
Abstract
Background
Headaches associated with pituitary adenoma have been reported to be related to the structural characteristics and endocrine factors of the tumour itself.
Objectives
The objective of this study was to investigate the prevalence and clinical characteristics of, and the risk factors for, non-functioning pituitary adenoma (NFPA)-associated headaches in Chinese patients with normal endocrine activity.
Methods
Ninety-seven patients with a NFPA with normal endocrine laboratory results were prospectively enrolled in this study. The relevant clinical demographic data were collected and examined with the appropriate statistical methods.
Results
The pre-operative prevalence of tumour-associated headaches was 48.5%; 87.2% of these patients had migraine-like headaches. A family history of primary headache (odds ratio (OR) 3.67; p = 0.032) and a higher tumour Knosp grade (OR 1.83; p = 0.001) were identified as risk factors for the occurrence of NFPA-associated headaches. The patient’s age, sex, visual disturbances, optic chiasm compression, tumour size and tumour volume were not significantly associated with NFPA-associated headaches (p > 0.05). In addition, headache severity was significantly correlated with the Knosp grade (r = 0.339; p = 0.001). The sides of the headaches and of cavernous sinus invasion were significantly concordant (48.9% agreement; κ = 0.257; p = 0.007).
Conclusions
Migraine-like headaches are a common clinical manifestation in patients with NFPAs. A family history of primary headaches and cavernous sinus invasion are risk factors for NFPA-associated headaches.
Introduction
Pituitary adenomas are benign neoplasms located in the midline of the intrasellar base. The main clinical symptoms include headache, a loss of vision and neuroendocrine abnormalities. The reported prevalence of headaches associated with pituitary adenomas varies from 33 to 72% (1–6) and the pathogenesis of this disorder remains unclear.
Pituitary adenoma-associated headache has been reported to result from multiple effects of the tumour and endocrine changes (1). Abe et al. (3) and Almalki et al. (7) have proposed that functional pituitary adenomas which secrete excessive prolactin and growth hormone result in headaches that are not related to the size or invasiveness of the tumour. With respect to non-functional pituitary adenomas (NFPAs), which account for 25–30% of all pituitary adenomas (8), Ferrante et al. (9) found that the prevalence of NFPA-associated headache was high as 41.4%, although the associated causes require further clarification.
The studies that have investigated the relationships between structural risk factors and headaches associated with pituitary adenomas have not yet reached a consistent conclusion. Gondim et al. (10) have suggested that the causes of headaches in patients with pituitary adenomas are related to the tumour size, optic chiasm compression and cavernous sinus invasion, whereas Levy et al. (11) reported that differences in the headaches were not related to tumour size or cavernous sinus invasion. This study aimed to investigate the incidence of headaches in Chinese patients with NFPA and normal endocrine activity to observe the clinical characteristics of the headaches and to analyse the potential risk factors.
Methods
Patients
A total of 120 patients presented with an initial diagnosis of pituitary adenoma and normal pre-operative laboratory tests for endocrine activities. Those patients who opted for trans-sphenoidal surgery in the Department of Neurosurgery of Beijing Tiantan Hospital from January 2011 to September 2014 were selected for this study. This study was approved by the ethics committee of Beijing Tiantan Hospital and all patients gave informed written consent for inclusion.
The inclusion criteria were as follows: (a) patients aged between 18 and 70 years; (b) endocrine laboratory results within the normal range; (c) no pre-operative intracranial haemorrhage, infection, hypertension, epilepsy, brain trauma or other cause of headache; (d) no cervicogenic headache, temporal arteritis, neuralgia or headache caused by oral or maxillofacial lesions; (e) no psychogenic headaches; and (f) post-operative pathological reports indicating a diagnosis of NFPA. The exclusion criteria were: pregnant and breastfeeding women; patients with pituitary tumour and acute stroke; patients unable to clearly describe the symptoms of their headache as a result of aphasia or a decreased level of consciousness; a history of primary headache (e.g. migraine, tension-type headache, trigeminal autonomic cephalalgia or other primary headache disorders) prior to the diagnosis of the pituitary adenoma; and overuse of prescribed drugs.
