
Abstract
Postictal headache (PIH), although it occurs in 34–59% of epilepsy patients, has not been adequately studied. This study aims to describe clinical characteristics and associations of PIH in generalised epilepsy in a South African tertiary neurology clinic.
Methods: Two-hundred consecutive adults with generalised epilepsy underwent semi-structured interviews, dividing them into study (with PIH) and control patients (no PIH), and data was statistically analysed.
Results: PIH occurred in 104/200, with 63% having headache after every seizure. Pain duration was 4–24 hours in 43% and pain intensity severe in 55%. The criteria of the International Headache Society (2004), International Classification of Headache Disorders, second edition (ICHD-II) classified 47% as migraine, 38% tension-type and 15% unclassified (but 13% probable migaine). Self-medication occurred in 81% and interictal headache was significantly associated with PIH—present in 64% of study patients versus 5% of control patients.
Conclusion: PIH occurs commonly in generalised epilepsy, mostly as migraine headache, with interictal headache a specific risk factor. PIH is underdiagnosed and undertreated, leading to self-medication. Optimal management should be elucidated in future studies.
Introduction
Headache in relation to seizures is a well-known phenomenon, occurring prior to, during or after seizures (pre-ictal, ictal and postictal headache). Of these, the postictal form has been reported in 34–59% of patients and thus is the most common type of seizure related headache (1,2).
As an entity postictal headache (PIH) is underdiagnosed. Contributing to this problem is the fact that the International Classification of Headache Disorders (ICHD-II) (3) does not have a category for PIH and the fact that doctors treating patients with epilepsy rarely address PIH by prescribing treatment for it (4–6), even though several studies have shown that PIH has a significant impact on morbidity, independent of the effect of seizures (6,7).
The undertreatment of PIH may on one hand be due to issues directly related to seizure occurrence and control which overshadow those of the headache, and on the other hand the fact that PIH remains a poorly understood entity, with scanty data available about its clinical characteristics and optimal treatment.
The few studies which have investigated PIH have several shortcomings. Some have not made use of standardised tools like the ICHD criteria (8–10). Although the ICHD criteria do not provide a category for PIH, trying to classify this form of headache according to known types of headache may be useful in elucidating the pathophysiology of the condition. Another deficiency in the available data on PIH involves the types of epilepsy in which this condition has been investigated. Research done by Förderreuther (4) and Syversten (6), respectively, looked at the characteristics of PIH in epilepsy in general but did not differentiate clearly between different types of epilepsy. This may be an essential distinction to make because there may be a unique association between specific seizure types and PIH. Other studies have investigated PIH extensively in patients with partial epilepsy (2,5,11,12). Despite some reports finding up to 96% of PIH in patients with generalised epilepsy, no study could be found that specifically evaluated this sub-population (6). Most of the PIH studies are from developed countries and as the etiological profile (13) of epilepsy differs between developing and developed countries; this might also have an effect on the characteristics of PIH.
The aim of this study is therefore to describe the clinical characteristics of PIH in patients with generalised epilepsy in a tertiary hospital outpatient clinic of a developing country, also evaluating potential associations between PIH and demographics, seizure type, family history and medication usage.
Methods
The study had a observational, cross-sectional design. Two hundred eligible patients with generalised epilepsy were consecutively recruited from the neurology clinic at the Steve Biko Academic Hospital, a tertiary care facility in Pretoria, South Africa. These patients were divided into the study and control groups based on the presence or absence of PIH.
Patients of an age of 18 years or older had to meet the criteria for generalised epilepsy according to the International League against Epilepsy (ILEA) classification. The diagnosis of generalised epilepsy was aided by the available clinical and electro-encephalopgraphic (EEG) evidence. PIH was defined as a headache with an onset within one hour after the termination of a seizure or the regaining of consciousness. This is in correspondence with the definition used by other studies on PIH. In order to limit recall bias, patients had to have had at least one of these headaches in the preceding year.
Patients with a potential secondary cause for headache despite having epilepsy were specifically excluded from enrolment. These included patients with conditions such as intracranial tumours or progressive neurological illnesses. Also excluded was anyone who had been diagnosed with epilepsy within the previous six months, in order to prevent including subjects in the study who might have an undiagnosed cause for headache. Patients in whom a diagnosis of non-epileptic seizures was confirmed or suspected were not eligible for enrolment and the ability of patients to reliably report seizures and headache characteristics was also taken into account, thus excluding patients with mental retardation from the study.
