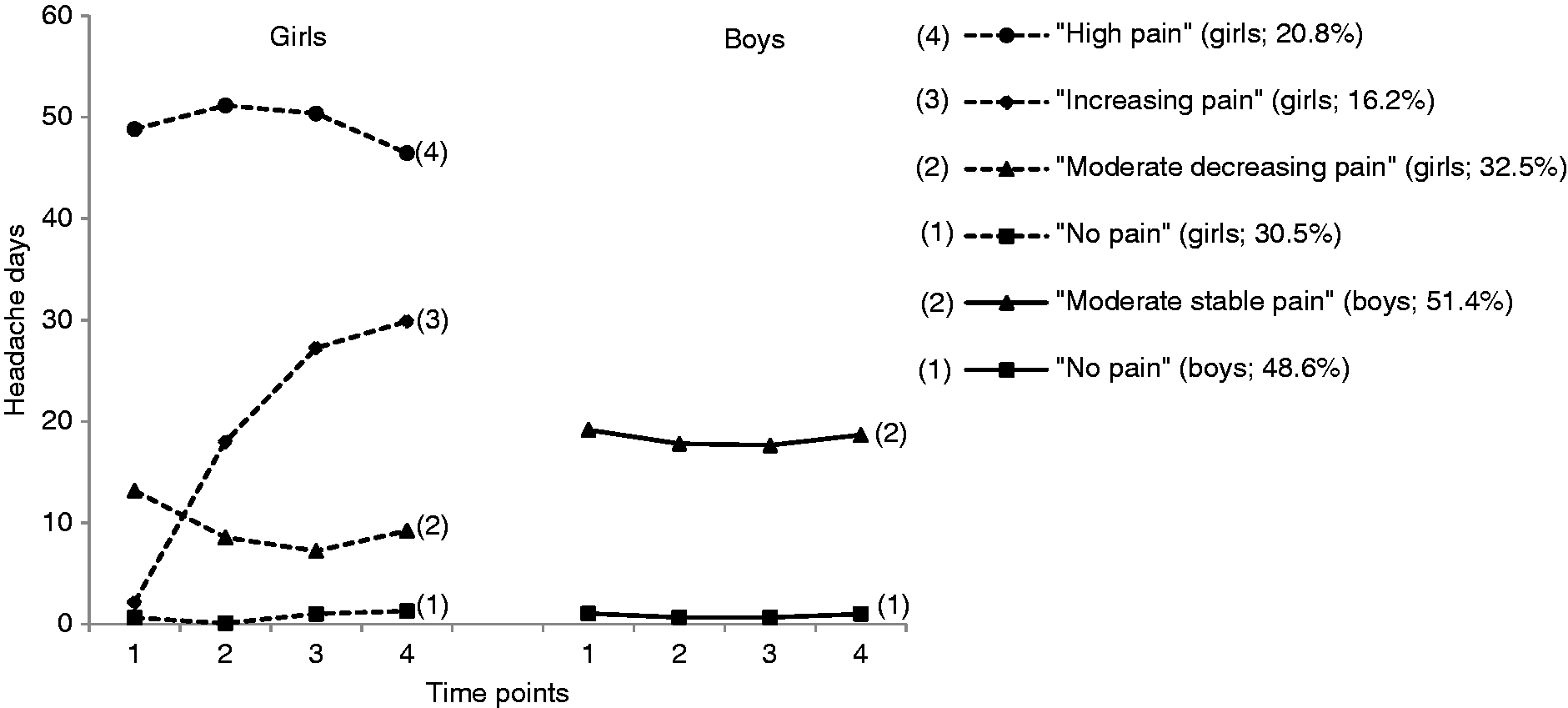
Study objectives
To our knowledge, no prior research used empirically established classes of headache trajectories in childhood and adolescence to predict headache frequency and related functional and psychological disability in adulthood. Thus, the aim of the present study was to address the two following research questions:
Will the identified trajectory classes predict headache frequency in young adulthood? Will individuals in these trajectory classes differ in their levels of functional disability and indicators of psychological functioning (i.e., depression, quality of life, and self-efficacy) as adults?
