
Abstract
Background
Osmophobia (Os) has been reported to be much more prevalent in migraine (M) than in other primary headaches, and its high specificity in the differential diagnosis between M and tension-type headache (TTH) has been reported. Os was included in the ICHD II Appendix as a diagnostic criterion of M. It disappeared in ICHD-3 beta. To understand this choice, we reviewed the literature after 2004.
Methods
This was a systematic review. We searched in PubMed, MEDLINE and Cochrane library for “osmophobia”, “odour/odorphobia AND headache”, “odour/odor hypersensitivity AND headache” and “olfactory hypersensitivity AND headache”.
Results
112 papers cited Os as an accompanying symptom of headache; 16 focused on Os in M diagnosis. With the data from 40 articles, we calculated the pooled prevalence of Os in 14,360 patients (2281 pediatric) affected by M (n = 12,496) and TTH (n = 1864). In M, the prevalence was 48.5% (CI 95% 41.4 to 55.8%) in adults and 23.4% (CI 95% 15.7 to 33.4%) in pediatric patients; in TTH, the prevalence was 8.9% (CI 95% 4.6 to 13.5%) in adults and 7.9% (CI 95% 3.3 to 18.1%) in pediatric patients. Ten of these papers allowed us to calculate the sensibility and specificity of Os in differential diagnosis between M and TTH. In adults, the value of specificity was 94.1% (CI 95% 88.9 to 96.9%), and sensitivity was 51.4% (CI 95% 38.4 to 64.2%). In pediatric patients, specificity was 92.0% (CI 95% 81.9 to 96.7%), and sensitivity was 22.1% (CI 95% 10.1 to 41.8%).
Conclusion
The literature endorses the inclusion of Os among M diagnostic criteria. On this ground, the decision to remove Os from ICHD 3 beta appears unjustified and a revision of this choice is recommended.
Introduction
Pain features and associated symptoms are cornerstones of the classification and differential diagnosis of primary headaches (1,2,3). As far as migraine (M) is concerned, no symptom has been identified as pathognomonic. Besides nausea, vomiting, phonophobia and photophobia, there are other manifestations that are variably reported by patients during M attacks. Among these osmophobia (Os), defined as unbearable perception of odours that are non-aversive or even pleasant outside the attack, had been identified as an accompanying symptom of M since ancient times (4). As early as the second century AD, Aretaeus of Cappadocia asserted that the sense of olfaction was altered during an M attack (“scents and unpleasant odours are equally intolerable”) (5). In the 19th century, Gowers evidenced that odours can trigger an M attack (6) and Liveing stated that “… the most grateful odours are with difficulty endured by the [migraine] sufferer” (7). Despite these time-honoured observations, until recently the relationship between Os and headache had been under-investigated in contemporary medical literature. In 1954 Friedman et al. reported a high prevalence of hypersensitivity to odours in migrainous patients (8), and in 1982 Wolfberg and Ziegler described osmophobic olfactory hallucinations in M (9). In 1985, Blau and Solomon reported the presence of Os in 20 out of 50 migrainous patients, suggesting that the prevalence of Os was comparable with that of photophobia or phonophobia (10).
Published in 1988, the first International Classification and Diagnostic Criteria for Headache Disorders, Cranial Neuralgias and Facial Pain (ICHD I) standardized the diagnostic criteria, becoming a milestone both in clinical practice and research (1).
This document, of unquestionable importance as an operational guideline, was a crucial stimulus also to ameliorate the proposed criteria. In fact, examining the ICHD I criteria for M, it was evidenced that there was the possibility of a diagnostic overlap between migraine without aura (MO) and tension-type headache (TTH) (11,12,13,14) in adults and in pediatric patients, since both forms can be characterized by pain of moderate intensity, overlapping duration and similar accompanying symptoms, even if quantitatively different.
On this ground, clinical practice and increasing knowledge about the relationship between M and olfaction (15,16,17) brought some researchers to focus on Os as a possible adjunctive symptom useful in the differential diagnosis among primary headaches and particularly between M and TTH. Merikangas et al., investigating the validity of the ICHD I diagnostic criteria for M and the discriminating capacity of each accompanying symptom in relation to subjective distress, found that Os had good sensitivity (higher than 50%) and specificity (higher than 60%), the latter being higher than that of other recognized criteria such as pulsating quality, photophobia and phonophobia. She suggested that the inclusion of Os among the M criteria could permit a more accurate differential diagnosis against other primary headaches (18).
