
Abstract
Background
Three successive editions of the International Classification of Headache Disorders and multiple guideline papers on headache care have described evidence based diagnosis and treatment of headache disorders. It remains unknown, however, to which extent this has improved the diagnosis and management of headache. That was the aim of our study in which we also analysed differences between three social groups in Russia.
Methods
We studied 1042 students (719 females, 323 males, mean age 20.6, age range 17–40), 1075 workers (146 females, 929 males, mean age 40.4, age range 21–67) and 1007 blood donors (484 females, 523 males, mean age 34.1, age range 18–64). We conducted a semi-structured, validated, face-to-face professional interview. Data on prevalence and associated factors have previously been published. A section of the interview focused on previous diagnosis and treatment, the topic of this paper.
Results
Only 496 of 2110 participants (23%) with headache in Russia had consulted because of headache. Students consulted more frequently (35%), workers and blood donors less often (13% and 14%). Only 12% of the patients with ICHD-3beta diagnosis of migraine and 11.7% with ICHD-3beta diagnosis of tension-type headache (TTH) had previously been correctly diagnosed. Triptans were used by only 6% of migraine patients. Only 0.4% of migraine patients and no TTH patients had received prophylactic treatment.
Conclusion
Despite existing guidelines about diagnosis and treatment, both remain poor in Russia. According to the literature this is only slightly better in Europe and America. Dissemination of existing knowledge should have higher priority in the future.
Introduction
In most countries, the great majority of headache patients are diagnosed, investigated and treated outside specialised centres. Unfortunately neither the precision of diagnosis, the use of investigations nor the treatment in general practice has been analysed sufficiently. Since the variability of such studies is likely to be high, large materials selected from the population are necessary. It is therefore important to study these factors in different social groups, something that to our knowledge has never been conducted before. We hypothesised that most headache patients are probably not diagnosed according to the International Classification of Headache Disorders, third edition beta (ICHD-3beta) (1). Further, that some probably undergo diagnostic tests that would not be needed if the ICHD-2 or now ICHD-3beta were correctly applied (2,3). Finally, we hypothesised that a wrong diagnosis leads to suboptimal treatment. Furthermore, different social groups may receive different medical service. We used the gold standard of headache diagnosis, which is a professionally conducted direct interview using a semi-structured, validated questionnaire. We applied this to blood donors, medical students and factory workers, more than 1000 in each group, and obtained ICHD-3beta diagnoses. A second semi-structured interview was focused on previous medical consultations, diagnoses, laboratory investigations and treatment. This information was then used to test the above hypotheses.
Materials and methods
Study design
This was a cross-sectional study that was conducted between September 2012 and August 2013. Details of materials and methods have been published before (4). An abbreviated version follows.
Study populations
We contacted 3361 and included 3124 people who agreed to be interviewed and were able to give characteristics of headaches unless the following reasons for exclusion were present: patient had a history of stroke or transient ischaemic attack (TIA), subarachnoid haemorrhage, intracranial aneurysm, intracranial haemorrhage, brain tumour, any operation on the brain, multiple sclerosis, epilepsy, encephalitis, meningitis, dementia, or other serious neurological or somatic disorder.
The sampling strategy was to prospectively and consecutively recruit participants from three different social groups. Selection of the group was based on a wish to cover the population as broadly as possible. Students represented the high intellectual and social group and workers performed manual work. Blood donors represented a middle group with much similarity to the general population (4). A feasibility aspect was part of the choice of social group. Thus we knew that students would have a high participation rate and we had previously studied blood donors and knew they would cooperate. Workers were recruited as part of a compulsory health examination.