These questions lead to the following hypotheses:
Being assigned to a pain trajectory class in childhood/adolescence will predict higher levels of headache frequency in young adulthood compared to a categorisation into the “no pain” trajectory class. As we have three pain trajectory classes in the female subsample, it is expected that women of the “high pain” and the “increasing pain” trajectory classes will show a higher headache frequency at wave 5 compared to females of lower-level trajectory classes (the “moderate pain” and “no pain” classes). Individuals of the pain trajectory classes compared to no pain classes will report higher levels of pain-related functional disability, more depressive symptoms as well as a lower quality of life and self-efficacy at wave 5. Women of elevated trajectory classes will again be most likely to have higher levels of dysfunctional characteristics in comparison to females in the “no pain” and “moderate pain” classes.
In line with previous studies, it is expected that women will demonstrate a higher headache frequency than men (3,6,9).
Methods
Participants and procedure
The current work is part of a large longitudinal population-based study with five assessment points. The ethics committee of the German Association of Psychology approved the study protocol. Subjects were between 7 and 14 years old at the first wave. Via a postal survey and an online questionnaire (added in wave 5 only), participating families were asked to report on headaches and other health-related psychosocial variables of one child. Families gave their written informed consent to an anonymous analysis of the data. The first four waves were conducted in consecutive years (2003–2006), and the fifth was nine years later. The families were selected randomly from four districts in Lower Saxony and the city of Hannover (Germany) via community directories. At first assessment, 8800 families were contacted. The response rate was 63.5%. Families responding in the first wave were contacted in the following four surveys. Since young children would have had difficulties answering the questionnaire, only parents’ reports were gathered for children aged seven to eight. Older children were asked to fill in a questionnaire themselves. Both children and parents completed separate questionnaires in waves one to four. In the fifth wave, only the children, now 19–27 years old, were contacted via their parents. They were asked to respond to a postal survey or an online questionnaire with the same questions. In all, 1650 individuals answered the postal survey, and 215 answered the online questionnaire.
The current sample is based on the study by Isensee et al. (32) in which children and adolescents (N = 3227) were classified into different trajectory classes based on their self-reported headache frequency across the first four waves. Children of these trajectory classes were included in the sample of the current study if they had at least responded to more than half of the questions of the survey of the fifth wave. This led to a reduction of the sample size (N = 1048). An additional reduction resulted due to mismatches of stated age and sex between waves 1 and 5 (N = 54; 1.7%). As a consequence, the final sample consisted of N = 994 individuals (41.9% men; 58.1% women). Males showed similar response rates in the different classes in the transition from childhood/adolescence to adulthood (“no pain”: 36%; “moderate stable pain”: 31%). Response rates differed more between female trajectory classes (“no pain”: 46.7%; “moderate decreasing pain”: 48.1%; “increasing pain”: 39.5%; “high pain”: 39.6 %). Thus, females in the elevated trajectory classes had a lower response rate. The mean age of the sample was 23.54 years (SD = 1.76; men: M = 23.50, SD = 1.74; women: M = 23.58, SD = 1.77). The lower (42.2%) and the middle (51.2%) socioeconomic status groups (SES; 33) were overrepresented in the sample. However, at wave 5, SES reflected a transition phase of the individuals that cannot be considered a stable and valid description of their status. No significant differences were found between individuals participating in online vs. postal survey at wave 5 concerning age and headache frequency (all p > 0.05). A slightly higher number of males responded to the online survey. As the effect size was very small (r = 0.04) this result was considered negligible.
Measures in wave 5
Headache frequency
In order to assess the level of mean headache days, individuals were asked whether they had experienced headache in the last six months “at least once a week” (3), “at least once a month” (2), “less than monthly” (1) or “never” (0). Following this, they had to specify the exact frequency of experienced headache in the chosen period. The stated frequency was extrapolated to six months, so that headache frequency could range between 0 and 182.
Functional disability
In order to assess interferences of headaches with daily activities in the last six months, three items of the “Chronic Pain Grade” (34) were administered and ratings were averaged. Items were rated on an 11-point scale from “no interference” (0) to “unable to carry on any activities” (10). The items addressed everyday activities, school activities, and familial or leisure activities (e.g., “In the past six months how much have headaches interfered with your family or leisure activities?”). Homogeneity of the scale is very good, with Cronbachs α = 0.89.
