
Abstract
This study was planned to investigate the prevalence of osmophobia in juvenile headache sufferers and to analyse the diagnostic utility of osmophobia in order to distinguish migraine without aura from episodic tension-type headache. We examined 305 consecutive patients presenting at our Paediatric Headache Centre. A semistructured questionnaire was given to 275 selected patients affected by migraine or tension-type headache. The prevalence of osmophobia during attacks was 18.5%, mainly in migraine patients (25.1%) vs. those with tension-type headache (8.3%). Osmophobia showed more specificity than phonophobia or photophobia in the differential diagnosis between migraine and tension-type headache. In conclusion, this study demonstrates that osmophobia resulted in a symptom with poor sensitivity (27.1%) but high specificity (92%) that could become a supportive diagnostic criterion even in children for the differential diagnosis between migraine without aura and tension-type headache.
Keywords
Introduction
In the last revision of the International Classification of Headache Disorders (ICHD-II) (1), the accompanying symptoms of phonophobia, photophobia, nausea and vomiting remain an essential part of the differential diagnosis between migraine and tension-type headache (TTH). In the appendix of this classification (point D), it was hypothesized that osmophobia could be introduced among diagnostic criteria of migraine without aura (MoA): in fact, the proposal is that in MoA two of the following five symptoms must be present: phonophobia, photophobia, nausea, vomiting and osmophobia (1). This last symptom has also been proposed as an additional factor in MoA diagnosis by the Canadian (2) and Italian (3) Societies for the Study of Headaches.
Several studies published on this topic have suggested that this further diagnostic criterion could be useful in clinical practice (4–6).
The term osmophobia refers to an unbearable perception of odours that are non-aversive or even pleasurable outside the attacks (5, 6). However, the relationship between the sense of smell and migraine has been known since ancient times (7).
Data regarding the relationship between osmophobia and primary headaches in adults have been accumulating (5–11); despite this, only one preliminary study has examined the relationship between osmophobia and primary headaches in children (12). However, migraine represents an important problem for the juvenile population, with a high prevalence in children and especially in adolescents (5–15%) (13) and with a strong impact on the quality of life (14).
The peculiar features in juvenile headaches subtypes (15–18), the complexity of differential diagnosis due to the modification of symptoms during development (19, 20) and the child's inability to describe the symptoms accurately (21) are all factors that confirm the ability to analyse the role of osmophobia in the differential diagnosis between the subtypes of primary headaches in children.
The aim of this study was to analyse the relationship between osmophobia and the two major subtypes of primary headaches in juvenile patients, with the goals of: (i) ascertaining the prevalence of the symptom in migraine and tension-type headache, (ii) identifying the clinical characteristics of osmophobia in juvenile patients, (iii) evaluating its relationship with age and gender of young patients and (iv) verifying the diagnostic utility of osmophobia in the differential diagnosis between MoA and episodic tension-type headache (ETTH), because these two types of primary headache present a greater overlap of phenotype (22).
Materials and methods
The study was conducted between January and July 2005. Patients were recruited from out-patients of our specialized Centre for diagnosis and therapy of headache in childhood and adolescence. Selection was based on the following criteria: (i) age 6–17 years, (ii) diagnosis of one of the four following subtypes of primary headache: migraine with aura (MA), MoA, ETTH and chronic tension-type headache (CTTH), in accordance with ICHD II criteria (1), (iii) no prophylactic therapy, (iv) absence of important and/or chronic diseases and (v) adequate cognitive and expressive skills to understand the questionnaire and take part in the interview. Patients with the following conditions were excluded: (i) diagnosis of any other type of primary headache, (ii) diagnosis of secondary headaches and (iii) diagnosis of primary headache but with a mixed pattern of migraine and TTH.
During the examination a structured family and personal case history was compiled for each child, and an accurate physical and neurological examination was performed. For each patient, a specialist completed a preprepared questionnaire with the clinical history of the headache: age of onset, family history for headache and complete pattern of the attacks. At the end of the visit, a second-level diagnosis of migraine or tension-type was made and only those patients who fulfilled the inclusion criteria were enrolled.
For this last group a semistructured questionnaire on osmophobia was completed. In agreement with other authors (6), we defined osmophobia as an unbearable perception, during a headache attack, of odours that are non-aversive or even pleasurable outside the attacks. We asked about the following main characteristics of this disturbance: (i) timing of the osmophobia according to: the attack (before or during), the duration (hours or minutes) and the frequency of the symptom; (ii) onset of the osmophobia regarding the headache history; (iii) kind of smell (food, perfumes, smoke and other); and (iv) possible triggering smells.
This interview and the diagnostic questionnaire for headache were given to the patient during the examination and were mainly based on the answers of the patients, with the help of the accompanying parent.