Data collection
All participants were interviewed using a semi-structured interview conducted by a neurologist or by trained senior medical students supervised by a neurologist. The interview was an updated version of interviews used for multiple studies of the Olesen group and had thus proven its value in delivering reliable headache diagnoses according to the ICHD-1 and -2. A neurologist (N.R.K.) conducted direct face-to-face interviews with all workers and blood donors. Medical students also performed a direct interview. If details were missing from this interview or if the diagnosis was unclear, the neurologist made a telephone interview. In a previous study (Russell et al. 1996) we studied 371 individuals with suspected migraine by face-to-face interview and 219 people by telephone interview (5). In both cases the interview used the semi-structured format that, slightly modified, was used in the present study. There were no statistically significant differences between the face-to-face interview and the telephone interview for migraine or its subforms overall or analysing females and males separately. Fifteen senior (last year of medical school) medical students were recruited as interviewers but only 11 completed the training and conducted the actual interviews. The examiner students were first requested to read selected literature and were then examined for headache diagnosis. Thereafter they performed at least 10 supervised interviews that were not used in the actual study.
The student participants were interviewed in the classroom. Participation rate was 92%. Manual workers of an oil and gas factory were recruited as part of a compulsory annual medical examination of all employees. Participation rate was 97%. The interview was performed in the room where the neurologist examined the workers. If time did not allow for finishing the headache interview, the rest was completed in a subsequent telephone interview.
Blood donors were interviewed before or immediately after donation of blood. Participation rate was 98%. Because of the high participation rate in all three groups, it was judged unnecessary to perform a non-participant analysis.
The semi-structured interview was modified and expanded from a previously validated interview (6). It included four parts: 1) personal data (age, sex, profession, telephone number); 2) detailed characteristics of headache; 3) information about possible risk factors for headache and 4) previous consultations, diagnosis and treatment of headache. The first three data sets have already been published (4,7). The present paper addresses section 4, which consisted of the following questions:
Have you ever visited a doctor because of your headaches? What kind of doctors have you visited? Which diagnosis did you get because of your headache? Which examinations have been performed because of your headache (magnetic resonance imaging (MRI), computed tomography (CT) scanning, electroencephalography (EEG), X-ray of the cervical spine, ultrasound examination of cerebral vessels or vessels on neck, others)? Which therapy/drugs did you get or do you now use for acute headache attacks? Tell names of drugs (paracetamol, ibuprofen, combined analgesics, ergotamine drugs, sumatriptan and other triptans, other drugs). Number of days of regular painkiller use or triptan use per month. Have you ever used prophylactic therapy? Tell names of drugs (we asked also about all existing drugs). Which non-medical therapy did you get for treatment of headache and have you ever tried alternative methods of treatment?
The headaches of each participant were diagnosed according to ICHD-3 beta from the questionnaire forms by E.R.L., N.R.K. and J.O. We did not include questionnaires if important data were missing and it was impossible to contact the participant. We excluded on this basis 125 individuals and also excluded five individuals with previous severe neurological disease. The total number of participants included in the study was 3124.
Statistical analysis
We estimated that the average prevalence of migraine would be 12% and that it would be 16% in females and 8% in males. With a p value of 0.05 and a risk of type 2 error of 20%, we estimated that the sample size would need to be 258. In order to have power to detect sex-specific differences and to have enough power if differences were somewhat smaller, we chose a sample size of 1000. For each item we used only participants with data on that item. Therefore the number of participants in these tables was sometimes less than the total number in each group.
Statistical analyses were performed with SPSS 17.0 software. Continuous variables were summarised as means, and categorical variables as numbers and percentages. We used chi-squared to compare distributions of categorical variables between groups. We set statistical significance at p < 0.05. We first used binary logistic regression to estimate odds ratios (ORs) with 95% confidence intervals (CIs) for consulting and laboratory investigations. Prevalence estimates and 95% CI for the prevalence estimates of migraine and other headache were determined using previously described methods (4).
Ethical considerations
The Medical Ethics Committee of The Urals State Medical University approved this study. All respondents were informed of the purpose of the survey. Written informed consent was obtained from all participants.
Results
Overview of Russian study population, clinical characteristics of participants in three different social groups and their headache.

TTH: tension-type headache.
According to our previous study, students had the highest one-year prevalence of migraine (29%) and tension-type headache (TTH) (77%) (4). Workers had the lowest one-year prevalence of migraine (7%) and TTH (37%). Blood donors had intermediate prevalence: migraine 12%, TTH 62%.
