
Abstract
Migraine-like features sometimes characterize the headache that follows epileptic seizure (postictal headache, PIH). We compared patients with different types of epilepsy to investigate the association between migraine-like PIH and seizure type. Subjects comprised 364 patients with partial epilepsy. Epilepsy types were temporal lobe epilepsy (TLE, n = 177), frontal lobe epilepsy (FLE, n = 116), and occipital lobe epilepsy (OLE, n = 71). Patients participated in a structured interview pertaining to PIH as well as interictal headache and family history of migraine. Headaches were classified according to the International Headache Society criteria, which was modified for this study. Forty percent had PIH and 26% of these patients had migraine-like PIH. Migraine-like PIH occurred significantly more often in cases of TLE and OLE than in cases of FLE. In addition, the incidence of interictal migraine headache was significantly higher in patients with migraine-like PIH. These results suggest that migraine-like PIH is related to particular regions of epileptogenic focus and that susceptibility to migraine headache predisposes to migraine-like PIH.
Keywords
Introduction
Patients with epilepsy often exhibit headache during the postictal period, but the pathophysiology of such headaches remains unclear. Post-ictal headache (PIH) can be of the migraine type, tension type or unclassified type of headache (1–3). Several researchers (3–6) have pointed out that the PIH has similar symptoms to migraine such as pounding pain and accompanying nausea, photophobia and phonophobia in a significant proportion of patients (41–56%). In addition, an effect of antimigraine drugs on PIH has been found in some cases (7, 8). Previous reports have suggested that migraine type headaches often occur during postictal periods in some epilepsy syndromes such as occipital lobe epilepsy (8–11). These findings suggest that migraine-like PIH and migraine have underlying mechanism in common, but the mechanisms themselves have not been clarified. Investigation of PIH with characteristics of migraine would contribute to understanding of the relation between migraine and migraine-like PIH. However, there have been very few studies on migraine-like PIH. We compared epilepsy patients with migraine-like PIH to those with other PIH and no PIH to find possible factors associated with migraine-like PIH.
Methods
Subjects comprised 364 patients(163 males and 201 females) with temporal lobe epilepsy (TLE), frontal lobe epilepsy (FLE) or occipital lobe epilepsy (OLE). All subjects were being treated at one of seven adult epilepsy clinics in Japan. Epilepsy type was determined according to the International League Against Epilepsy criteria (12) on the basis of clinical symptoms, electroencephalography, and neuroimaging finding such as computed tomography or magnetic resonance imaging (MRI). Although neuroimaging study findings were available in all cases, we did not analyse precise structural abnormalities because of differences in the specificities of the devices and scanning conditions at each institution. Patients were classified as symptomatic or cryptogenic, whereas idiopathic type was not included. No patient with progressive brain disease or recent brain injury was included. We defined epigastric ascending sensations and elementary visual signs as necessary for the diagnosis of TLE and OLE, respectively, as the initial seizure symptom. Motor symptoms or gestural automatisms without prolonged postictal confusions were required for the diagnosis of FLE. Patients who matched the above criteria for TLE, FLE or OLE were consecutively asked to participate in the study. Informed consent was obtained from each subject.
The epilepsy types were as follows: 177 patients with TLE, 116 patients with FLE, and 71 patients with OLE. Patients ranged in age from 12 to 81 years (mean 37.2 years). Duration of epilepsy and age at onset of epilepsy was 0–56 years (mean 21.9 years) and 0–56 years (mean 15.3 years), respectively.
The data obtained for each patient included seizure type, seizure frequency, and number of antiepileptic drugs (AEDs) taken. Seizure types consisted of 109 patients with simple partial seizures (SPS) and/or complex partial seizures (CPS), and 255 patients with SPS and/or CPS combined with secondarily generalized tonic-clonic seizures (SGTC). The distribution of seizure frequency was 21 patients with daily seizures, 59 patients with weekly seizures, 123 patients with monthly seizures and 161 patients with yearly seizures or less frequent. Number of AEDs ranged 0–5 (mean 1.9).
PIH was defined as any headache occurring within 30 min after seizure. PIH was further classified according to the diagnostic criteria of the International Headache Society (IHS) (13). In this study, we used the modified criteria that excluded the limit of the duration of headache because the headaches in some patients matched the criteria for migraine without aura except that their durations were shorter. These headaches were often described as lasting for less than four hours. However, since most patients had been treated for both epilepsy and migraine symptoms, it was difficult to determine the specific duration of PIH. Therefore, we considered these PIHs as migraines without aura. Other types of PIH that did not meet the IHS migraine criteria were classified as other PIH.