The clinical characteristics of the patients (age, sex, family history of primary headache, clinical manifestations, medical history, visual disturbances and endocrine changes) were recorded pre-operatively.
Headache identification
A trained pain specialist conducted interviews using a questionnaire before and three months after the operation by telephone and subsequently screened the patients with headache according to the classification of pituitary adenoma-associated headache proposed by Schankin et al. (2). Each eligible patient with a pituitary adenoma-associated headache was experiencing the headache for the first time when the pituitary adenoma was detected by magnetic resonance imaging (MRI).
The patients with pituitary adenoma-associated headache fulfilled all three of the following criteria: (a) the patients reported headaches pre-operatively; (b) headaches resulting from the overuse of prescribed drugs were excluded based on the International Classification of Headache Disorders, 2nd edition (ICHD-II) (12); and (c) there was evidence of post-operative amelioration as defined according to both the Headache Index (13) and a reduction in the intake of drugs for pain relief of 50–100% compared with the pre-operative intake within three months of the operation.
The variables included: the side of the head on which the headache occurred; the quality, duration, frequency, triggers and pain-relieving features of the pain; and other associated symptoms. Headache severity was determined according to the following numerical rating scale: 1–3 (mild headache); 4–6 (moderate headache); and 7–10 (severe headache). The post-operative headaches were evaluated over three months according to the criteria for the treatment efficiency of migraine headaches (13). The Headache Index was defined as follows: headache severity (numerical rating scale) × headache duration (fraction of 24 hours) × headache frequency (days per month).
The following three categories were used to assess the post-operative resolution of the headache: complete resolution was defined as a 100% reduction in both the Headache Index and the intake of pre-operative drugs for pain relief; partial headache resolution was defined as a 50–99% reduction in the Headache Index and the intake of pre-operative drugs for pain relief; and no resolution was defined as a < 50% reduction in the Headache Index or the intake of pre-operative drugs for pain relief.
Tumour characteristics
The patient’s MRI results were interpreted by a neurosurgeon, who assessed the tumour size, optic chiasm compression, and the relationship between the tumour and the cavernous sinus (Knosp classification). Based on the maximum diameter of the tumour, each tumour was categorized as a micro-adenoma (≤1 cm), macro-adenoma (1–4 cm) or giant adenoma (≥4 cm). The shape of the pituitary adenoma was assumed to be an ellipsoid in the assessment of the tumour volume. After the measurement of the tumour diameter in three orthogonal planes, the tumour volume was calculated using Cavalieri’s principle using the formula: tumour volume = 4/3π (a/2 × b/2 × c/2), where a, b and c represent the diameter in the three dimensions. For multi-lobed tumours, the volume was assumed to be the sum of the volume of all the lobes.
Knosp classification
We used the Knosp classification, proposed in 1993, to assess the relationship between the tumour and the cavernous sinus as follows: the tumour did not cross the medial intercarotid line (grade 0); the tumour passed the medial intercarotid line, but did not cross the median intercarotid line (grade 1); the tumour extended beyond the intercarotid line, but did not extend beyond or tangential to the lateral aspects of the intra- and supracavernous internal carotid artery (grade 2); the tumour extended laterally to the lateral tangent of the intra- and supracavernous internal carotid arteries (grade 3); and the internal carotid artery was completely encased by the tumour (grade 4) (Figure 1) (14).