After enrolment patients participated in a semi-structured interview conducted by the principal investigator using a data capturing sheet. Demographic information was collected regarding the age, race and gender of patients. Data about seizures included the duration of epilepsy history as well as seizure frequency. Seizures were further described as primary or secondary generalised based on existing electrophysiological and radiological tests. Classification according to tonic, clonic, absence or myoclonic seizures was also undertaken.
Further information was collected from patients reporting PIH to characterise this entity more specifically. Headache frequency was measured in terms of the percentage of seizures which were followed by PIH, and categorised as 25%, 50%, 75% or 100%. The onset of PIH was recorded according to the patient’s recall of how soon the headache started after termination of a seizure or upon regaining consciousness.
The severity of the headache was measured by the patient’s score on the Visual Analog Scale (VAS) for pain and converted into a score out of 10 (10 being the most severe pain). Further data were collected regarding localisation, accompanying symptoms and headache quality (pulsating/throbbing or pressing/tightening) and then analysed according to ICHD-II criteria. Headaches not meeting specific criteria for either migraine or tension-type headache were indicated as unclassified.
Subjects were further asked whether they experienced interictal headache. This was defined as any form of headache commencing more than 24 hours after a seizure. Data regarding the type of interictal headache were not collected.
Family data collected consisted of first-degree relatives with epilepsy or headache. The final category of information gathered pertained to medication usage. Patients indicated if they self-medicated for the pain of PIH or whether a doctor had prescribed medication. Additionally, all currently used anti-epileptic drugs (AEDs) were listed.
All patients enrolled in the study provided signed informed consent before participating in the semi-structured interview. Data were collected anonymously and are not traceable to a particular individual. The study was approved by the MMed Committee and the Research Ethics Committee of the Faculty of Health Sciences, University of Pretoria, as well as the Chief Executive Officer of the Steve Biko Academic Hospital. Statistical analysis was conducted by a biostatistician of the Medical Research Council in Pretoria. Based on previous reports (indicating the prevalence of PIH at 34–59%), with p-α set at 0.05 and a power level of 0.9, it was calculated that 200 patients should be enrolled. Data were analysed by descriptive statistics utilising mean, median, standard deviation and range as appropriate. Categorical data were compared using Pearson’s chi-square test, Kruskal-Wallis and Mantel-Haenszel (recommended if multiplicity is suspected) testing. In addition, logistics regression was used for the binary variables. STATA version 10 was employed throughout.
Results
Characteristics of postictal headache
From the total of 200 recruited patients, 104 were found to have PIH, yielding a prevalence of 52% in this population of adult patients with generalised epilepsy.
Among the subjects with PIH (N = 104), a majority of 63% (N = 65) reported experiencing headache after every seizure, in contrast to 37% (N = 39) having PIH less frequently (Figure 1).
Frequency of PIH, as measured by the percentage of seizures which are followed by a headache (e.g. the 75% category indicates that 20% of patients experience PIH in relation to 75% of their seizures).
The onset of PIH was immediate upon termination of the seizure or upon regaining consciousness in 94.2% (N = 98) of subjects. PIH lasted less than four hours in 35.6% of patients, from 4 to 24 hours in 43.3% and longer than a day in 21.1% (Figure 2). One patient reported that her headache lasted up to seven days.
Duration of postictal headache (N = 104).
It was slightly more common for PIH to localise unilaterally; this was the case in 55.8% (N = 58) of patients as opposed to 44.2% (N = 46) who experienced pain bilaterally. Topographically, frontal PIH was the most frequent (75%), followed by temporal (48.1%), parietal (21.2%) and occipital (11.5%). Some patients indicated more than one location.
The mean pain intensity of PIH as measured by the VAS was 7.06 cm (standard deviation [SD] ± 1.68). If the results are classified into mild (≤3 cm), moderate (>3 < 7 cm) and severe (≥7 cm), the majority of patients (54.8%) fall in the severe category, although the mean is on the border between moderate and severe (Figure 3). Three patients indicated a score of 10/10 on the VAS for the severity of their PIH pain.