Principal investigators of each institution conducted a structured interview with each subject using a standardized questionnaire that had been administered in our previous studies (5, 14, 15). The questionnaire addressed characteristics of the headache pain, the duration and severity of PIH, and accompanying symptoms such as nausea/vomiting, photophobia or photophobia. Subjects were asked if they had any headaches independent of seizure (interictal headache) about the frequency of those headaches, characteristics of the pain, the severity and duration of those headaches, and accompanying symptoms. Then we classified interictal headache as migraine or other headache in accordance with the IHS criteria. A family history of migraine in first-degree relatives was also inquired about.
For data analyses, patients with migraine-like headache were categorized as migraine-like PIH group and patients with other headaches as other PIH group. We regarded patients without PIH as controls for the statistical analyses. One-way analysis of variance (ANOVA) was used for lineal data. Post hoc pairwise multiple comparisons and range tests were carried out with the Dunnett's test (16) because the Levene test indicated unequal variances across groups. Kruskal–Wallis test was used for comparison of seizure frequency. The χ2 test (contingency table analysis) was used for categorical data. To identify special conditions responsible for significant χ2 values in the n × m contingency table analysis, the expected number (EN) of patients and adjusted standardized residual (ASR) were computed for each cell (17). In accordance with a normal standard deviation, the absolute value of the ASR (z score) was used to identify cells that varied markedly from independence (i.e. z > 1.96 for P < 0.05). P-values < 0.05 were taken to be significant. All statistical analyses were performed with SPSS ver.9.0.
Results
One hundred and forty-seven patients of the 364 (40.4%) subjects experienced PIH. Of these 147 patients, 38 (25.9% PIH patients, 10.4% total patients) fulfilled the modified IHS criteria for migraine without aura.
Demographic and clinical features of the three study groups are shown on Table 1. There were no significant differences in sex, age at onset, number of AEDs, family history of migraine, duration of epilepsy and seizure frequency between the three groups. Patients with both migraine-like and other PIH were significantly younger than patients without PIH were (P = 0.008). However, there was no significant difference between patients with migraine-like PIH and those with other PIH. With regard to seizure type, SGTC was significantly associated with other PIH, but not with migraine-like PIH (P = 0.000). Other PIH occurred at a significantly higher frequency in patients with SGTC (n = 90, EN = 76.4, ASR = 3.4, P = 0.001), whereas patients without SGTC showed PIH less frequently (n = 82, EN = 65.0, ASR = 4.0, P = 0.000). Epilepsy type was significantly associated with PIH (P = 0.000, Table 2). Patients with TLE showed no PIH more frequently (n = 120, EN = 105.5, ASR = 3.1, P = 0.002) and other PIH less frequently (n = 39, EN = 53, ASR =−3.2, P = 0.001). Patients with FLE showed migraine-like PIH less frequently (n = 6, EN = 12.1, ASR =−2.2, P = 0.028). Patients with OLE showed other PIH (n = 29, EN = 21.3, ASR = 2.2, P = 0.028) and migraine-like PIH more frequently (n = 14, EN = 7.4, ASR = 2.8, P= 0.005).
Comparison of demographic and clinical factors between postictal headache with and without migraine-like features

AED, antiepileptic drug; TLE, temporal lobe epilepsy; FLE, frontal lobe epilepsy; OLE, occipital lobe epilepsy; SGTC, secondarily generalized tonic clonic seizure; D, daily; W, weekly; M, monthly; Y, yearly or less.
Association between postictal headache and epilepsy type
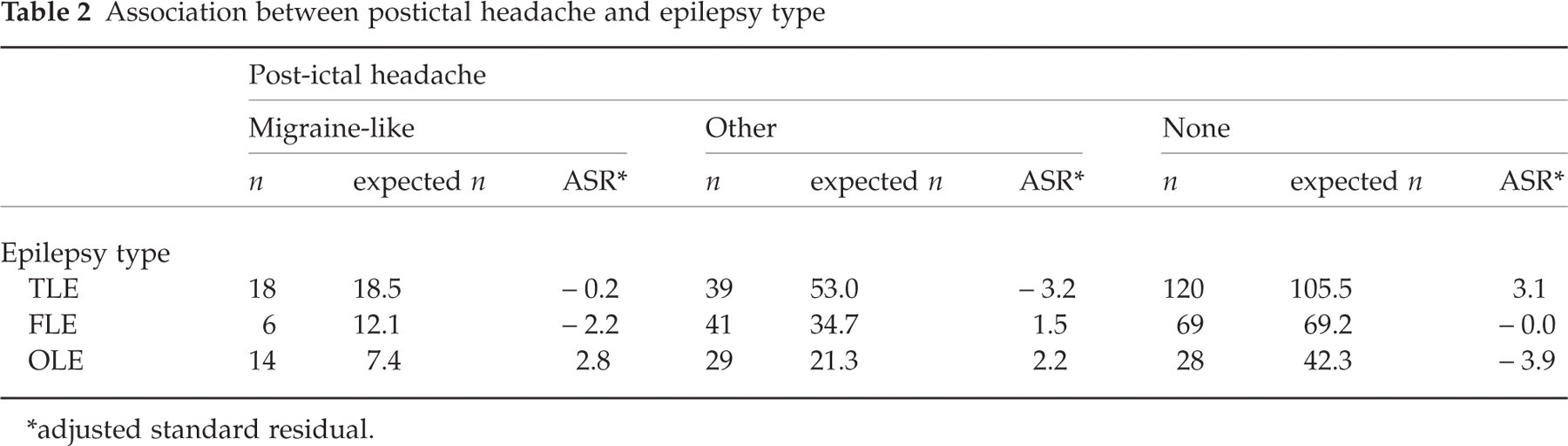
∗adjusted standard residual.