Previous consultations and investigations of participants with ICHD-3beta interview diagnosis of migraine or TTH in three different social groups of Russia.

ICHD-3beta: International Classification of Headache Disorders, third edition beta; TTH: tension-type headache; EEG: electroencephalogram; CT: computed tomography; MRI: magnetic resonance imaging.
Laboratory investigations were conducted in half (52.6%) of patients with migraine or TTH by recommendations of physicians. These investigations included ultrasound examination of cerebral vessels (17%), MRI of the head (16%), X-ray of cervical spine (16%), EEG (14%) and CТ (4%).
We compared the ICHD-3beta diagnosis made at the interview to the diagnosis given by doctors previously (Table 3, Figure 1). Only 12% of the patients with an ICHD-3beta diagnosis of migraine and 11.7% with an ICHD-3beta diagnosis of TTH had been correctly diagnosed. Wrong diagnoses included: autonomic vascular dysfunctions (56%), cervical osteochondrosis (35%), and intracranial hypertension (10%). Patients with TTH had all these diagnoses more frequently than patients with migraine. Students had a diagnosis of autonomic vascular dysfunction and intracranial hypertension more often than blood donors and workers. Thus, participants from all three social groups had a wrong diagnosis in 75%–80% of the cases (Figure 1).
Percentage of previous correct diagnoses of migraine and tension-type headache (TTH) in three different social groups. Diagnosis at previous consultations in participants with ICHD-3beta diagnosis of migraine or tension-type headache (TTH) in three different social groups of Russia. ICHD-3beta: International Classification of Headache Disorders, third edition beta.