Pain intensity of PIH as measured on the Visual Analog Scale (VAS) for pain (N = 104). Mild ≤3 cm; moderate >3 < 7 cm; severe ≥7 cm.
The quality of the pain was reported in 51% (N = 53) as pressing or tightening in nature, while 49% (N = 51) judged it to be throbbing or pulsating. Aggravation by physical activity (54.8%; N = 57), photophobia (54.8%; N = 57) and nausea (40.4%; N = 42) were the most common symptoms which accompanied PIH (Figure 4).
Symptoms accompanying postictal headache.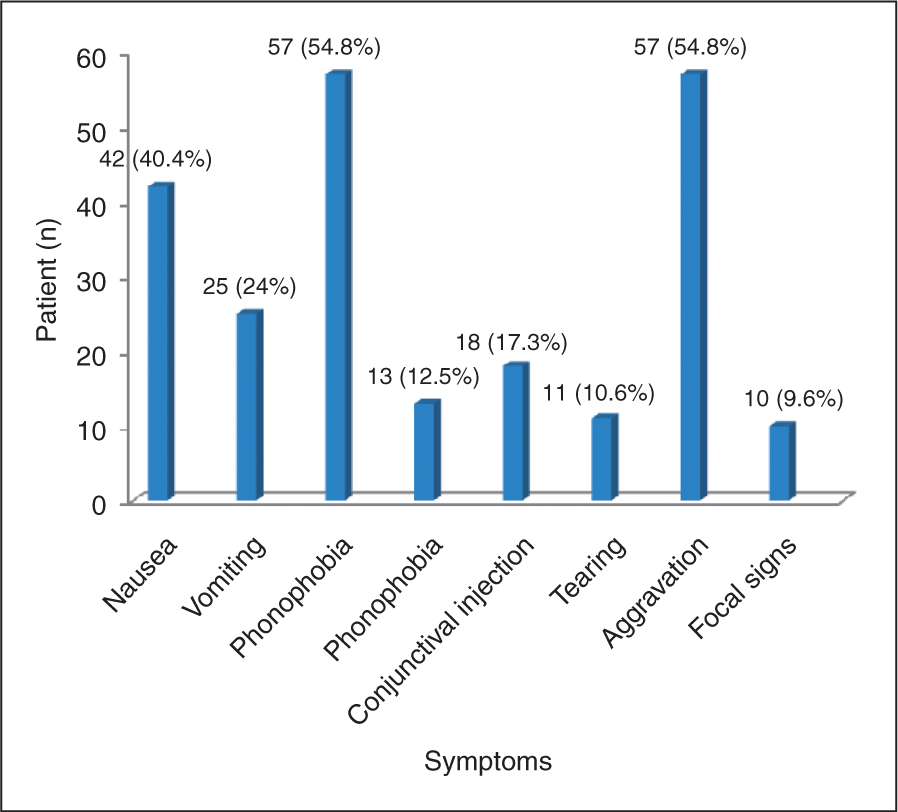
Using the ICHD-II criteria to classify the type of PIH experienced by patients, of 104 subjects, 49 had a migraine-like headache, 39 tension-type and 16 could not be classified (Figure 5). It is, however, noteworthy that of the latter 16 cases, 14 met all the criteria for migraine, except for the duration of the headache, which was stated as less than four hours. These 14 cases would therefore meet the criteria for probable migraine.
