
Abstract
Background
Intraorbital lesions associated with symptomatic trigeminal autonomic cephalalgias (TACs) are rarely reported. We present a case of orbital metastatic leiomyosarcoma, presenting with chronic paroxysmal hemicrania-like headache.
Case report
A 43-year-old man presented with a severe paroxysmal headache in his left periocular and frontal area for a year. The attacks occurred 10–12 times per day, lasting 10–15 minutes with ipsilateral lacrimation and conjunctival injection. Neurological examination and brain MRI without contrast were unremarkable. Different medications were tried, without beneficial effects. A follow-up contrast-enhanced brain MRI performed one year after the baseline MRI revealed an enhancing mass in the left superior oblique muscle. Orbital metastatic leiomyosarcoma arising from the thigh was revealed. He received gamma knife surgery, which completely resolved the headache.
Discussion
Intraorbital lesion should be considered a possibility in patients with headache mimicking TACs. Baseline contrast-enhanced MRI is essential, and repeated MRI scans might be needed if clinically indicated.
Background
Trigeminal autonomic cephalalgias (TACs) are characterized by severe unilateral headache with ipsilateral craniofacial autonomic manifestations, and their circadian rhythmicity. The group contains cluster headache (CH), paroxysmal hemicrania (PH), and short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT syndrome), and hemicrania continua (HC), classified based on the attack duration, frequency, and treatment response (1). While structural lesions associated with secondary TACs are generally located in the sella turcica or the cavernous sinus (2), intraorbital lesions involving the superior oblique muscle are rarely reported. We present a case of orbital metastatic leiomyosarcoma, presenting with chronic PH-like headache (3).
Case report
A 43-year-old man came to the neurological outpatient clinic complaining of severe throbbing paroxysmal headache localized in his left periocular and frontal area for one year before his visit. The attacks were accompanied by ipsilateral lacrimation and conjunctival injection, and occurred 10–12 times per day, lasting 10–15 minutes, at one-hour intervals. Neurological examination was normal, without painful eye movement or oculomotor palsies. The results from the pupil examination were normal, and no optic disc edema was found. A baseline non-contrast enhanced brain magnetic resonance imaging (MRI) with a slice thickness of 5.0 mm was performed; it was normal without observations of neurovascular contact of the trigeminal nerve. The laboratory findings, including erythrocyte sedimentation rate (ESR), showed no abnormalities. The headache was not exacerbated by movement of the eyes, and no tenderness was observed.
Indomethacin was partially effective at a dose of 75 mg/d, although no clinical response was seen despite increasing the dose up to 225 mg/d for one week. Besides, various medications were used together for a year; the drugs included sumatriptan (50 mg/d), prednisolone (from 5–60 mg/d), lamotrigine (200 mg/d), lithium (400 mg/d), verapamil (240 mg/d), topiramate (25 mg/d), and melatonin (4 mg/d). The patient received sphenopalatine ganglion (SPG) and occipital nerve blocks in addition to the oral medications. The SPG block resulted in the complete resolution of the headaches for two weeks, but the headache quality and oculomotor status did not show any change with the use of medications.
A follow-up contrast-enhanced brain MRI with 1.2 mm thick slices was performed one year after the baseline MRI (see Figure 1). The scan revealed an enhancing mass (22 mm in length) in the left superior oblique muscle. Positron emission tomography-computed tomography (PET-CT) scanning was performed to screen the metastasis. Orbital metastatic leiomyosarcoma arising from a primary focus in the right thigh was revealed with bone (twelfth thoracic vertebra, right fifth rib) and multiple lung metastases. He received gamma knife surgery (GKS) for the orbital leiomyosarcoma and also underwent palliative chemotherapy including etoposide, ifosfamide, and cisplatin with six cycles. The headache completely disappeared after the GKS, but the patients developed left superior oblique palsy instead. A follow-up orbital MRI was performed three months after the GKS, and showed decreased volume of the metastatic orbital leiomyosarcoma.