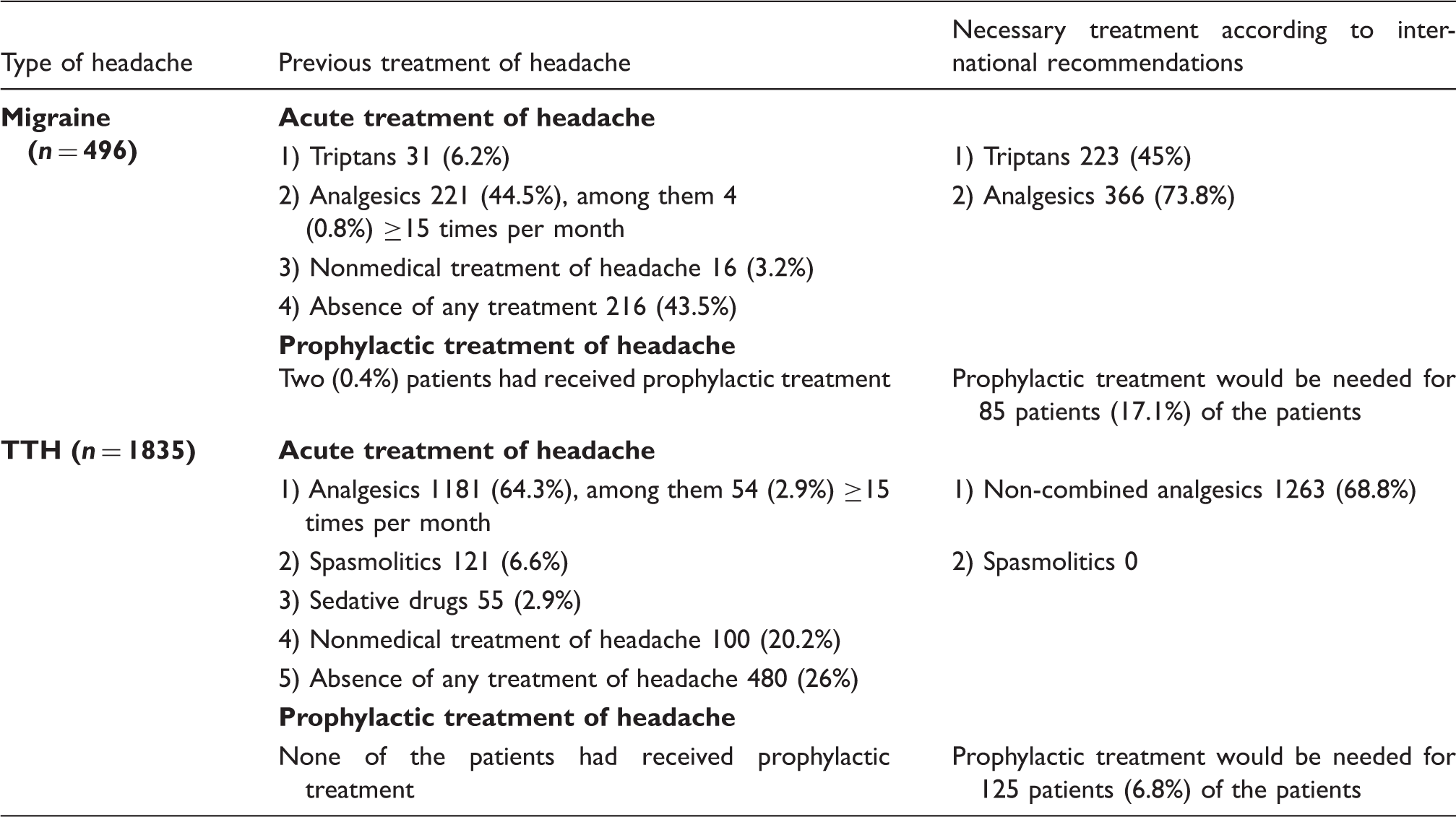
Previous treatments of headache in the three social groups according to ICHD-3beta diagnosis of migraine or TTH are presented in Table 4. We included all participants who had any past treatment of headache. Many drugs were not prescribed by physicians and participants used them by recommendations of pharmacists. The great majority of patients used only acute treatment. Only 0.4% of migraine patients and no TTH patients had received prophylactic treatment. Patients with migraine used analgesics or nonsteroidal anti-inflammatory drugs (NSAIDs) in 44% of cases and triptans in 6%. Patients with TTH used analgesics or NSAIDs in 64% of cases, other drugs (spasmolytics, anti-hypertensives or sedatives) in 11%. Analgesics ≥15 days per month were used by 0.8% of patients with migraine and 2.9% with TTH. Nobody used triptans ≥10 days per month. Many patients with TTH (20%) but few with migraine (3%) used non-medical treatments: cold to the head, drinking tea, sleep. A lot of patients with migraine (43%) did not use any treatment at all. One-fourth (26%) of patients with TTH did not use any treatment for pain relief. Treatment of migraine and TTH is summarised in Figure 2.
Previous treatment of migraine and tension-type headache (TTH). Previous treatment of participants with ICHD-3beta interview diagnosis of migraine or tension-type headache (TTH) in three different social groups of Russia. ICHD-3beta: International Classification of Headache Disorders, third edition beta; NSAID: nonsteroidal anti-inflammatory drug.