Anatomical diagram of the saddle area and the three-line schema for the Knosp classification. a: Internal carotid artery; b: cavernous sinus; c: hypophysiscerebri; d: lateral intercarotid line; e: median intercarotid line; and f: medial intercarotid line.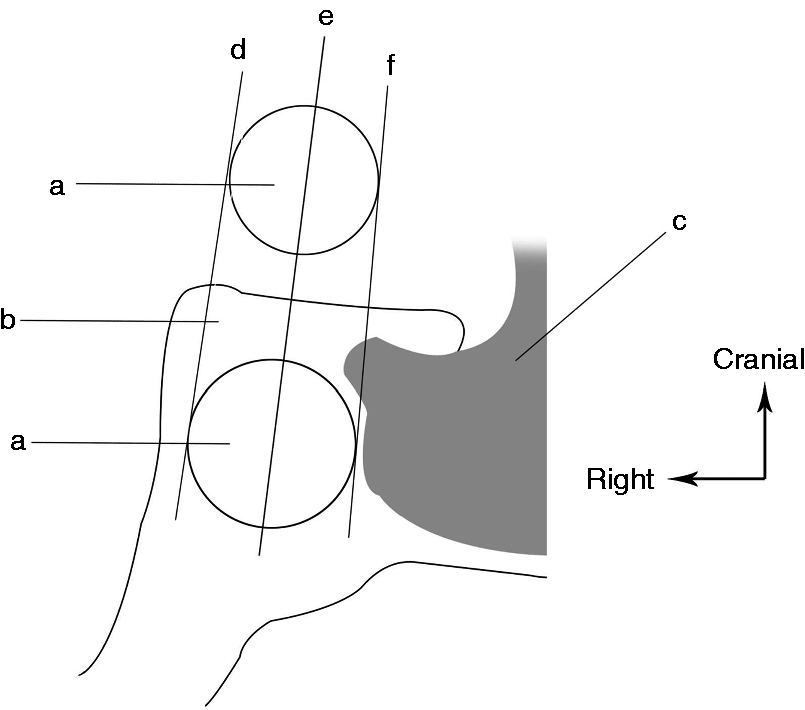
Statistical analysis
The statistical analyses were performed using IBM’s Statistical Package for the Social Sciences (SPSS) version 21.0 software. The t-test, χ2 test or Fisher’s exact test were used for univariate analyses to compare those patients with and without NFPA-associated headache. Continuous variables, including age and tumour volume, were analysed using t-tests. Categorical variables, including sex, family history of primary headaches, visual disturbances, optic chiasm compression, tumour size and Knosp grade, were analysed using the χ2 test or Fisher's exact test (when the expected values were < 5). The baseline variables with p < 0.2 were included as potential risk factors in the preliminary screening. Univariate and multivariate logistic regression analyses were then conducted to examine the potential risk factors for NFPA-associated headache. We identified the final multivariate model for NFPA-associated headache using a backwards stepwise approach with p < 0.05 of the likelihood ratio test for the exclusion of excess factors. Unadjusted and adjusted odds ratios (ORs) and their confidence intervals (CI) were calculated separately. Spearman statistics were calculated to examine the correlation between headache severity and Knosp grade. To assess concordance, the agreement (%) and κ statistic were calculated to compare the side of the headache and the side of cavernous sinus invasion; p < 0.05 was considered statistically significant.
Results
Among the 120 patients who were initially diagnosed with a pituitary tumour with normal endocrine activity, 97 were later verified to have NFPAs based on the post-operative pathological diagnoses. Twenty-three patients were excluded because they did not meet the inclusion criteria, including two patients with Rathke’s cleft cysts, seven patients with prolactin-secreting pituitary adenomas, four patients with follicle-stimulating hormone-secreting pituitary adenomas, three patients with luteinizing hormone-secreting pituitary adenomas, one patient with an adrenocorticotropic hormone-secreting pituitary adenoma, and six patients with pituitary adenomas with mixed secretions.
Characteristics of NFPA-associated headaches
Among the 97 NFPA patients, 53 patients reported headache for the first time simultaneously with the initial diagnosis of pituitary adenoma by MRI. Six of the 53 patients with pre-operative headache did not show post-operative remission and thus 47 patients were defined as having NFPA-associated headache. The calculated prevalence of NFPA-associated headache was therefore 48.5% in this study.
Among the 47 patients with NFPA-associated headaches, there were 41 patients with migraine-like headaches (87.2%), three patients with stabbing headaches (6.4%), two patients with cluster-like headaches (4.3%) and one patient with symptoms similar to those of short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (2.1%). With respect to the severity of the NFPA-associated headaches, 14 patients had mild headaches (29.8%), 25 patients had moderate headaches (53.2%) and eight patients had severe headaches (17.0%).