Depressive symptoms
In order to measure depression, the module “major depressive syndromes” (PHQ-9) of the German Patient Health Questionnaire (PHQ-D; 35) was used. Here, nine items (e.g., “feeling down, depressed or hopeless”) assess the level of depressive symptoms on a four-point-scale from “not at all (0)” to “almost every day” (3). The sum of the nine items (0–27) was used as an indicator of depressive symptoms. Kroenke, Spitzer and Williams (36) found good to excellent reliability and validity of the instrument.
Quality of life
Individuals’ quality of life was assessed with six items that were adapted from the short version of the Child Health Questionnaire (CHQ-50; 37,38) in order to achieve a better comparability with the previous assessment points of the survey. The individuals were asked to evaluate their satisfaction with life in general and in specific areas of life in the last three months (school/ professional and athletic performance, friendships, physical appearance, health; e.g., “How satisfied have you been in the last three months with your friendships?”). The items were rated on a five-point scale from “very unsatisfied” (1) to “very satisfied” (5). Homogeneity of the scale is satisfactory with Cronbachs α = 0.73.
Self-efficacy
The three items of the ASKU-scale (General Self-Efficacy Scale, short form; 39) were used to assess self-efficacy of individuals. Individuals had to evaluate the applicability of three statements (e.g., “I can rely on my own abilities in difficult situations.”) on a five-point scale from “doesn’t apply at all” (0) to “applies completely” (4). For each individual, a mean score was calculated with higher scores indicating higher self-efficacy. Reliability and validity are satisfactory (39).
Statistical analyses
To test the first hypothesis on the predictive power of paediatric headache trajectory classes for headache frequency in young adulthood, the four classes of trajectories in the girls’ subsample (“no pain”; “moderate decreasing pain”; “increasing pain”, “high pain”) and two trajectory classes in the boys’ subsample (“no pain”; “moderate stable pain”) were dummy-coded. The ‘no pain’ class was the reference