Classification of PIH according to ICHD-II criteria.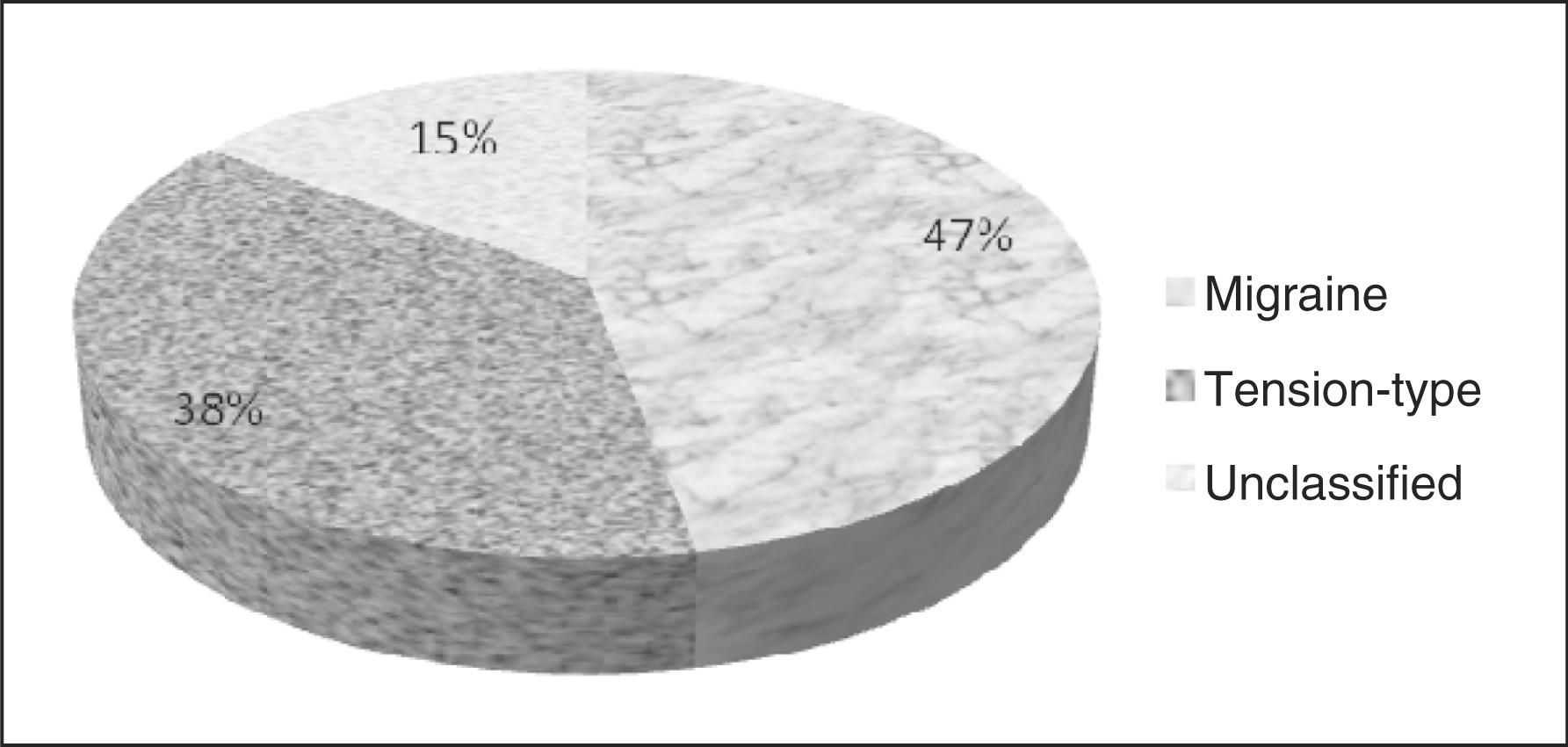
Breakdown of postictal headache type according to gender

PIH = postictal headache.
There were 84 (81%) patients with PIH who acknowledged that they self-medicated their headaches, mostly with paracetamol and non-steroidal anti-inflammatory drugs (NSAIDS). In contrast, only 20 (19%) patients had been given a prescription from a doctor to treat PIH, usually also paracetamol or NSAIDS, except for three subjects who had received amitriptylene. No patients had used specific migraine medication such as a triptan.