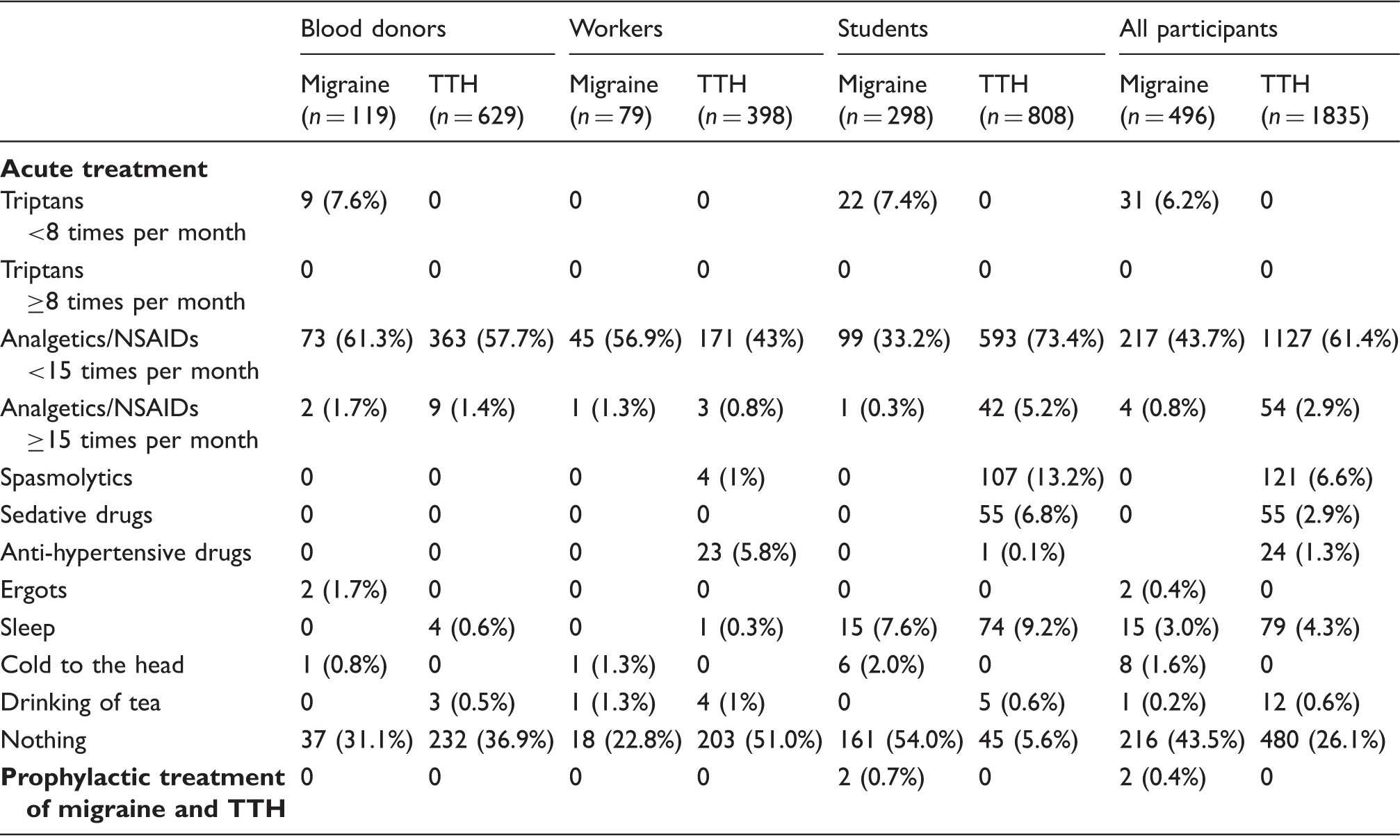
Only students used triptans (7.4%) or prophylactic drugs (0.7%) for treatment of migraine. Only students had medication-overuse headache (analgesics): in 5.2% of cases with TTH and in 0.3% of cases with migraine (Table 4). They frequently used sleep for pain relief. Only workers used anti-hypertensive drugs for pain relief (5.8%). We did not find any special features of treatment of headache in blood donors.
Discussion
By a validated, semi-structured, diagnostic interview in three social groups in Russia comprising more than 3000 individuals, we found that many patients with migraine and TTH had not consulted because of headache, and those who did often received the wrong diagnosis and treatment. Our study showed lower use of triptans and prophylactics and lower rates of correct headache diagnosis than in most other studies.
Do patients with headache consult?