(a) Transverse, coronal T1-weighted fat-suppressed contrast-enhanced MR images reveal an enhancing mass (22 mm) involving the left superior oblique muscle. (b) Follow-up contrast-enhanced MR images demonstrate decreased volume (15 mm) of the metastatic lesion from the leiomyosarcoma to the left superior oblique muscle.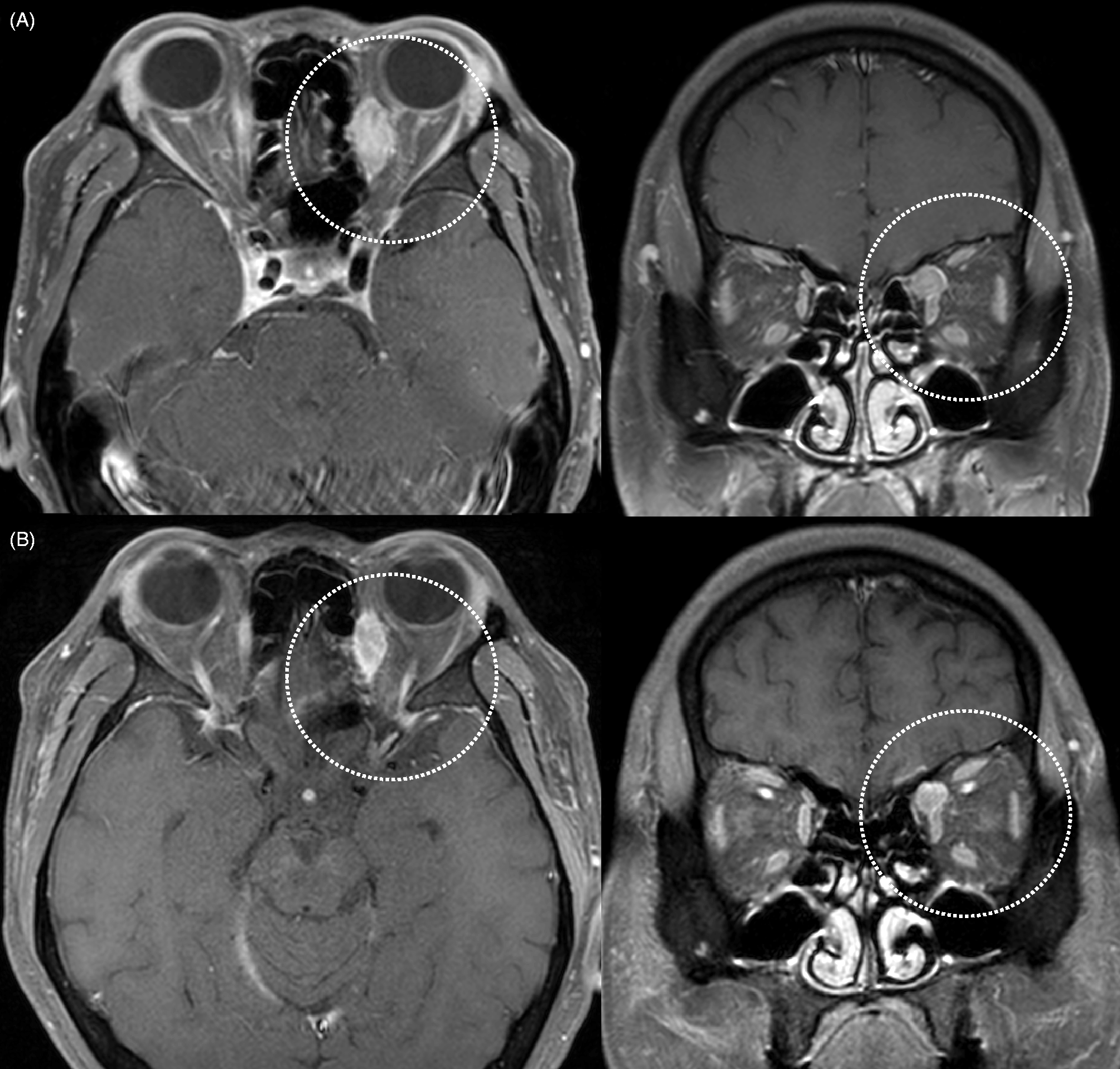
Discussion
Our case is the first report of orbital metastatic leiomyosarcoma involving the superior oblique muscle, mimicking a chronic PH-like headache without oculomotor symptoms and neurological deficits. Diagnoses of headache that can be associated with orbital pain such as CH, SUNCT syndrome, HC, and ocular inflammatory disorder including trochleitis were ruled out according to the third edition of the International Classification of Headache Disorders (ICHD-3 beta). According to previous reports, a considerable proportion of secondary TACs do not satisfy all the ICHD-3 beta criteria (2,4,5). Of the three case studies of patients with PH-like headaches (2), one who had a gangliocytoma growing within the sella turcica fully met the diagnostic criteria, while the other two were missing one of the features required to fulfill all the criteria for the lack of indomethacin trial and short duration of 40–50 seconds (6–8). In a review of chronic PH reported by Trucco et al., six of 18 patients met all the diagnostic criteria of PH; there were four patients for whom there was not enough information to make a diagnosis (4). Therefore, our study highlighted the importance of ruling out secondary etiology, which requires careful evaluation if the headache characteristics do not qualify to be diagnosed as PH (so-called probable PH) (5).