The overall duration of the occurrence of headaches in the 47 patients was between two weeks and 60 months, with a median duration of 10 months. Specifically, one patient had a headache for less than two weeks (2.1%), six patients had had headaches for between two weeks and one month (12.8%), eight patients had had headaches for between one and three months (17.0%) and 32 patients had had headaches for three months or longer (68.1%).
Headache conditions three months post-surgery
Among the 53 patients with pre-operative headaches, 19 showed complete headache remission three months after surgery, 28 showed partial remission and six showed no remission.
Risk factors for NFPA-associated headaches
Univariate analysis of non-functioning pituitary adenoma (NFPA)-associated headache in demographic data, clinical manifestation and imaging characteristics of the tumours.
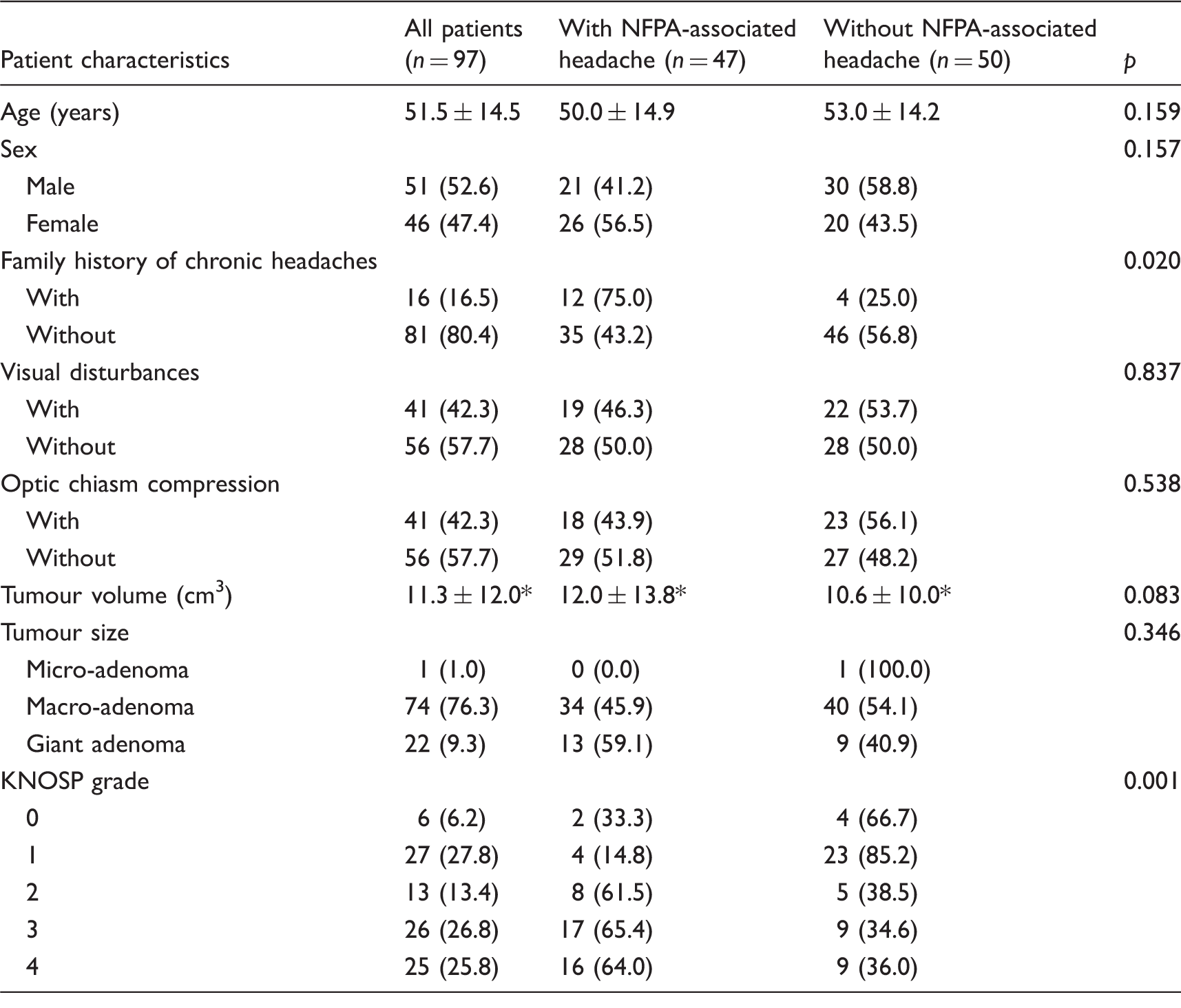
Data presented as mean ± standard deviation values of no. (%) of patients.