Comparison of study and control groups
Demographical data for study and control groups
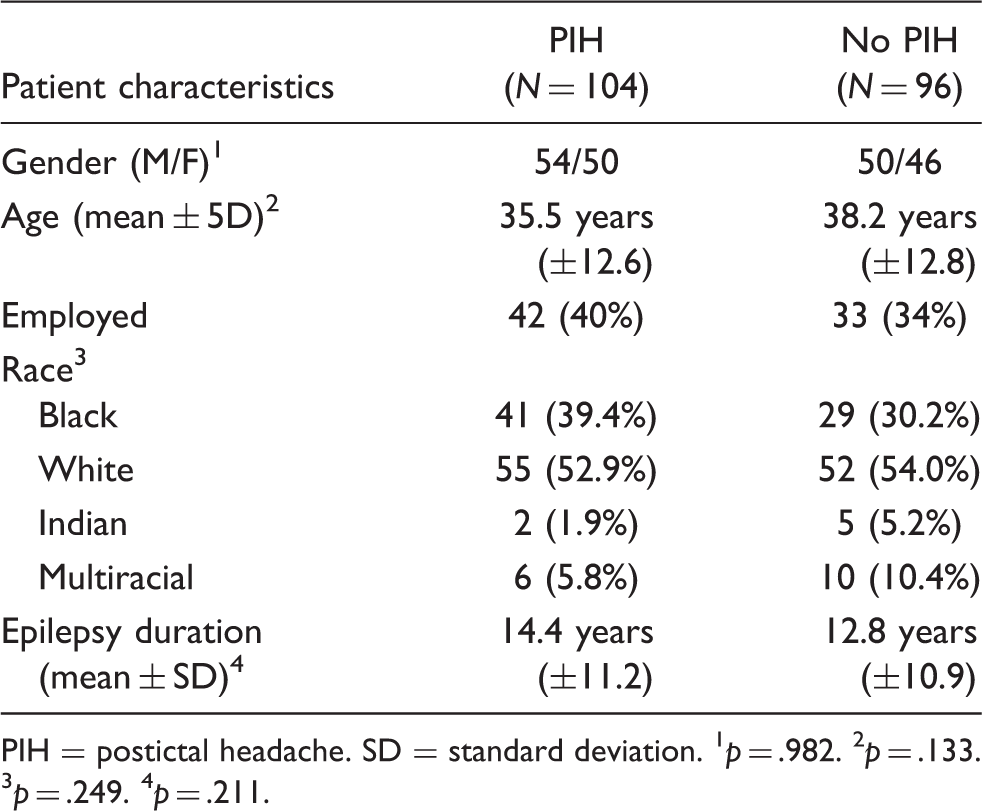
PIH = postictal headache. SD = standard deviation. 1 p = .982. 2 p = .133. 3 p = .249. 4 p = .211.
Comparison of seizure characteristics between study and control groups
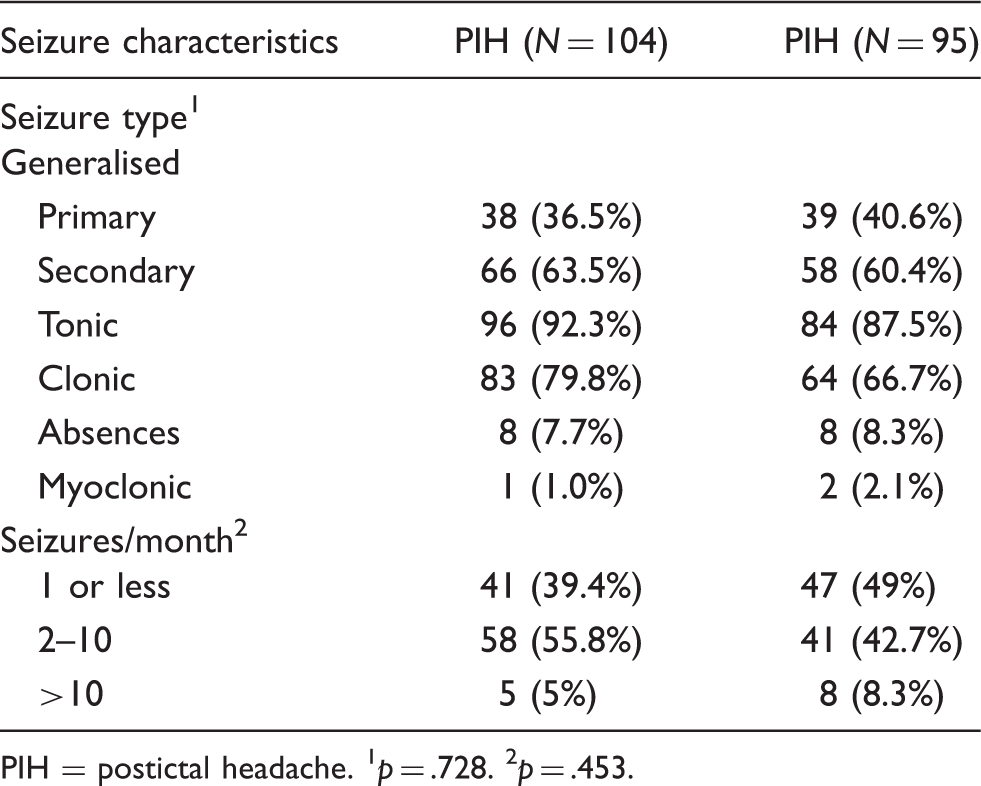
PIH = postictal headache. 1 p = .728. 2 p = .453.
