
Abstract
Background
To date we are lacking prospective data for field testing of ICHD-3 beta criteria for periictal headache (PIH).
Methods
Patients with focal epilepsy diagnosed by means of prolonged video-EEG monitoring completed a paper-pencil diary for three months and recorded seizures and headaches on a daily basis. According to ICHD-3 beta, we classified PIH, defined as headache present on a day with at least one seizure, as “7.6 headache related to epileptic seizure”, “7.6.1 hemicrania epileptica” or “7.6.2 postictal headache”. In addition, we compared the ICHD-3 beta diagnoses to the diagnoses according to ICHD-2.
Results
Thirty two patients completed the diary. Data analysis included 2,668 patient days, 300 seizures and 37 episodes of PIH. Two of these episodes (5.4%) were classified as headache related to seizure, three (8.1%) fulfilled both the criteria of headache related to seizure and hemicrania epileptica and four (10.8%) were postictal headaches. Twenty eight episodes (75.7%) did not fulfil any of the ICHD-3 beta criteria of seizure-related headaches, mostly because headache onset was before seizure onset. Applying ICHD-2 criteria allowed only one single episode of PIH to be classified as postictal headache.
Discussion
Our study is the first to present prospective field testing data of the ICHD-3 beta criteria for three types of seizure-related headaches. The majority of PIH episodes do not fulfil any of these criteria. One quarter can be classified according to ICHD-3 beta, whereas purely clinical diagnosis of PIH is markedly restricted in ICHD-2 because of mandatory electroencephalographic evidence.
Introduction
Periictal headache (PIH), defined as “headache with a clear-cut temporal relationship to seizures”, occurs in 28–47% of patients with epilepsy according to retrospective surveys (1–4). A number of studies further distinguished between preictal, ictal and postictal headache, and suggest that postictal headache is the most frequent type and preictal the rarest (1,2,5–7). In addition, (post)ictal headache seems to be more common in generalized tonic-clonic compared to focal seizures (2,5,8–10). The only prospective study on this topic covering an observational period of three months found PIH in only 5% of the patients, 20% experienced interictal headache (IIH), and 2.2% reported PIH as well as IIH (11).
According to ICHD-3 beta12, PIH is classified as 7.6 “headache related to epileptic seizure”, 7.6.1 “hemicrania epileptica” and 7.6.2 “postictal headache”. ICHD-2 (13) provides criteria only for the two latter. With respect to hemicrania epileptica, simultaneous onset of headache and seizure is required both in ICHD-3 beta and ICHD-2. Synchronous EEG registration demonstrating epileptic discharges ipsilateral to the headache is mandatory in ICHD-2, whereas ICHD-3 beta allows diagnosis also if headache improves immediately after the seizure has terminated. In addition, headache characteristics are not specified in ICHD-3 beta, whereas migrainous features are required in ICHD-2. Similarly, features of tension-type headache (TTH) or migraine required for diagnosing postictal headache according to ICHD-2 have been deleted in ICHD-3 beta. Onset of postictal headache within three hours and resolution within 72 hours after the seizure are mandatory both in ICHD-3 beta and ICHD-2. In contrast to the studies cited above, preictal headache is not included in ICHD.
In previous studies, PIH has not been systematically classified according to ICHD-2 (13), but its criteria have been used for classifying PIH as migraine or TTH. ICHD-3 beta (12) criteria of seizure-related headaches have not at all been tested formally. Therefore, we performed a prospective diary study in patients with focal epilepsy to conduct field testing (14), assess the proportion of headaches fulfilling the new diagnostic criteria, and compare ICHD-3 beta diagnoses to those of ICHD-2.
Methods
Patients
We screened all consecutive patients (n = 883) admitted to the epilepsy monitoring unit of the Department of Neurology, Medical University of Vienna, between January 2006 and June 2012 for eligibility. Inclusion criteria comprised 1) an age of 18 to 65 years, 2) a diagnosis of focal epilepsy (15) based on a previous prolonged video-EEG monitoring and 3) the patient’s ability to fill out the study questionnaires and the headache and seizure diary. Exclusion criteria were 1) a diagnosis of idiopathic generalized epilepsy or psychogenic non-epileptic seizures, 2) acute symptomatic seizures due to e.g. stroke, encephalitis or tumour, 3) medication overuse headache or any other secondary headaches, 4) previous or current substance abuse, 5) moderate-to-severe mental retardation and 6) a severe psychiatric disorder. We invited all eligible patients personally, by phone, or by mail to participate in this study. Detailed reasons for the exclusion and non-participation of patients are given in Figure 1.