In 1999, a Scandinavian study compared TTH and M in terms of hypersensitivity to environmental stimuli, reporting a higher presence of Os in migrainous than TTH patients (46% vs 13%) (19). In 2001, Spierings et al. found that smell hypersensitivity differentiated M from TTH, intolerance to smell being significantly more prevalent in migrainous patient (68% versus 29%) (20).
In the Italian guidelines for M treatment (21), released in 1993 by the Italian Society for the Study of Headache and revised in 2001 (22), Os was quoted as a relevant accompanying symptom and as a valuable diagnostic aid for the differential diagnosis of M versus TTH. Also, the Canadian guidelines on M diagnosis, published in 1997, recommended that in the anamnesis “the presence of aversion to odors also [has to] be determined” and noted “…[osmophobia] is a highly sensitive and specific feature of migraine” (23).
In 2004, Kelman published two articles investigating the place of Os in M diagnosis on a large sample of patients. In the first article, he reported a 24.7% Os prevalence in migraineurs. In the second, he highlighted the role of Os in the diagnosis of M, calculating its sensitivity and specificity in the presence and absence of nausea and vomiting, alone or in association with other symptoms. Os was demonstrated to be specific, although scarcely sensitive, in the diagnosis of M. In the absence of nausea and vomiting, sensitivity and specificity of Os alone, or in association with phonophobia or associated to photophobia, were respectively 1.1% and 98.4%, 1.1% and 98.6%, and 1.1% and 99.0% (24,25).
In 2004, 16 years after the first release of ICHD I, a revised version (ICHD II) was published (2), where the potential usefulness of Os for M diagnosis was recognized. Indeed, a modified version of criterion D of ICHD I for MO diagnosis, which included Os, was proposed and was inserted in the ICHD II Appendix to stimulate further research on this topic (“A1.1 criterion D. During headache at least two of the following: 1) nausea; 2) vomiting; 3) photophobia; 4) phonophobia ; 5) osmophobia”).
Ten years later, in 2013, a provisional draft for a new edition of headache classification (ICHD 3 beta) was proposed to the scientific community. In this version, Os was deleted without explanation from the Appendix. Indeed, in ICHD 3 beta Os is just mentioned in the definition of “accompanying symptoms” on the footnotes of the classification (“Accompanying symptoms: Symptoms that typically accompany rather than precede or follow headache. In migraine, for example, the most frequent are nausea, vomiting, photophobia and phonophobia; osmophobia, diarrhoea and other symptoms occur more rarely”) (3).
To check for possible reasons leading to this exclusion, we reviewed the literature on this topic. To the best of our knowledge this is the first review of Os and its relevance in M diagnosis, even if a partial analysis of our data had been already presented in October 2015 (26).
Methods
A systematic review was carried out on Medline, PubMed and on Cochrane Library using as keywords the following terms: “osmophobia”, “odour/odor phobia AND headache”, “odour/odor hypersensitivity AND headache” and “olfactory hypersensitivity AND headache”. We limited our research to articles in English, French, Spanish and Italian. The electronic bibliographic search was conducted in February 2016. All articles citing Os (apart from case reports) published from May 2004 (after the release of ICHD II) up to February 2016 were considered potentially eligible. Full texts were checked, and their references controlled carefully to ensure that all significant papers were included in the review. Data on the prevalence of Os in M and TTH, and values of sensitivity, specificity, positive (PPV) and negative (NPV) predictive value of Os in M diagnosis were collected. Data about patients in which M or TTH diagnosis was only “probable” were not included in our study. Data about possible comorbidity between M and TTH in the same patient in each article were also collected. Using available data, a global analysis was performed by the random effect model, to determine the prevalence of Os in M and in TTH, in both adult and pediatric patients, and to evaluate the heterogeneity among articles.
The same statistical model was used to calculate cumulative values of sensitivity, specificity, PPV, NPV, odds ratio (OR) and risk ratio (RR) of Os in the differential diagnosis between the two principal forms of primary headache, in both pediatric patients and adults. Differences between adult and pediatric patients were calculated using ANOVA Q test.
Results
Summary of the articles that analyze osmophobia in the differential diagnosis between migraine and tension type headache.

Abbreviations: Os osmophobia; Sn sensitivity, Sp specificity, PPV positive predictive value, NPV negative predictive value; M migraine, MO migraine without aura, MA migraine with aura, CM chronic migraine, TTH tension-type headache, ETTH episodic tension-type headache, CH cluster headache, oPH primary headaches other than M and TTH, OPH other primary headaches.