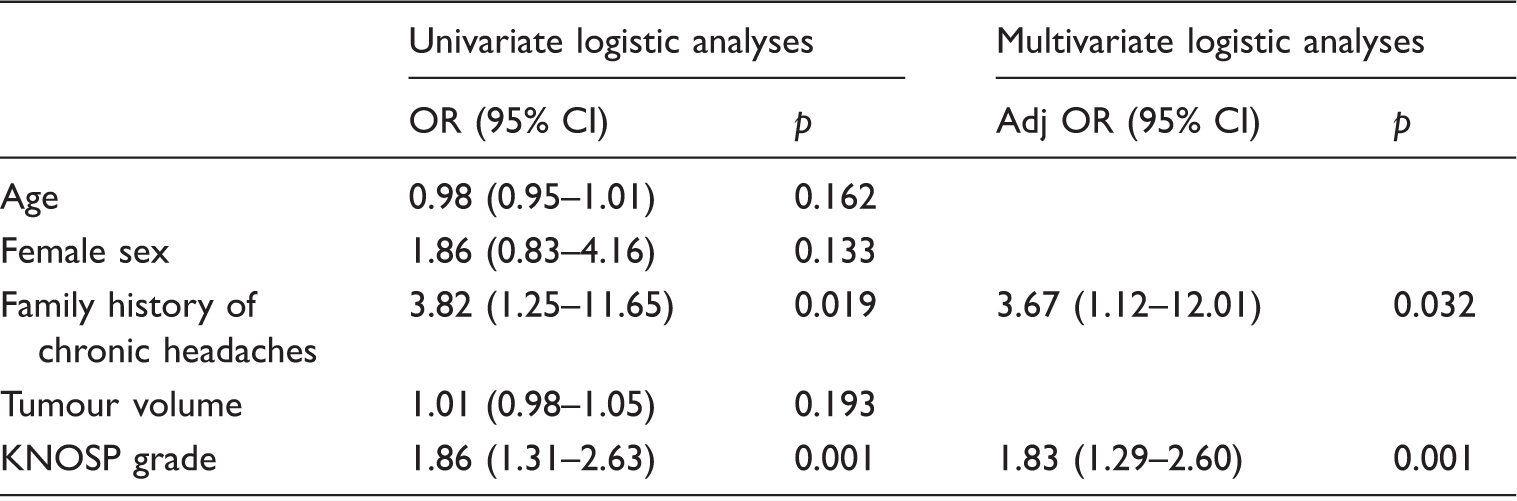
The patients with a family history of primary headache (χ2 test; p = 0.020) and higher Knosp grades (χ2 test; p = 0.001) were more likely to have NFPA-associated headaches (Table 1). The baseline variables shown in Table 1 with p < 0.2, including age, female sex, family history of chronic headaches, tumour size and Knosp grades, were entered into univariate and multivariate logistic regression analyses. The univariate logistic regression analyses showed that NFPA-associated headaches were significantly related to a family history of primary headache (OR 3.82; 95% CI 1.25–11.65; p = 0.019) and a higher Knosp grade (OR 1.86; 95% CI 1.31–2.63; p = 0.001) (Table 2). The multivariate logistic analysis also indicated that both a family history of primary headache (OR 3.67; 95% CI 1.12–12.01; p = 0.032) and a higher Knosp grade (OR 1.83; 95% CI 1.29–2.60; p = 0.001) were risk factors for NFPA-associated headache (Table 2). Further analysis showed a significant correlation between headache severity (four levels: no pain, mild headache, moderate headache and severe headache) and Knosp grade (Spearman rank correlation, r = 0.339; p = 0.001; Figure 2).