A history of interictal headache was found to be significantly associated with PIH. A total of 67 of 104 subjects (64.4%) in the study group indicated that they experienced headaches which were unrelated to seizures, versus only 5 out 96 subjects (5.2%) in the control group (p = .9991). Further subgroup analysis was conducted for the 67 patients who had both postictal and interictal headache (Figure 6), showing that 40 (59.7%) had migraine-like, 14 (20.9%) tension-type and 13 (19.4%) an unclassified type of PIH. A clear relationship between interictal and migraine-like postictal headache thus emerged (p = .0001).
Type of postictal headache experienced by patients with a history of interictal headache.
A family history of first-degree relatives with either headache or epilepsy did not have a noteworthy association with the PIH group when compared to the controls.
The mean number of AEDs prescribed for subjects with PIH (2.10 ± 0.75) was remarkably similar to the number being used by subjects without PIH (2.11 ± 0.86). The most commonly used AEDs in both groups were valproate, clonazepam and carbamazepine (Figure 7).
Use of anti-epileptic drugs (AEDs) among patients with (N = 104) and without (N = 96) PIH. No significant differences are present.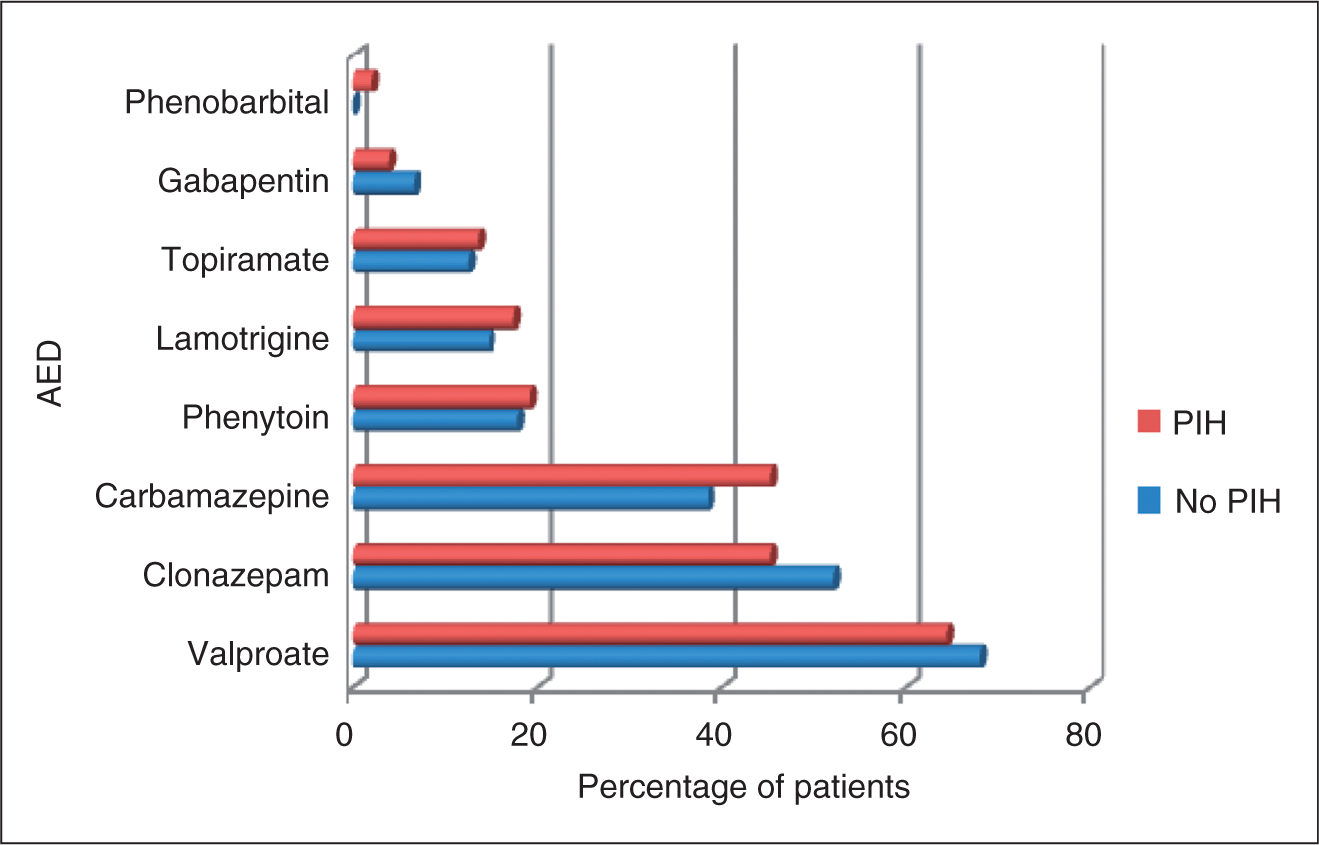
Among patients with migraine-like PIH (N = 49), 31 (63.4%) were using valproate, which did not differ appreciably from the 67 (70%) patients without PIH (N = 96) who were using the same drug. Similarly, no notable disparity was found in the usage of topiramate among the aforementioned two subgroups (migraine-like PIH: 16.3%; no PIH: 12.5%).
Discussion
Comparison with other studies
The main strength of our study lies in the fact that we evaluated PIH in 200 patients with exclusively generalised epilepsy. Previous studies on PIH have included patients with both partial and generalised seizures, and as a result these sub-groups of patients with generalised epilepsy were quite small. To our knowledge this study is the largest of its kind to evaluate PIH specifically in patients with generalised epilepsy.