class for both sexes. This resulted in three dummy variables for women (‘moderate decreasing vs. no pain’; ‘increasing vs. no pain’; ‘high vs. no pain’) and one dummy variable for men (‘moderate stable vs. no pain’). Our main outcome variable (headache frequency) turned out to have a non-normal, highly skewed distribution. Figure 2 shows the empirical distribution for females and males and a negative binomial distribution fitted to it. This distribution fitted the data best. In consequence, negative binomial regression analyses were carried out. A negative binomial regression analysis is used for count data (i.e., headache frequency) when the data show an overdispersion (more variance in the data than the model can explain) that cannot be accounted for by a Poisson distribution (40). The dummy variables were included as predictors in the negative binomial regression models simultaneously. Separate regression analyses for men and women were carried out.
Empirical distribution of headache frequency for women and men and a fitted negative binomial distribution.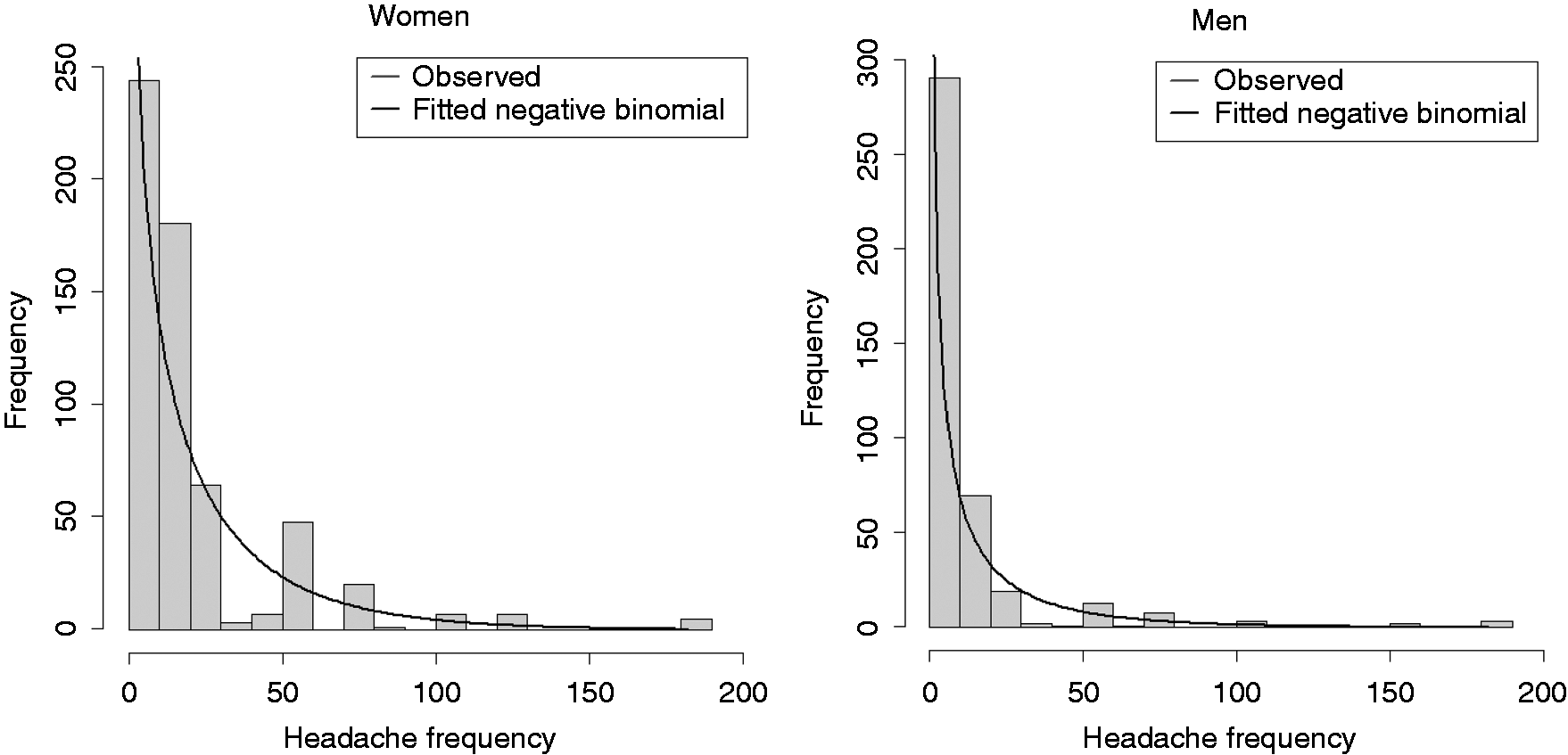
To compare headache frequencies between trajectory classes, Kruskal-Wallis tests for women (four classes) and Mann-Whitney U-tests (U) for men (two classes) were carried out. The r coefficient was used as effect size with r = 0.1–0.3 indicating a low effect, r = 0.3–0.5 a moderate effect and r > 0.5 a large effect (41).
In order to answer the second research question on sex-specific trajectory class differences regarding functional disability and indicators of psychological functioning in young adulthood, Kruskal-Wallis tests and Mann-Whitney U-tests were again carried out for both sexes separately. Since pairwise comparisons were used, p values were Bonferroni adjusted.
Data from individuals were included in the analyses only if more than half of the items on a scale were answered. Alpha level was set to 5%. Analyses were carried out using SPSS Statistics 23.
Results
Sex differences in headache frequency and related variables
Descriptive statistics for headache frequency and related variables at wave 5 (Means and SD or Medians and first and third quartile).