Blood tests or diagnostic neuroimaging were used where indicated to rule out secondary headaches. Personal information of all patients was included in our database and privacy was guaranteed by omitting the patient's name during data input for statistical processing.
The data were collected in a database (Microsoft Excel®) and then processed using
The study included descriptive statistic analyses; the χ2 test was used to assess the relationship between nominal variables, and the t-test was used to compare means in independent samples. The levels were considered significant with a value of P < 0.05. In addition, sensitivity, specificity and positive and negative predictive values were calculated for each different accompanying symptom.
Results
Demographic and clinical specifications
Of 305 consecutive patients, we excluded 30 subjects affected by: other primary headaches (n = 20), secondary headaches (n = 4) and not classifiable headaches (n = 6). A total of 275 patients were enrolled, aged 6–17 years (mean 11.2 ± 2.8 years), 158 female (57.5%) and 117 male (42.5%).
In accordance with the headache classification (1), 167 patients (60.8%) suffered from migraine: in 144 patients (52.4%) the diagnosis was MoA, in 23 (8.4%) it was MA. The remaining 108 patients (39.2%) were affected by TTH, divided into ETTH (n = 88, 32.0%) and CTTH (n = 20, 7.2%) (Table 1).
Distribution of headache subtypes in the study population
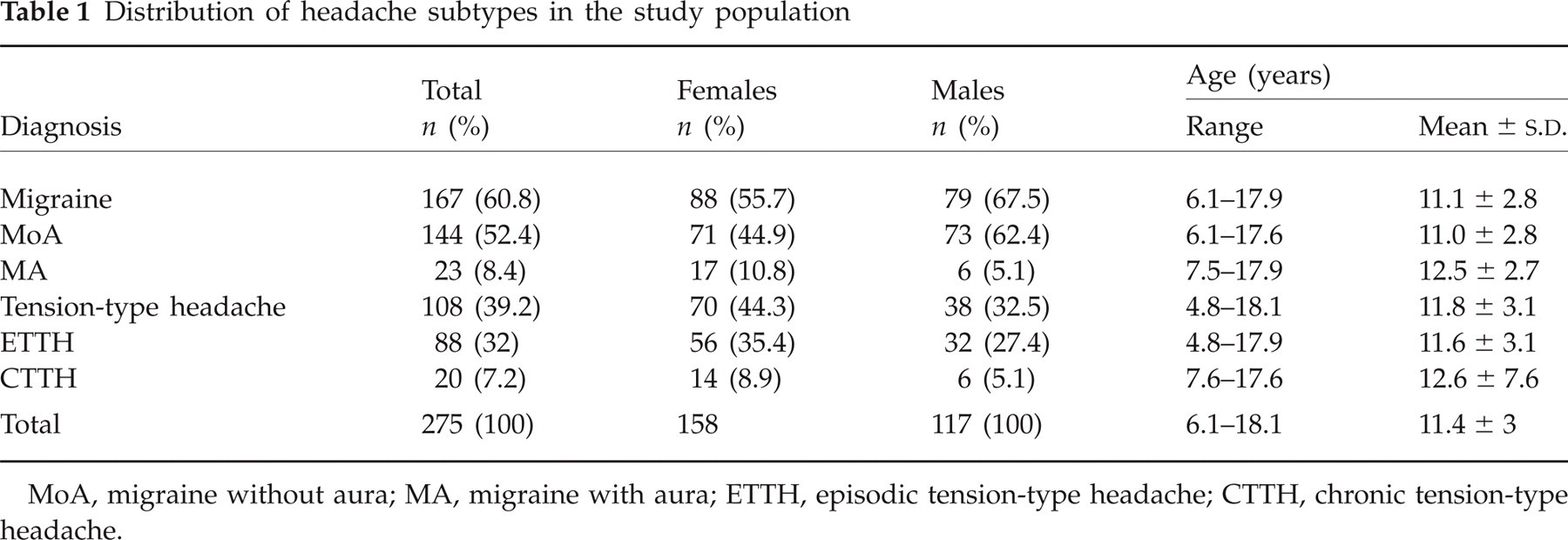
MoA, migraine without aura; MA, migraine with aura; ETTH, episodic tension-type headache; CTTH, chronic tension-type headache.
Osmophobia and type of headache
Of the 275 patients, 51 (18.5%) reported osmophobia during attacks: 25.1% of the migrainous group, 8.3% of TTH group (P < 0.05).