This table sums up how the problem of migraine (M) and tension-type headache (TTH) co-diagnosis is approached in each of the 44 papers reporting prevalence of osmophobia in migraine and/or tension type headache.

Legends:
Italics: article reporting prevalence of osmophobia in migraine only.
In our analysis, we excluded four articles (41,71–73) because patients from these articles had been included by the same authors in larger studies taken into account in our statistical analysis.
As a whole, these 40 articles collected 14,360 subjects, 2281 of which were pediatric patients (<18 year old). In the total sample, 12,496 patients had an M diagnosis while 1864 were TTH patients. The prevalence of Os in M and TTH was highly variable in different studies.
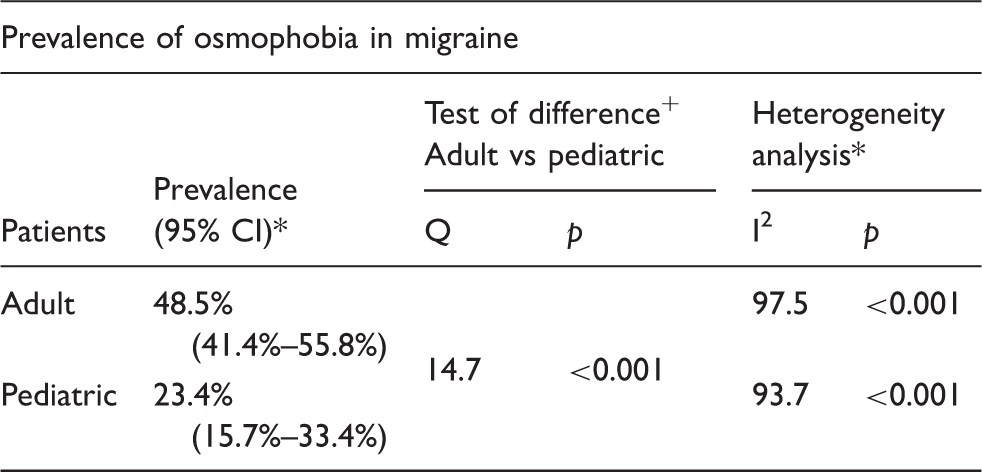
In M, values ranged from 8.3% to 86% in adults, and from 10.3% to 34.6% in pediatric patients. Therefore, a high degree of heterogeneity, in terms of prevalence of Os, was demonstrated among the articles, both in adults and pediatric patients (I2 adults 97.5, pediatric patients 93.7, p < 0.001). The calculated pooled prevalence of Os was 48.5% (CI 95% 41.4 to 55.8%) in adults and 23.4% (CI 95% 15.7 to 33.4%) in pediatric patients, and a significant difference was found when comparing calculated values in the two groups. Results regarding the calculated prevalence of Os in M from pooled data are summarized in Table 3.
Prevalence values of osmophobia in migraine and 95% confidence intervals (CI) are calculated in adults and pediatric patients from pooled data of 33 and six articles respectively; high and significant heterogeneity (I2) of data is observed among different articles (*random effects model). A significant difference is found between adult and pediatric patients (+Anova Q Test).
Prevalence values of osmophobia in tension-type headache and 95% confidence intervals (CI) are calculated in adult and pediatric patients from pooled data of eight and three articles respectively; high and significant heterogeneity (I2) of data is observed among different articles (*random effects model). No significant difference is found between adult and pediatric patients (+Anova Q Test).

Analyzing data from adult patients stratified by the country in which each study was conducted, we found a significantly higher prevalence of Os in Asian countries than in Western countries, both in M and TTH patients. The same can be said of Latin American countries, in which the prevalence of Os was significantly higher than in Western areas. When comparing Asian and Latin American patients alone, the values of prevalence of Os appeared to be significantly higher in Asian patients suffering TTH. As far as M is concerned, despite a tendency to a higher prevalence of Os in Asian migraineurs than in Latin American ones, the difference is not significant. The same analysis was not possible in pediatric patients, because the studies on children had been carried out in Western countries, and in Italy in particular.
Osmophobia in differential diagnosis between migraine and tension-type headache in adult and pediatric patients. Sensitivity, positive predictive value (PPV), odds ratio (OR) and risk ratio (RR) of osmophobia in migraine are significantly higher in adults than in pediatric patients, while specificity and negative predictive values (NPV) are not significantly different in the two groups (*random effect model, +Anova Q-test). 95% confidence intervals (CI) are reported.