Compared to previous Russian research (8,9), our patients with migraine had consulted two times more frequently (54% versus 25%) but patients with TTH had consulted almost with the same frequency (12.5% versus 9.5%). Our data are in accordance with most population-based European studies. In Denmark 56% of patients with migraine had consulted their GP. The corresponding percentage among people with TTH was 16% (10). One or more specialists had been consulted by 16% of migraine sufferers and by 4% of patients with TTH. The consultation rates of chiropractors and physiotherapists were 5%–8%, all similar to our results (10). In Germany only 42% of migraineurs had consulted a physician, and the majority relied exclusively on over-the-counter medication (11). In Italy 29.2% of respondents had received no type of professional health care, such as from their GP, a headache specialist, or a headache centre (12). Another study conducted in Italy found that 62.4% of patients with migraine visited their GP in the last year, 38.2% saw a specialist for headache, 23% attended an emergency department and 4.5% were admitted to hospital for migraine (13). In Croatia half of patients with headache and 36.3% of respondents with migraine had never visited a doctor. More than half of TTH patients had never visited a physician (14). The majority of patients were only partially satisfied with their current treatment, and almost one-third were not satisfied. Patients in Europe had mostly consulted GPs, while in Russia they had more often consulted neurologists. In China significantly higher proportions of respondents with migraine (52.9%) or headache on ≥15 days per month (47.9%) had consulted a physician for headache than of those with episodic TTH (41.1%; p < 0.05) (15). In Korea less than half (40.7%) of the individuals with chronic daily headache reported having consulted a doctor for their headaches (16). In the United States (US) 68% of female and 57% of male migraineurs reported having consulted a doctor for headache (17). In Japan as many as 59.4% had never consulted a physician about their headaches (18). The most common reason why sufferers had stopped visiting their physician was that they had been told their headaches were not fatal. In Norway the top three barriers to optimal care were misidentifying migraines as headaches (50%), satisfaction with current treatment (45%) and inconvenience of physician consultation (41%) (19). Women were more likely to consult than men (20).
Do patients get the right diagnosis?
In the United Kingdom (UK) 70% of headaches were not given a diagnostic label, 24% were diagnosed as primary, and 6% as secondary headaches (21). It was suggested that GPs’ difficulty in diagnosing headache contributes to the high level of morbidity and unmet need in this disease. In the US only 56.2% of those with migraine had ever received a medical diagnosis. In France 60% of all migraine patients were not aware that they had migraine (22). In Spain 55.9% had been previously diagnosed with migraine (23). In Turkey 42% of patients with migraine got the right diagnosis during the first visit to a doctor and 51% got the correct diagnosis at further visits (24). Less than half of patients (45%) had received a diagnosis of migraine from a physician in Sweden (25). In Italy only 26.8% of migraine patients had a previous diagnosis of migraine (13). Our study showed that only 12% of migraine patients and 11% of TTH patients got the correct diagnosis in Russia. This is even worse than the unsatisfactory situation described above for other countries. Probably the main reasons are very poor uptake in Russia of the international headache classification and of the international guidelines about treatment of headache. Russian doctors seem to still use old-fashioned, locally popular diagnoses such as autonomic vascular dysfunctions (56%) and cervical osteochondrosis (35%). These diagnoses still figure in the official Russian guidelines. Due to the efforts of a few enthusiastic Russian headache experts, efforts of the Global Campaign Against headache and a progressive minister of health, these guidelines are presently being modernised and will in future use the ICHD-3beta classification terminology and diagnostic criteria.
Do patients get the right investigations?
Few studies have analysed the use of laboratory investigations for patients with primary headache in the general population (10,26,27). This requires a large study like ours in which thousands of people are directly interviewed to obtain the correct diagnosis of migraine and TTH. One may then look back and consider if laboratory tests had really been necessary. Even then such evaluation is difficult. There may have been atypical features at the time of previous consultation, the headache may have been resistant to treatment, etc. In Denmark supplementary diagnostic investigations due to headache were rare (<3%) (10). In Brazil, on the other hand, doctors usually recommended one or two additional examinations for patients with primary headache, most frequently EEG (26). In Moldova doctors frequently used X-ray of the cervical spine for patients with headache (27). While the indication for CT and MR of the head are difficult to assess retrospectively, it is clear that EEG and Х-ray of the cervical spine are almost never indicated (28). In the present study we show that several laboratory tests were probably not necessary.
Do patients get the right treatment?