Study flow chart.
Methods
At baseline, all patients underwent a semi-structured interview covering demographic data, years since the onset of epilepsy and frequency of seizures and headaches within the previous three months. In addition, the patients completed Beck’s Depression Inventory (BDI) (16) and Beck’s Anxiety Inventory (BAI) (17). Finally, they received a 90-day seizure and headache diary, including instructions on how to use it. The patients had to fill in the diary every morning after breakfast and they had to record the absence and presence of seizures and headaches during the previous 24 hours. They had to give the number and types of seizures (focal vs. secondary generalized) and they had to give all headache characteristics required for diagnosing migraine without aura and tension-type headache (TTH) according to ICHD-3 beta. Furthermore, the patients had to record the exact time of onset and termination of each epileptic seizure and headache episode. Thus, the information in the diaries provided all headache features required for classifying PIH according to ICHD-3 beta and ICHD-2. Diagnosis of hemicrania epileptica was limited by the fact that information about simultaneous onset of headache and electroencephalographically-demonstrated ipsilateral epileptic discharges was not available. We defined PIH as headache present on a day with at least one seizure and applied ICHD-3 beta and ICHD-2 criteria to all headaches meeting this definition. Interictal headache (IIH) was defined as headache on a day without a seizure.
The study protocol was approved by the ethics committee of the Medical University of Vienna. Written informed consent was obtained from all participating patients.
Data analysis
All computations were performed using SPSS statistical software, Version 20.0. Demographic and other patient-related data are given as percentages or mean ± standard deviation and/or median and first to third quartile (interquartile range, IQR), if applicable. Comparisons of means were carried out using the student’s t-test (normal distribution) or the Mann-Whitney U-test (non-normal distribution). Correlations were calculated using Pearson’s (normal distribution) or Spearman’s (non-normal distribution) coefficients. To determine predictors of PIH logistic regression, analysis was performed with PIH as the dependent variable and the number of seizures and headache days at baseline, as well as BDI and BAI scores as independent variables. The level of significance was set at <0.05.
Results
Thirty two patients (17 female, age 40.4 ± 12.7 years, body mass index 24.1 ± 4.3) completed the headache and seizure diary. Six (19%) patients were diagnosed with frontal lobe epilepsy (FLE), 14 (44%) with temporal lobe epilepsy (TLE), one (3%) with parietal lobe epilepsy, two (6%) with occipital lobe epilepsy and nine (28%) with focal epilepsy, not further classified. Patients suffered from epilepsy for a mean of 18.3 ± 13.3 years. The mean number of seizures in the three months prior to study inclusion was 10.9 ± 22.6, median 2.5 (IQR 0–10). The mean number of antiepileptic drugs taken at study inclusion was 1.6 ± 0.8. Headaches had occurred for 8.4 ± 13.1, median 4 (IQR 0–10) years. The mean number of headache days in the three months prior to study inclusion was 7.2 ± 12.3, median 2.5 (IQR 0–7.8). The mean BDI score was 6.0 ± 6.5 and the mean BAI score was 7.7 ± 9.4.
The analysis of diary data was based on 2,668 patient days, with a mean of 84 ± 19 days per patient.
Seizures
Thirty two patients recorded a total of 244 days with at least one epileptic seizure. The total number of seizures was 300 (263 focal seizures, 37 secondary generalized tonic-clonic seizures). The median number of seizures per patient was two (range 0–57) and the median number of days with at least one seizure was two (range 1–57). Seven patients (22%) were free of seizures during the observational period. Among patients with at least one seizure, the median number of seizures per patient was four (range 1–57) and the median number of days with at least one seizure was four (range 1–57). Among patients with PIH (n = 8), the median number of PIH episodes per patient was two (range 1–18).