The odds ratio (OR) and risk ratio (RR) for M in osmophobic patients was 27.5 (CI 95% 9.6–78.9) and 9.3 (CI 95% 4.7–18.4) in adults, 3.4 (CI 95% 2.5–4.7) and 2.7 (CI 95% 1.9–3.8) in pediatric patients (Figure 1). Analysis of OR and RR demonstrated a high heterogeneity between studies in adults (OR I2 83.8, p < 0.001; RR I2 71.1, p 0.002), while the studies in pediatric patients appeared homogeneous (OR I2 0.0, p 0.445; RR I2 15.6, p 0.308). When comparing the two groups, OR and RR appeared significantly higher in adults than in pediatric patients (Table 5).
Odds Ratio (OR) of osmophobia for migraine versus tension-type headache. Values in different articles and of our pooled analysis (calculated by random effects model) are reported with 95% confidence interval (CI) and graphically compared.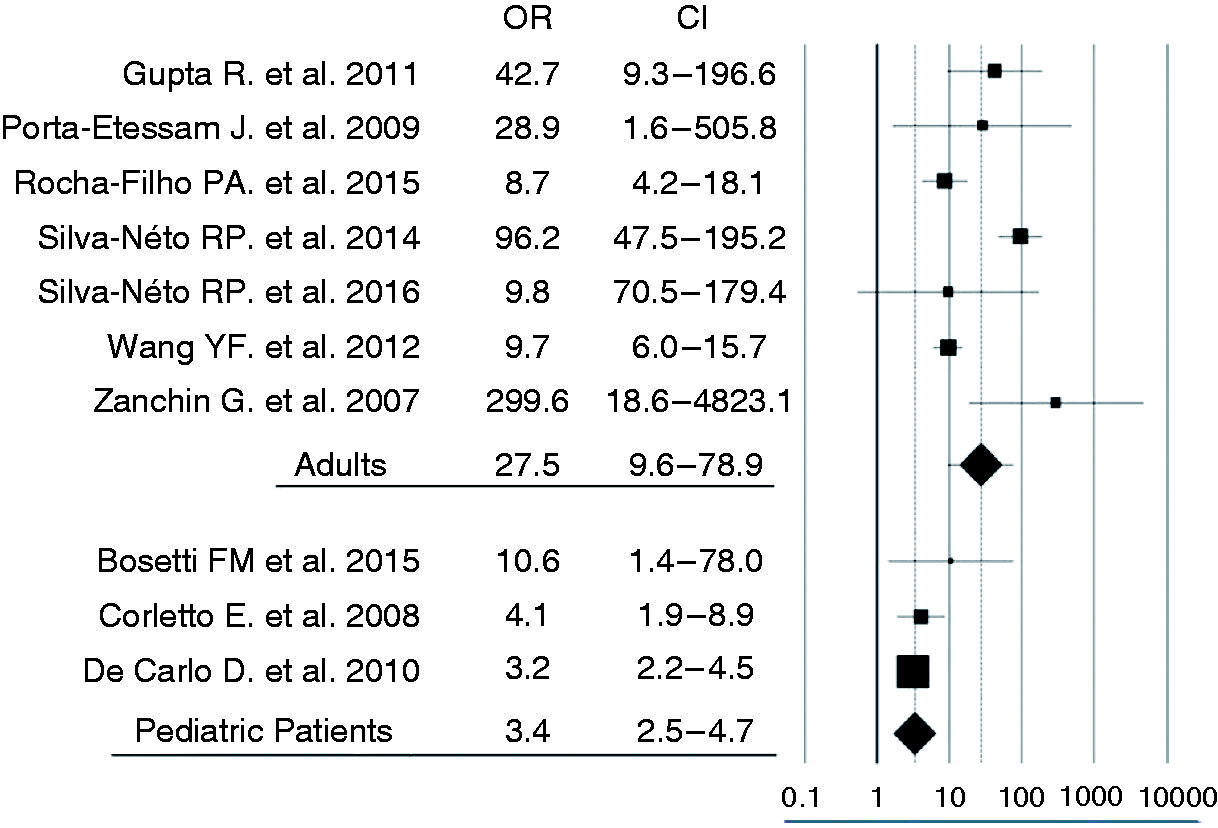
Discussion
In the last 12 years, interest in the relationship between olfaction and M increased much more than in previous years, as demonstrated by the number of papers dealing with Os published after 2003. This sprouting of literature is probably related to the stimulus given by the insertion of Os in the ICHD II Appendix. In our opinion, this can be a demonstration of the importance of the Appendix in promoting research on selected topics.