Not many studies on aspects of PIH are available in the literature; however, PIH does seem to occur more commonly after generalised seizures than after partial ones (11,12). While Schachter et al. (9) reported that 96% of patients with generalised epilepsy experienced PIH, they did not make use of a standardised epilepsy classification system. The lowest reported prevalence of peri-ictal headache, including PIH, was 4.8% in a study by Kwan et al. In contrast to other studies, which mostly had a cross-sectional design, this study was performed prospectively, therefore raising concern that recall bias may be an important confounder in other studies. However, this study only collected data over three months, during which half of the patients did not experience a seizure and this may thus account at least in part for the low prevalence observed. The 52% prevalence of PIH in our study in which patients with primary and secondary generalised seizures were assessed is still lower than that found by others, such as Karaali-Savrum (10) (67%) and Syversten (6) (68%), where sub-groups of patients with primary generalised seizures were assessed.
One has to consider the possibility that our study population may have contained patients with partial epilepsy, which would also have influenced the prevalence.
Studies of PIH in patients with partial epilepsy reported a slightly lower prevalence in this sub-population, ranging from 16% to 44% (2,4,5). A significant association between PIH and occipital lobe epilepsy in particular has been demonstrated (2,11,14). It is postulated that the occipital area may play a key role in the pathophysiology of PIH, at least in patients with partial epilepsy.
In our study, 63% of subjects had PIH after every seizure, which compares well with the results of Leniger (1) (60%) and Förderreuther (4) (66%). As these studies included patients with all types of epilepsy, one may tentatively deduce that in so far as the frequency of PIH is concerned there are no differences in patients with generalised or partial seizures.
The mean duration of PIH in our study was 17.9 hours; variations from 5.9 to 12.8 and 20 hours, with large standard deviations (1,6,10), are seen in other studies. Thus, if the results are categorised, the majority of patients in various studies have postictal headaches which last from 4 to 24 hours (4,5,8).
In patients with partial seizures, up to 90% experience PIH ipsilateral to the epileptic focus (5). In our study, about half of the patients had PIH even though generalised seizures had occurred. The possibility that patients with secondary generalised epilepsy had PIH lateralising to the original insult has to be considered but was not further investigated.