Headaches
In the entire group of 32 patients, eight (25%) subjects recorded at least one episode of PIH and 22 (69%) at least one episode of IIH. PIH was present on 37 (15%) of 246 days with at least one epileptic seizure and accompanied 37 (12%) of 300 seizures. With respect to the seizure type, 73% of the PIH episodes appeared in relation to focal seizures and 27% were related to secondary generalized tonic-clonic seizures. IIH was present on 325 (13%) days without a seizure. None of the patients had PIH exclusively, 14 (44%) had IIH exclusively, and eight (25%) had both PIH and IIH.
Characteristics of patients with and without PIH according to prospective diary recordings.

Note: p-values in bold are statistically significant.
Classification of PIH according to ICHD
Three of the eight patients with PIH had at least one episode fulfilling ICHD-3 beta 7.6, 7.6.1 and/or 7.6.2 criteria. ICHD-3 beta allowed classifying nine (24.3%) of the PIH episodes, whereas 28 (75.7%) episodes did not fulfil any of the ICHD-3 beta criteria for PIH. Hence, the incidence of ICHD-3 beta PIH was 3.6% (i.e. nine of 246 days with a documented seizure). In detail, five PIH episodes could be classified as headache related to seizure, three as hemicrania epileptica, and four as postictal headache, including three episodes fulfilling both the criteria of headache related to seizure and hemicrania epileptica. Of the 28 PIH episodes that did not meet ICHD-3 beta criteria, 25 (89%) started 4.1 ± 3.6 hours (range 5 min – 9.5 hours) before seizure onset, thus being preictal headaches, and only one (4%) of these headache episodes remitted immediately after the seizure had terminated.
One patient (No. 17, Figure 2) documented 18 (49%) PIH attacks (two classified according to ICHD-3 beta as seizure-related headaches, 14 preictal and two postictal headaches, albeit not classifiable according to ICHD-3 beta or ICHD-2). Excluding this outlier increased the proportion of PIH episodes classifiable according to ICHD-3 beta from 24.3% to 37%.
Number of individual PIH episodes. Each column shows the number of PIH episodes during the three-month prospective observation for each patient.
Applying ICHD-2 criteria allowed identification of only one single episode of PIH that was classified as postictal headache. This finding is explained by the fact that headache related to seizure (7.6) is not at all included in ICHD-2, hemicrania epileptica could not be diagnosed because of the mandatory EEG criterion and three of the four headaches classified as postictal headache according to ICHD-3 beta did not fulfil ICHD-2 criterion A, i.e., the mandatory headache features.
According to ICHD-3 beta (12) one episode of headache related to seizure could also be classified as migraine without aura and another as TTH, and one episode of postictal headache also fulfilled the criteria of TTH, whereas the remaining six headache episodes could not be classified as (probable) migraine or (probable) TTH. Among 28 episodes of PIH not fulfilling ICHD-3 beta 7.6 criteria, two (7%) were classified as migraine without aura, five (18%) as probable migraine, eight (31%) as TTH, and two (7%) as probable TTH, whereas 11 (39%) did not fulfil any of these criteria. In total, 60.7% of the preictal headaches, as compared to 33.3 % of the seizure-related headaches according to ICHD-3 beta, also fulfilled the criteria of migraine or tension-type headache.
Classification of IIH according to ICHD-3 beta (12)
Classification of 112 IIH episodes in eight patients with focal epilepsy.