Interictal headaches were observed in 182 patients (50.0%). Of these, 29 patients (15.9% of patients with interictal headache, 8.0% of the total patients) had migraine with or without aura in accordance with the IHS criteria. There was a significant correlation between PIH and interictal headache (χ2 = 15.0, P = 0.005, Table 3). Subsequent residual analysis showed that patients with migraine-like PIH had interictal migraine more frequently (n = 9, EN = 3.0, ASR = 3.8, P = 0.000) and that patients without PIH had interictal migraine less frequently (n = 12, EN = 17.3, ASR =−2.1, P = 0.036).
Association between postictal and interictal headache
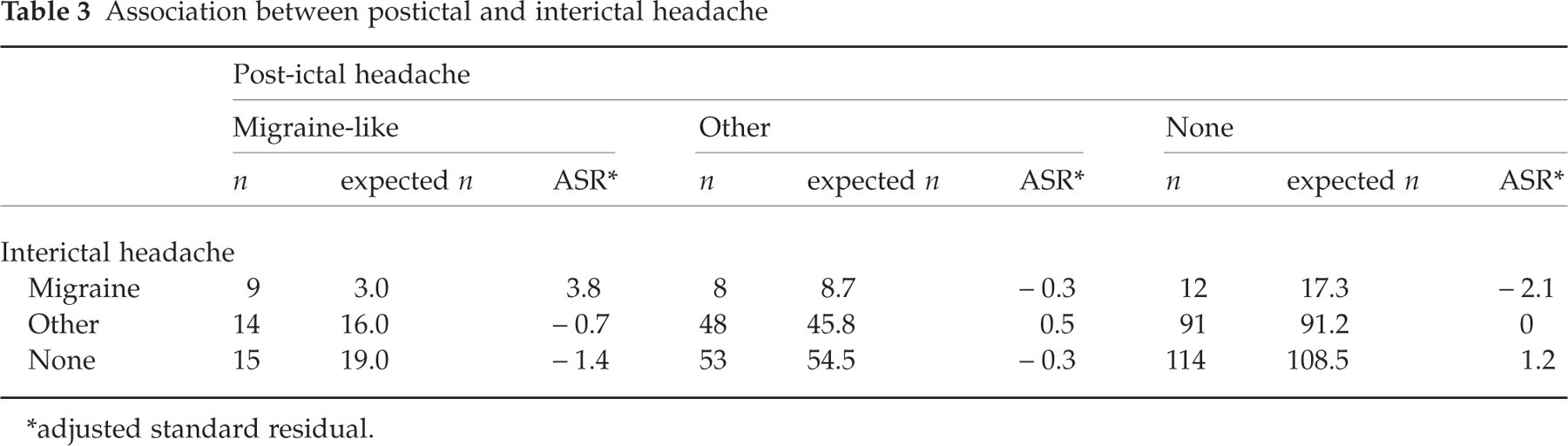
∗adjusted standard residual.
Discussion
Forty percent of our study population with partial epilepsy exhibited PIH. Migraine-like PIH occurred in 10% of the total study population and in 26% of patients with PIH. Leniger et al. (3) reported that out of 341 patients with epilepsy 115 patients (34%) had seizure-associated headache and that 64 patients (56% of patients with seizure-associated headache, 19% of total patients) complained about migraine-like seizure-associated headache. In other reports (4–6), 41–53% of patients with PIH exhibited migraine-like headache. The lower frequency of migraine-like PIH in our study patients than that in other studies is likely due to the following: Our sample was restricted to patients with TLE, FLE and OLE, whereas other studies included various types of epilepsy in addition to these three types. Thus there seemed to be differences in the distribution of epilepsy type between the samples studied. Moreover, some of our patients were taking higher dose of sodium valproate and zonisamide that could reduce migraine as well as seizures, since sodium valproate has proven prophylactic effects on migraine (18–20). Zonisamide has also been suggested to be useful (20).