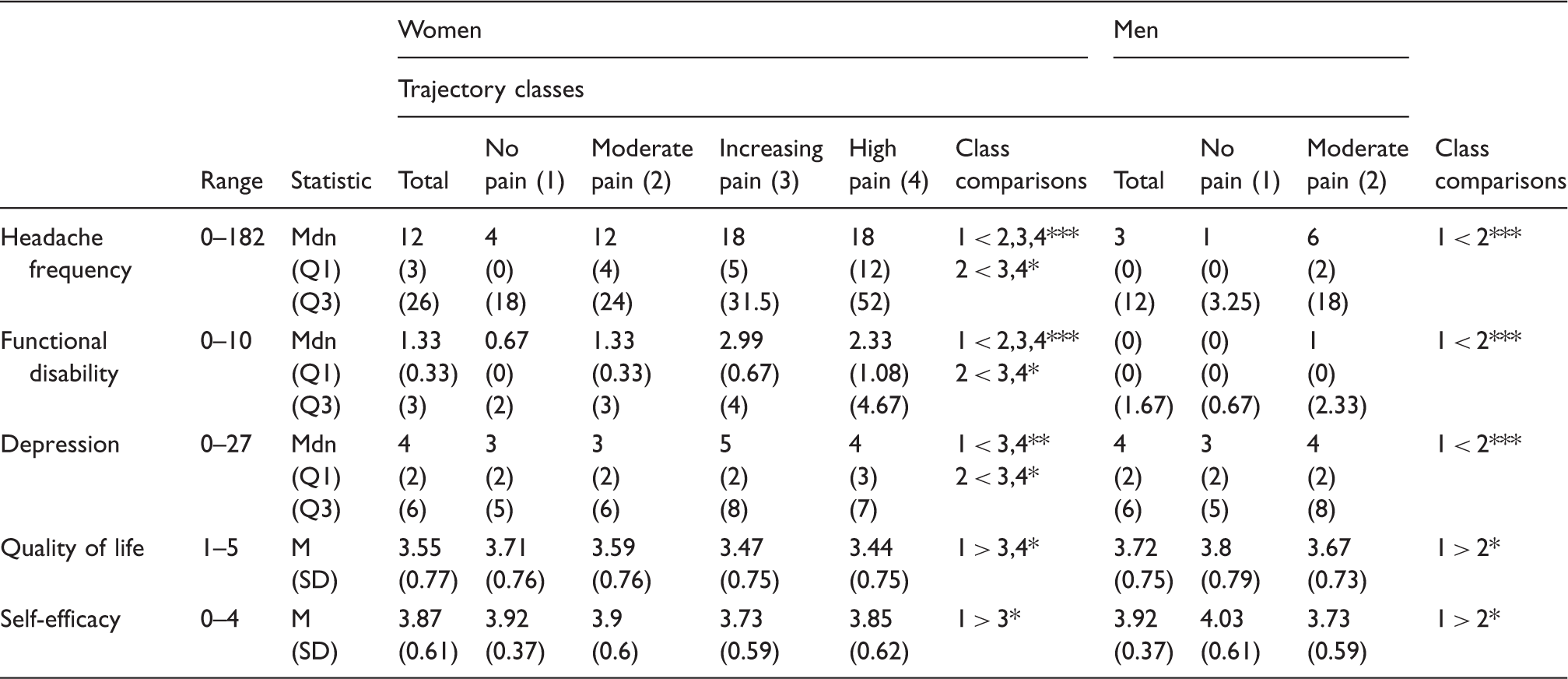
Note: women: “no pain” trajectory class (1) N = 185, “moderate pain” trajectory class (2) N = 203, “increasing pain” trajectory class (3) N = 83, “high pain” trajectory class (4) N = 107; men: “no pain” trajectory class (1) N = 219, “moderate pain” trajectory class (2) N = 197; pairwise comparisons are based on Kruskal-Wallis tests; one-sided testing, p values are Bonferroni adjusted; p < 0.05; *p < 0.05; **p < 0.01; ***p < 0.001; due to the skewed distribution of headache frequency, functional disability and depression the medians as well as the first and third quartile are shown for these variables.
Headache frequency: differences between trajectory classes in women and men
Results of negative binomial regression analyses on headache frequency at wave 5 for women (N = 575) and men (N = 413).

p < 0.05; **p < 0.01; ***p < 0.001
Men of the “no pain” and “moderate pain” trajectory classes also significantly differed in their headache frequency (r = 0.43).
Trajectory class differences for functional disability and indicators of psychological functioning in women and men
In the female subsample, significant differences in functional disability were found for almost all trajectory class comparisons (r between 0.10 and 0.29) except for the “increasing pain” vs. the “high pain” class (Table 1). With regards to the level of depression, women of the “no pain” and “moderate pain” classes differed from females of elevated trajectory classes (r = 0.10–0.13). Concerning quality of life (r = 0.11–0.13) and self-efficacy (r = 0.12), fewer class comparisons turned out to be significant in the women’s subsample (Table 1) and effects tended to be small.