In the present study most participants used only acute treatment for their headache. In the US 49% usually used over-the-counter medications, 20% usually used prescription medications, and 29% used both (29). Only 12.4% of migraineurs in our study indicated that they had taken a migraine-preventive medication, but 17.2% had used medications such as beta blockers with potential anti-migraine effects for other medical reasons (29). In Korea 40.7% of patients with chronic daily headache had not received treatment for their headaches during the previous year (16). In Italy 82.8% of patients with migraine used non-specific drugs for migraine attacks, whereas 17.2% used triptans and only 4.8% used a preventive migraine medication (13). About 80% of migraine patients took over-the-counter medications (13).
In Norway complementary and alternative medicine (CAM) was used by 62%, most often physiotherapy, acupuncture and chiropractic treatment. Contact with a physician increased the probability of use of CAM. Acute headache medications were taken by 87%, while only 3% used prophylactic medication (30). In Croatia in a population-based study, specific anti-migraine therapy was taken by half of patients with migraine: 35.7% of patients used triptans and 21.7% ergotamines. Prophylactic treatment had been used by 13.9% with migraine, 1.2% with TTH, and 6.9% with probable migraine (31). Alternative methods of treatment had been tried by 27% of migraine and TTH patients. In a population-based study in Turkey, although more than half of the migraineurs reported four or more attacks per month and severe intensity, only 4.9% were on prophylactic medication mostly with selective serotonin reuptake inhibitors (SSRIs) although these are known to be ineffective in migraine and TTH (24). The current and past use of other prophylactic treatments such as beta blockers, flunarizine and anti-epileptic drugs were less than 1% each. As attack medication, 19.3% of migraineurs reported the use of simple analgesics, 15.8% combined analgesics, 41.4% NSAIDs, 14.5% ergots, and only 2.9% triptans (24). Our data are in accordance with a previous Russian study which found that 40% of patients used combined analgesics for acute treatment of headache, 22% used simple analgesics, 0.5% of patients used triptans and 0.7% used prophylactic treatment (9).
Previous treatment of migraine and tension-type headache (TTH) in a Russian population in comparison with international recommendations.
It is necessary to improve diagnostics and treatment of headache by continuous campaigns and teaching throughout the world. The Global Campaign Against Headache in collaboration with the World Health Organisation already runs such campaigns but even stronger efforts are needed. The size of the problem is clear; now is the time to effect change (34).
Strengths and weaknesses of our study
A strength of our study was that we used the ICHD-3beta for an epidemiological study for the first time. Furthermore, we used a direct, validated, semi-structured interview instead of a self-administered questionnaire. We studied different social groups and each group had a very large size for a direct interview study.
The three social groups are not representative of the general population, but this is still a bottom-up study of unselected people rather than patients. It is a weakness that participants from villages and low social strata who have a high prevalence of headache in previous studies were missing. Therefore our results cannot be generalised to the whole Russian population. We did not use headache diaries, but that was impossible to do without a high drop-out rate.
Conclusion
The inappropriate diagnosis, investigation and treatment of primary headache disorders in our material reflect insufficient use of the ICHD and international guidelines for investigation and treatment.
Clinical implications
It is extremely important to accurately diagnose patients with headache according to the International Classification of Headache Disorders (ICHD) but diagnosis is often wrong, leading to incorrect treatment. Old-fashioned diagnostic procedures such as electroencephalography (EEG) and X-ray of the skull/cervical spine are still used too much but this is also true for neuroimaging. Triptans are used too little for attack treatment. Prophylaxis is used far too little. Clinical and laboratory diagnosis as well as treatment of headache disorders need improvement in the general population.
Footnotes
Acknowledgements
We gratefully acknowledge the following doctors and students who participated in this study: T.S. Tsypushkina, P.A. Filimonova, K.I. Fljagina, N.I. Tsvetkova, E.A. Korzovatykh, A.N. Ruzaeva, V.V. Shirshova, A.D. Kozlova, T.A. Troshina, A.D. Malygina, A.M. Alent’ev, Ju.S. Drozd, Ju.V. Sarafanova, I.A. Dyachkov, P.A. Oshurkov and A.V. Dmitriev.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.