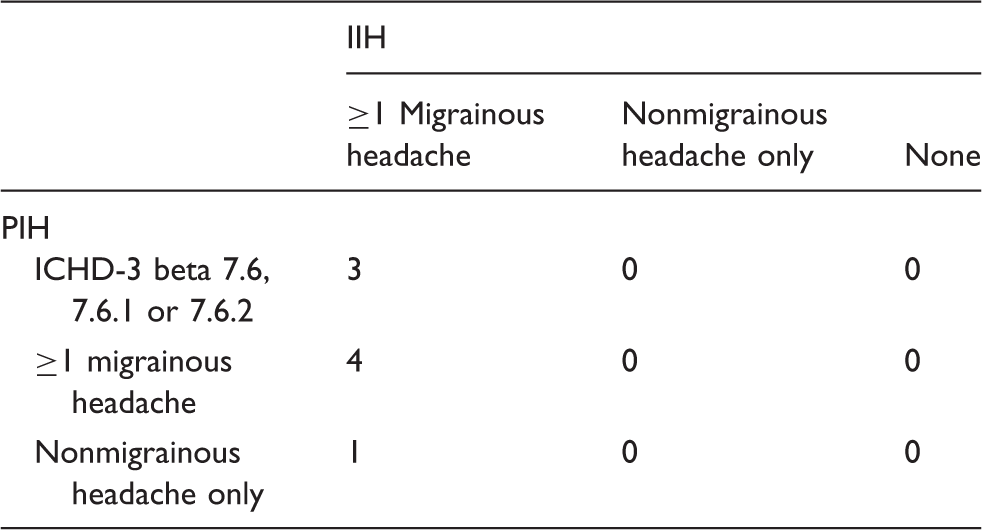
Relation between IIH and PIH in 8 patients with focal epilepsy.
Discussion
Our study is the first to present field testing data of the ICHD-3 beta (12) criteria of PIH in patients with focal epilepsy. The incidence of PIH, defined as headache on a day with a seizure, was 15%, and the incidence of ICHD-3 beta seizure-related headaches was 3.6%. Out of a total of 37 PIH episodes, only 24% fulfilled the ICHD-3 beta 7.6 criteria.
The incidence of PIH in our sample lies in between the rates reported in the only other prospective study (10%) (11) and a more recent retrospective study (35.3%) (5). In our study, the patients with PIH were predominantly female and reported more headache days and seizures at baseline than patients without PIH, but only the number of seizures at baseline significantly predicted PIH. Duchaczek et al. found low age at epilepsy onset, antiepileptic polytherapy and generalized tonic-clonic seizures to be predictors of PIH (5), but these authors did not include headache days or the number of seizures at baseline, or psychometric variables like BDI or BAI, into their analysis. Although our sample of patients with PIH is small, our results may serve as another part of the puzzle to identify patients who suffer from PIH. Particularly, patients with higher seizure frequency should routinely be asked about the occurrence and severity of PIH.
PIH classified according to ICHD has never been examined before. Using purely clinical assessment allowed classification of only one single PIH episode (2.7%) according to ICHD-2 (13). This proportion increased to nine (24.3%) in ICHD-3 beta. The increase in sensitivity included all episodes of seizure-related headache and hemicrania epileptica and three of four cases of postictal headache. The increase is explained by 1) criteria for seizure-related headache newly added in ICHD-3 beta, 2) the deletion of headache features for hemicrania epileptica and postictal headache, and 3) the addition of a clinical feature as an alternative to mandatory electroencephalographic evidence in hemicrania epileptica.
By obtaining diary data on PIH and IIH we were able to show that PIH that were classified as 7.6, 7.6.1 or 7.6.2 were not preceded or followed by migrainous or non-migrainous IIH within 24 hours. Intriguingly, all patients with PIH suffered from IIH, and reported at least one migrainous IIH attack.
The strength of this study is its prospective design using detailed daily diaries. Limitations are the small total sample size and the fact that only a minority of the patients reported PIH. In addition, patient recruitment in a tertiary centre does not allow generalizing the findings to all patients with focal epilepsy.
In conclusion, our study is the first to present prospective field testing data of the ICHD-3 beta criteria for three types of seizure-related headaches. The majority of PIH episodes do not fulfil any of these criteria. One quarter can be classified according to ICHD-3 beta, whereas purely clinical diagnosis of PIH is markedly restricted in ICHD-2 because of the mandatory electroencephalographic evidence. Needless to say, these findings have to be replicated in a larger sample of epilepsy patients.
Clinical implications
First study to present prospective field testing data of the ICHD-3 beta criteria for three types of seizure-related headaches. One quarter of periictal headaches can be classified according to ICHD-3 beta. Purely clinical diagnosis of PIH is markedly restricted in ICHD-2, because of mandatory electroencephalographic evidence
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.