Neuroimaging is essential to exclude secondary etiology of PH. In addition, the possibility of intraorbital lesions must be considered in patients with PH. To the best of our knowledge, only one case with an orbital cavernous hemangioma showing a visible swelling in the right eye, and mimicking cluster-like headache without periodicity, has been reported (2). Interestingly, the lesion is located in the medial orbital fossa and involves the superior oblique muscle in our case, but no focal neurological signs, such as visual disturbance, diplopia, and restriction of eye movement, were observed. Moreover, the baseline non-contrast enhanced brain MRI with 5.0 mm thick slices at admission was unremarkable. It is possible that the absence of contrast and thickness of the slices did not allow the small leiomyosarcoma to be detected. Baseline MRI with contrast enhancement is essential in patients with headache mimicking PH even without neurological deficits, and repeated MRI might be needed if clinically indicated.
Leiomyosarcomas, which are characterized by smooth muscle differentiation, can be found in the retroperitoneum or any location where there is a vein. Hematogenous spread predominantly to the lung is the most common spread pattern (9). Surgical resection could be tried in patients who have isolated pulmonary metastatic disease. However, in a majority of the patients with metastatic disease, chemotherapy is administered with a palliative intent. Among the metastatic diseases, metastatic orbital leiomyosarcoma has been published very rarely, and only a few cases related to this topic have been reported in the literature (3). To our knowledge, this is the first report of an orbital metastatic leiomyosarcoma of a lower extremity mimicking chronic PH-like headache.
The disappearance of headache after the removal of the associated condition is the most important thing while diagnosing symptomatic headache. The remission of headache after gamma knife surgery suggested an association between orbital leiomyosarcoma and PH-like headache. We hypothesize that the mass had an effect over the superior oblique muscle, thereby altering the neural connections of the orbit. Anastomoses between the trochlear nerve and the orbital nerve branches such as lacrimal, frontal, supratrochlear, nasociliary, or infratrochlear nerves relay sensory input via the trigeminal system, and adjust their periodicity via the trigeminohypothalamic tract (10). Owing to the reflex activation of the parasympathetic outflow from the superior salivatory nucleus, predominantly through the SPG, headache mimicking PH could occur with parasympathetic symptoms ipsilateral to pain (11,12). In this case, the SPG block was found to provide transient pain relief by blocking the sensory connection between the orbital nerve branches of the SPG and the trigeminal nerve (11). The leiomyosarcoma in the superior oblique muscle mimicking chronic PH-like headache without neurological deficits is a rare occurrence that warrants further pathophysiological investigation.
Conclusion
Neuroimaging is essential to exclude the secondary etiology of TACs. In addition, the possibility of an intraorbital lesion must be considered in patients with headache mimicking PH. It is important to consider symptomatic causes if the headache characteristics do not meet the diagnostic requirements. We suggest that baseline MRI with contrast enhancement is essential in patients with PH, even in the absence of neurological deficits, and repeated MRI might be needed if clinically indicated.
Footnotes
Clinical implications
Suspicion of a secondary cause should be raised if the headache characteristics do not qualify to be diagnosed as paroxysmal hemicrania.
Baseline MRI with contrast enhancement is essential, and possible intraorbital lesion should be considered in patients with headache mimicking paroxysmal hemicrania. Repeated MRI might be needed if clinically indicated.
Abbreviations
TACs, trigeminal autonomic cephalalgias; CH, cluster headache; PH, paroxysmal hemicrania; SUNCT syndrome, short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing; MRI, magnetic resonance imaging; ESR, erythrocyte sedimentation rate; SPG, sphenopalatine ganglion; PET-CT, Positron emission tomography-computed tomography; ICHD-3 beta, third edition of the International Classification of Headache Disorders.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.