In this study we calculated a mean value of 7 cm for the pain intensity of PIH on the VAS, with the majority of patients falling in the severe (≥7 cm) category. Other studies, performed in populations of patients with mixed types of seizures, generally reported lower values: Kwan (7) found a mean of 5.4 and Leniger (1) found a mean 6.4 on the VAS. The majority of patients in Förderreuther’s study (4) experienced PIH of moderate (3–7 cm) severity. The PIH in patients with generalised epilepsy, therefore, seems to be more severe.
A recent trend in PIH research has been to attempt classification of the PIH according to the ICHD-II criteria. Applying this the present study demonstrated that 47% of subjects with PIH had a migraine type of headache. This matches up to others, which have found postictal migraine rates of 34–55% (1,4,6). If the 14 patients from the unclassified group in our study (who had probable migraine) are also included with the main migraine group, the figure for patients with a migraine PIH would actually be 60%.
Two studies in cohorts of patients with exclusively partial epilepsy reported figures of 26% (12) and 16% (15) for migraine-like PIH, respectively. Considering that the aforementioned rates of 34–55% were from studies involving all types of epilepsy, it seems as if migraine PIH potentially has a stronger association with generalised seizures. This observation requires further verification.
Accounts of usage of over-the-counter analgesics by patients with PIH vary from 30–80% (4,5,7). Our finding of 81% lies towards the top of the range, which may be explained by the higher pain intensity among patients in our study, which would prompt them to self-medicate more readily.
The significant association between postictal and interictal headache in our study has also been noted by other researchers in groups of patients with mixed or partial epilepsy (4,5,9). Similar to our finding, Leniger et al. (1) have also reported that this relationship is strongest for patients with a migraine-like PIH.
Other associations with PIH reported by previous authors include a younger age of onset of epilepsy, as pointed out by Ito and colleagues (11). Schachter et al. (9) found that patients with four or fewer seizures per year were more than twice as likely to have PIH. These relationships with PIH were not duplicated in our study nor in others.
Treatment of postictal headache
No studies have been found which have evaluated any treatments for PIH. Two case reports, however, indicated that sumatriptan was able to terminate acute migraine PIHs (14,16). The triptans are well known for their efficacy in treating acute migraine attacks, and the AEDs valproate and topiramate are used for migraine prophylaxis (17,18). These agents are therefore attractive candidates for future research, specifically in patients who experience migraine-like PIH. In this study, no difference was found in the use of valproate or topiramate among the migraine-like PIH group and the control group. However, it is possible that patients in the latter group might already have had a prophylactic effect from the AED. The efficacy of these drugs needs to be tested in prospective studies, while controlling for the fact that some AEDs may actually cause headache as a side effect.
Study limitations
This study had several limitations. First, it was performed at a tertiary referral centre and may of the subjects may have had more refractory epilepsy compared to epilepsy patients in general. This was also reflected in the mean number of AEDs being used by study patients (2.1) and the fact that 78.5% of subjects were using polytherapy. As such one should be careful to extrapolate the results to general populations of patients with epilepsy who are well controlled.
Moreover, as a cross-sectional study, recall bias was a factor. We attempted to limit this by only including patients who had at least one postictal headache in the past year in the study group. However, 85.6% of patients with PIH were experiencing one or more seizures per month and the majority of patients had headache after every seizure. While the frequency of PIH therefore is unlikely to affect recall, postictal confusion may very well be a factor influencing a patient’s ability to remember headache characteristics. Unfortunately, by the very nature of the study, this problem is difficult to work around.
During the semi-structured interview patients were asked only whether they had interictal headaches. In retrospect it would have been useful to have characterised these interictal headaches in more detail and to have classified them according to ICHD-II criteria as well. In this way the relationship between postictal migraine and interictal migraine could have been investigated more thoroughly.
Conclusion
The study confirms that PIH in patients with generalised epilepsy is a common occurrence. The results add to the present literature by indicating in particular an association between generalised seizures and migraine postictal headache, as the majority of patients’ headaches (60%) could be classified as either migraine or probable migraine.
The gravity of the condition is reflected by the fact that the majority of patients experience PIH after every seizure, with severe headache lasting up to 24 hours and for which self-medication is mostly used; doctors do not seem to prescribe specific headache drugs to treat PIH. A history of interictal headache has emerged as a risk factor for PIH. Future research should focus on clarifying the pathophysiology of the condition and on evaluating the efficacy of medications for both acute and prophylactic treatment.