Demographic features showed that patients with both migraine-like and other PIH were younger than those without PIH. The relation between PIH and age has not been investigated in other studies. Although it would be difficult to draw conclusions from the present data, possible explanation could be a decrease of PIH with age. More extensive epidemiological and longitudinal studies would be needed to determine the relation between PIH and age.
With regard to other demographic factors, there was no difference between the two PIH groups and the control group. Likewise, Leniger et al. (3) showed no differences in sex and family history of migraine between patients with migraine-like and other PIH. In general, women are more susceptible than men to migraine: Caucasians, 15.3–25% in women and 5.9–8.6% in men (21–24), while Asians, 9.2–12.9% in women and 3.6–4.8% in men (24, 25). In contrast, there seems to be no sex difference in the prevalence of migraine-like PIH. This suggests that the occurrence of migraine-like PIH depends on special conditions in addition to the pathophysiology of migraine.
The incidence of PIH was significantly higher in patients with SGTC than in those without as a number of studies have shown (2–5, 15, 26). However, SGTC was more frequently followed by other PIH than migraine-like PIH. This finding was compatible with other reported findings (2, 3). The reason for this remains unclear, but one possible explanation is that generalization of seizure discharge may induce some other pathophysiological changes within the whole brain structure. Duration of epilepsy and seizure frequency was not related to PIH. This suggests that neither prolonged course nor severity of epilepsy is likely to have an impact on PIH.
Our most important finding was that the occurrence of migraine-like PIH was significantly related to the region of epileptogenic focus. OLE was strongly correlated with migraine-like PIH. The occipital lobe is deemed to be the brain structure most responsible for the development of migraine (27, 28). Although PIH occurred at a lower frequency in patients with TLE, migraine-like PIH occurred comparatively higher than other PIH did. The posterior temporal cortices locate close to the occipital cortices and the anatomic connections between the mesial temporal structures and occipital lobe are abundant (29, 30). When both the temporal lobes and occipital lobes are firing, the structures related to migraine symptoms could become quickly involved. According to the cortical spreading depression (CSD) theory (27), neural activity occurring in the occipital area spreads forward across the cortical surface and discontinues at the Sylvian fissure. Subsequent reduction in cortical blood flow is likely associated with migraine (31). Recent studies with new methods such as positron-emission tomography or functional MRI have confirmed the changes in blood flow during migraine attack (32, 33). It is very likely that CSD plays an important role in the induction of migraine-like headache in certain patients with epilepsy. Bowyer et al. (34) conducted magnetoencephalographical study during migraine aura and observed neuroelectrical activity in not only the occipital area but also in the temporal area. This finding may support our hypothesis that there is a link between migraine-like PIH and CSD in patients with OLE and TLE. In contrast, we found that only a few patients with FLE exhibited migraine-like PIH. The frontal cortices are both anatomically and functionally distant from the occipital cortices. Therefore CSD may be less associated with the occurrence of PIH in patients with FLE than in those with OLE or TLE. Measurements of neural activity and cerebral blood flow following epileptic seizure would contribute to clarifying the pathophysiology of PIH.
Patients with migraine-like PIH showed a higher frequency of interictal migraine in comparison to patients with other PIH or no PIH. Moreover, patients with other PIH did not show a significant relation to any type of interictal headache. Leniger et al. (3) found a relation between migraine-like seizure-associated headache and a history of migraine, which is compatible with our findings. Susceptibility to migraine headache may be a factor predisposing to migraine-like PIH.
The present study has several methodological limitations. Though our study involved a comparatively large number of patients recruited from multiple institutions, the characteristics of patients are not representative of those of the general population with partial epilepsy. Patients visiting the special epilepsy clinic tend to suffer from epilepsy complicating cerebral function. Also, the number of patients with OLE was insufficient for subsequent multiple analysis. In addition, structural abnormalities were not factored into our analysis because of differences in the specificities of neuroimaging methods between institutions. Various neuropathological conditions were likely represented in our subject group.
In conclusion, we did find a relation between particular epileptogenic regions and migraine-like PIH that can be considered as clinical evidence of CSD. The pathophysiology of PIH may be similar to that of migraine except in some aspects. Further studies with a larger sample are needed to confirm our findings.