Many aspects of olfaction and M have been studied: possible altered perception of smell in migraineurs (51,60,74), the neuroanatomical circuit linking M and olfaction (61,75–77), odor triggers (44,49,64,78,79), association with other symptoms (47,52,69), clinical relevance of Os in the psychophysical health of migraineurs (29,32,48,52,57,73).
Given the aim of this review article, we focused our attention on the diagnostic relevance of Os. All papers (29,31,32,35,37,39,41 in adults; 28,36,38,40 in pediatric patients) considering this aspect reported a higher prevalence of Os in M than in other primary headaches, particularly when compared with TTH both in adults and in children.
Prevalence of Os is highly variable in the different studies. Variability is more evident in M than in TTH: This finding could be partially attributed to the higher number of studies investigating this symptom in M than in TTH. However, many other influences may contribute to this variability. In part, it could be due to the difficulty encountered in investigating this symptom: indeed, anamnestic interview about the presence of Os may not be easy, even in adults, both for its important subjective “hedonic” component and for the interfering presence of nausea, which may lead investigators to underestimate or, on the contrary, overestimate the presence of Os. Again, bias among different authors may only partially explain the variability of results, since the same research group finds the highest and the lowest prevalence of Os in two different articles (31,44).
Another possible explanation for the variability in the reported prevalence of Os may be linked to the differences among selected patients, such as sex and age distribution (29,31,32,39,52,68), type of M or TTH (32,36–39,47,52) or possible comorbidity of M and TTH. Finally, as suggested by Wang et al. (32) and Saisu et al. (60), the ethnic group may influence the prevalence of Os, since it has been observed that olfactory acuity is different in different ethnic groups both for genetic and epigenetic factors (80,81), and some authors suggest a possible higher odor sensitivity in Asian patients (81,82).
Our sub analysis of data on M patients demonstrates a prevalence of Os that differs significantly among countries (Europe, USA, Australia versus Latin-American versus Far East countries). The prevalence in Latin American and Far East countries is particularly high, although the result of our analysis may suffer a bias, since a single article by Wang et al. (32) is the source of more than 70% of Asian migraineurs. The same holds true in a similar sub-analysis we make of TTH patients, demonstrating a higher prevalence of Os in non-Western sufferers, and particularly in Asian sufferers: This result may also suffer a bias, since 80% of Asian TTH sufferers are studied in a single paper by Chu et al. (53).
Focusing on the 16 articles that analyze Os usefulness in the differential diagnosis between M and TTH, despite some differences in method, style or strength, all authors conclude that this symptom should be used in clinical practice. In some articles, a crystal-clear association is demonstrated between Os and other M symptoms (30–32,36,38,52) such that the more migrainous accompanying symptoms an M patient reports, the more they are likely to experience Os during the attack. We believe that this evidence, supporting the proposition that Os may be seen as typical of migraineurs, can be summed up in a statement: “The more migrainous, the more osmophobic”.
Different but even, is the relevance of Os in juvenile patients: De Carlo et al. report that the presence of Os predicts the evolution to M within three years in the majority (62%) of children whose headaches were formerly classified as TTH. Authors conclude that “the detection of osmophobia in children affected by TTH correlated with a greater likelihood (OR: 5.6) of evolution to migraine compared with children with TTH without osmophobia”, confirming the prognostic importance of Os, being considered “one of the most relevant predictors of evolution from TTH to migraine at a 3-year follow-up in children” (33). For this reason, in children Os could be considered as the “herald of migraine”.
To evaluate the usefulness of Os in M diagnosis, some authors calculated sensitivity and specificity values for this symptom in differential diagnosis with TTH.
While Wang et al. (32) and Silva Neto et al. (31) found quite a high sensitivity, Zanchin et al. (39) in adults and Corletto et al. (38) in children demonstrated a low sensitivity of Os in differential diagnosis between M and TTH. Rocha-Fillo et al. (29) found intermediate values instead, comparable with those in our global analysis on pooled data (Table 5).
As far as specificity values of Os are concerned, in the literature they are consistently very high, both in adult and pediatric patients (range 87.5 to 100%), leading authors to confirm the usefulness of Os for M diagnosis and to support its insertion among the ICHD criteria. Only one study in adults found different results: Wang et al. (32), studying 2331 Taiwanese patients, showed a relatively low (69%) specificity of Os in differentiating M vs TTH, concluding that Os alone has a limited diagnostic value, being more useful for its high NPV. Nevertheless, they support the inclusion of this symptom in a revised alternative diagnostic panel for M. As a possible explanation, we believe that the specificity value calculated in this article, which is not inferior to the specificity values of phonophobia reported in the same paper, may be ascribed mainly to the high prevalence of Os found by the authors in TTH patients, possibly in relation to their ethnic origin, as hypothesized above. In conclusion, even if with some differences, all the authors suggest the insertion of Os in the ICHD as a diagnostic criterion for M.