Incidence of severity of headache with different Knosp grades. Univariate and multivariate logistic analyses of potential risk factors for non-functioning pituitary adenoma-associated headache. Adj OR: adjusted odds ratio; CI: confidence interval; OR: odds ratio.
Relationships between the headache and side of cavernous sinus invasion
Concordance of the side of headache and cavernous sinus invasion sides.

Discussion
We observed 97 patients with NFPAs and normal endocrine activities who underwent trans-sphenoidal surgery. Among these patients, 47 (48.5%) patients had headaches that developed at the same time as the identification of the pituitary adenomas by head MRI. Nineteen (40.4%) patients with NFPA-associated headache had complete relief three months after surgery. However, the post-operative analyses revealed that 28 (59.6%) of the 47 patients with NFPA-associated headache had only a partial remission of headache and required further treatment. Thus it is important to clarify the clinical characteristics of, and risk factors for, pituitary adenoma-associated headache to improve the diagnosis and treatment of this disease.
Among the affected patients, up to 70.2% had moderate or severe headaches. The placebo effect has been reported to be particularly strong in all headache and pain disorders after invasive treatment. According to Schankin et al. (2), patients prefer surgery for the treatment of pituitary adenomas. Therefore it is likely that the patients had high expectations for the resection of their tumours rather than the treatment of their headaches and therefore, as in the study by Schankin et al. (2), the placebo effect can be neglected. The improvements in headache in this study were significantly temporally related to the successful treatment of the neoplasms. According to the ICHD-3 beta version (15), the headaches in this study met the diagnostic criteria for ‘headache attributed to intracranial neoplasm’, which is a type of secondary headache called ‘pituitary adenoma-associated headache’ (2). However, because the exact time course of the process of recovery from pituitary adenoma-associated headache after surgery is not known, the achievement of long-term (more than three months) post-operative headache amelioration requires further investigation with continuous follow-up.
Abe et al. (3) reported that pituitary adenoma-associated headaches primarily manifest as a feeling of a heavy head and that pulsating headaches are rare and only occur in female patients. Bussone et al. (16) indicated that pituitary adenoma-associated headaches are often similar to chronic tension-type headaches interspersed with occasional episodes of migraine-like headaches. Levy et al. (17) speculated that pituitary adenoma-associated headaches are primarily migraine-like headaches and have the major characteristics of vascular pulsating headaches. We found that 87.2% of the NFPA-associated headaches were primarily characterized as migraine-like headaches and that the majority were vascular pulsating headaches, which is consistent with the findings of Levy et al. (17). We hypothesized that migraine and pituitary adenoma-associated headaches may share a similar pathophysiological mechanism. Therefore, in addition to surgical treatment for tumour resection, the principles of migraine treatment should also be applied to the treatment of NFPA-associated headaches before and after surgery.
A series of studies by Levy et al. (11) and Schankin et al. (2) have shown that a family history of primary headache is a risk factor for headache associated with pituitary adenoma. Genetic factors are important risks for primary headache such as migraine or cluster headache (18,19). Our results are consistent with these earlier observations. One possible mechanism for headaches in patients with a family history of headaches is that the tumour alters the adjacent structures during its gradual growth. The genetic backgrounds of some patients may reduce the headache threshold and thus make these patients more likely to have headaches.