For men, both trajectory classes differed significantly from one another in all headache-related variables (r = 0.09–0.37). Men in the “moderate pain” class had a higher functional disability, higher values of depression, lower quality of life, and less self-efficacy.
Discussion
The aim of the current study was to examine the predictive power of empirically established headache trajectory classes in childhood and adolescence for the status of headache frequency, functional disability, depression, quality of life and self-efficacy in young adulthood.
In accordance with prior findings (8–10) a significantly higher headache frequency in women compared to men was found. The higher frequency of headache in women may have contributed not only to a higher functional disability than in men but also to a lower quality of life and self-efficacy (12,42–44).
In agreement with our first hypothesis, headache trajectory classes were indicative of the level of headache affliction in young adulthood for both sexes. Women being assigned to the “high pain” or “increasing pain” trajectory class reported a substantially higher headache frequency than women being assigned to the “no pain” or “moderate pain” trajectory classes. This corresponds well with other studies that describe headache in childhood and adolescence as a risk factor for adult headache (1,5,28).
In accordance with our second hypothesis, subjects that were assigned to a pain compared to a no pain trajectory class reported significantly higher unfavourable levels on all headache-related variables. Women of the “increasing pain” and “high pain” trajectory classes showed significantly higher levels of functional disability and depression as well as a lower quality of life compared to females of the other classes. However, as can be seen in medians and quartiles as well as means and standard deviations, levels of functional disability and depression were low and levels of quality of life and self-efficacy tended to be rather high in each trajectory class of both sexes. Thus, none of the examined variables reached a level of clinical significance, and effect sizes of class comparisons proved to be only small to moderate, as would be expected in population-based studies. Nevertheless, findings emphasise the potential influence headache can exert on well-being in different areas of life, including the emotional, psychological, social and functional levels (8,21,26).
As compared to functional disability and depression, quality of life and self-efficacy differed less between the trajectory classes in women at wave 5. This may indicate a lower significance of these two psychological indicators for headache problems.
Strengths and limitations of the study
The large sample size and the long assessment period (in total 12 years) are considerable strengths of the study. Furthermore, the statistical methods used are powerful tools in evaluating the long-term developmental relationship between paediatric headache trajectory classes and headache problems in young adulthood. Thus, the study extends existing knowledge on the long-term course of headache by taking into account the heterogeneity of the sample as well as differences between sexes in an adequate statistical manner.
A limitation is the drop-out. Less than a third of the adolescents who were classified based on their headache trajectories could be included in the current study as young adults. This might be due to a lack of motivation in this population-based, non-clinical sample. A second limitation is a lack of knowledge about the period between wave 4 in 2006 and wave 5 in 2015. Changes in headache frequency as well as potential factors and interventions influencing these changes are unknown. A third limitation is that we cannot exclude a recall bias due to the postal and online survey used. This problem could only be overcome by using a continuous assessment of headaches, which was not feasible with regards to the large sample size of the study.
Another limitation is the lower response-rate of the female elevated trajectory classes in wave 5, which led to a slightly smaller variance in the data set. This may lead to an underestimation of the predictive power of these classes. Finally, the generalization of our results is limited since the study sample was not representative with regards to the general population.
Conclusion
Results indicate that being member of an elevated paediatric headache trajectory class substantially increases the risk of suffering from headache as a young adult. In particular, the female “high pain” trajectory class included a specific amount of women with high headache frequencies in young adulthood. Findings further highlight the impact paediatric headache may exert on adult life, including heightened levels of functional disability and depression.
Article highlights
This is the first study that uses empirically established and sex-specific paediatric headache trajectories to predict young adult headaches. Paediatric headache trajectory classes were compared with regards to the young adult’s level of functional disability, depression, quality of life and self-efficacy. Elevated paediatric headache trajectories involve a considerable risk for headache and related problems in adulthood.
Footnotes
Acknowledgments
We thank Anastasia Gorbunova for checking and preparing the data set.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research project has partly been supported by a grant from the German Ministry of Education, Research and Science as part of the German Headache Consortium.