Despite the general agreement on this point, only a few articles analyze how Os should be included in the ICHD. Some papers studied the applicability of the criteria for M proposed in the ICHD II Appendix A1.1 and evaluated the diagnostic concordance between these and the ICHD II criteria. The reliability of the A1.1 criteria was high, with an M diagnostic concordance with the ICHD II criteria ranging between 96 and 98% (32,36,42) both in adults and pediatric patients.
Kelman, Zanchin et al. and De Carlo et al. in particular support the usefulness of the ICHD II A1.1 criteria for M. The first author demonstrates a high concordance in M diagnosis between the ICHD II and ICHD II Appendix A1.1 criteria, with 98.3 % of adults classified as M with the two methods (42). De Carlo et al. report in children a comparable diagnostic capacity between the ICHD II and ICHD II A1.1 criteria (96.2%), and relates the small difference observed to the ability of the A1.1 criteria to re-classify patients in which diagnosis was uncertain rather than to a diagnostic deficiency of these criteria (36).
On the other hand some authors, while supporting the insertion of Os in ICHD, are in favor of a revision of the ICHD A1.1 criterion D, proposing that this should be fulfilled in the presence of nausea/vomiting or of two among phonophobia/photophobia/Os (32,42).
Our statistical analysis of the literature further supports a role for Os in M diagnosis. Besides confirming low-moderate values of sensitivity in adults, and especially in pediatric patients (51.4 versus 22.1%), particularly relevant is the demonstration of high specificity and PPV of Os in the differential diagnosis between M and TTH (specificity 94.1 versus 92%; PPV 96.1 versus 82.6%). Despite being lower than those obtained in some of the published articles, the values of specificity calculated from the pooled data are so high that it is possible to say that, when present, Os is a good clinical marker for M.
This is even more the case if we consider that the variability in the reported specificity in the differential diagnosis between M and TTH may be linked to the differences among selected patients, such as sex and age distribution, type of M or TTH or, particularly, to bias due to a possible comorbidity of M and TTH. Indeed, among the 10 papers reporting precise data about the differing prevalence of Os in M versus TTH (29,31,32,35,37,39,44 in adults; 28,36,38 in pediatric patients), only five excluded patients presenting both M and TTH (31,35,38,39,44), one considered patients with both M and TTH as migrainous patients (32) and four (28,29,36,37) did not mention the comorbidity issue.
Moreover, comparison of the diagnostic values of Os calculated in our global analysis with those reported in the literature for other accompanying symptoms used as diagnostic criteria for M can further underscore the worth of our results. Sensitivity values appear lower than those of the other M accompanying symptoms such as phonophobia and photophobia, particularly in pediatric patients; however, when focusing on specificity and PPV, the comparison suggests that, both in adults and pediatric patients, the specificity and PPV of Os are higher than those of phonophobia or photophobia alone and, in some series, comparable to the values of these two symptoms combined or, particularly in adults, comparable to nausea (25,31,32,83–85).
In conclusion, although we believe that the debate should remain open about how to formally insert Os in the ICHD classification, its diagnostic relevance remains unequivocal. On this ground, it appears that the choice of removing Os from the ICHD 3 beta version without explanation is not in keeping with the published data and should be revised. In general terms, it is desirable that in the future a possible modification of the ICHD would be motivated.
Clinical implications
Os shows a higher prevalence in M than TTH both in adults (48.5 versus 8.9%) and pediatric patients (23.4 versus 7.9%). Os prevalence in M is significantly higher in adulthood. The specificity and PPV of Os are very high in M both in adults and pediatric patients (specificity 94.1 versus 92%; PPV 96.1 versus 82.6%) and support the usefulness of this symptom in differential diagnosis between M and TTH. An ethnic variability in the prevalence of Os is possible and should be further investigated. Although more studies are needed to better determine how Os should be inserted within the criteria for M diagnosis, in keeping with the published data Os deserves a place in the ICHD as a useful clinical marker of M. Therefore, the choice in the ICHD 3 beta to remove Os from the ICHD II Appendix should be revised.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.