The Knosp classification is an important indicator for determining pre-operatively whether pituitary adenomas have invaded the cavernous sinus (14,20). Many pain-related receptors are distributed throughout the internal carotid artery, trigeminal nerve and ganglions in the cavernous sinus and therefore compression by the tumour may cause pain. Our clinical data on NFPA-associated headache identified the Knosp grade as an independent risk factor, whereas other factors, such as the patient's age, sex, visual disturbances, optic chiasm compression, tumour size and tumour volume, were not independent risk factors. In addition, the Knosp grade was significantly correlated with headache severity. Together, these findings support the hypothesis that pituitary adenomas with cavernous sinus invasion appear to stimulate afferent pain nerve endings in the cavernous sinus to cause headache (10). Consistent with the findings of Wang (21), the headache and cavernous sinus tumour invasion sides were concordant in our patients with pituitary adenomas. These findings further indicated that structural factors potentially account for the pathogenesis of NFPA-associated headache. However, further study is needed to verify the causality. It can be speculated that sufficient decompression of the cavernous sinus using reliable assistive technologies, such as intra-operative ultrasonic imaging or MRI, may be an effective method for relieving NFPA-associated headache. Because patients with early-stage NFPA do not have endocrine symptoms, they are not diagnosed until there has been severe compression by the tumour. Consequently, nearly all of the patients recruited for this study had large or giant adenomas, with the exception of a single patient with a micro-adenoma. The characteristics of, and risk factors for, headaches in patients with non-functional pituitary micro-adenomas need to be further investigated.
To eliminate the interference of endocrine factors, patients with NFPA with normal endocrine laboratory tests were selected for this study. However, although NFPAs are non-secretory, it is difficult to exclude the influence of endocrine changes on headaches because it is possible that some NFPAs exert paracrine effects via unmeasured peptides (22,23) which may affect the occurrence of NFPA-associated headaches. The influence of such peptides on NFPA-associated headaches requires further research. In addition, the growth of tumours in some patients with NFPA can continuously affect the gland tissue and alter the levels of secretion of different pituitary hormones. Notably, some of the patients with NFPA who were not enrolled in this study showed mildly increased serum prolactin levels. It remains to be evaluated whether the occurrence of headache is associated with endocrine dysfunction or structural factors in patients with NFPA with abnormal endocrine laboratory test results.
Although we used strict diagnostic criteria for pituitary adenoma-associated headache in this study, there are still some limitations. The major limitation is that primary headaches, especially those prevalent in the general population, may occur by chance. The prevalence of migraine in China has been reported to be 9.3% and that of other primary headaches, such as tension-type headaches, to be 10.8% (24). Although we tried to exclude patients with a history of primary headache prior to the diagnosis of pituitary adenoma-associated headache, primary headaches may still have occurred during this study and such coincidences are difficult to avoid. Even if surgery resulted in an improvement in the headaches in our study, it is not uncommon for headaches to respond to a surgical procedure for reasons that are not yet clear (e.g. the effects of anaesthesia). In addition, the mechanisms of headache are very complex. Pituitary adenoma-associated headache may result from multiple factors, including the tumour itself, infection, inflammatory cytokines and vascular changes (25). Among these factors, the levels of expression of inflammatory cytokines, such as neuropeptide Y, calcitonin gene-related peptide, vasoactive intestinal peptide and substance P, are thought to be additional important pathophysiological factors in pituitary adenoma-associated headaches (26–28). The therapeutic effects of other treatments in addition to surgery for patients with NFPA who showed partial remission after surgery were not investigated in this study and merit further research.
Conclusion
The prevalence of headaches associated with NFPA is relatively high. When diagnosed with NFPA-associated headache, the clinical manifestations in most of these patients were similar to those who had migraine headaches. Our results suggest that a family history of primary headaches and pituitary adenomas with cavernous sinus invasion are two significant risk factors for this type of disease. Clinicians should pay more attention to these two factors when taking medical histories and other examinations.
Clinical implications
In addition to surgical treatment for tumour resection, the principles of migraine treatment may also be applied to the treatment of NFPA-associated headache. A family history of chronic headaches and cavernous sinus invasion are risk factors of NFPA-associated headaches, which could lay the foundation for further clinical treatment. For patients with abnormal results on endocrine examination, further studies should be carried out to determine whether the occurrence of headache is associated with endocrine function or structural factors.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this study was supported by the High-level Technical Personnel Training Program of the Beijing Municipal Health System (grant numbers 2011-3-034 and 2014-3-035). These grants contributed equally to the clinical study, data analysis, and manuscript writing.