Moreover, dividing the two main groups into four diagnostic subgroups, osmophobia was found in 27.1% (39/144) of MoA and in 13.0% (3/23) of MA, in 8.0% (7/88) of ETTH and in 10.0% (2/20) of CTTH (Table 2). Furthermore, with the aim of evaluating whether the TTH in our patients could have an important link with migraine, we divided the 108 patients with TTH into two groups: patients with and patients without osmophobia. The family history for migraine was analysed in both groups. A significant difference was observed: 77.7% (7/9) of osmophobic patients presented a positive family history for migraine compared with 43.4% (43/99) of the non-osmophobic group (P < 0.05).
Prevalence of osmophobia according to diagnosis in subtypes of primary headache

MoA, migraine without aura; MA, migraine with aura; ETTH, episodic tension-type headache; CTTH, chronic tension-type headache.
Role of gender and age in the prevalence of osmophobia
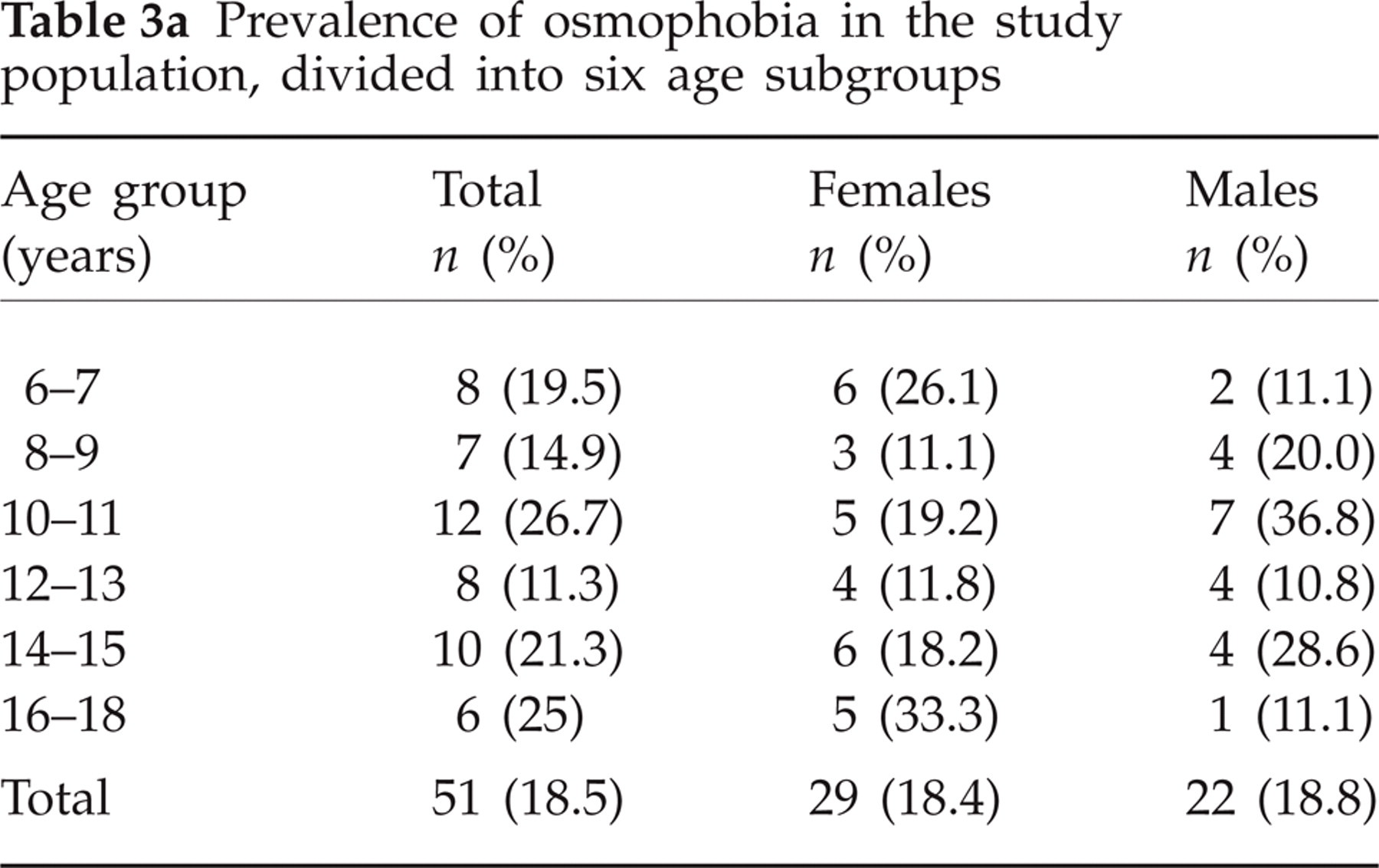
No significant difference was found between patients with osmophobia regarding distribution by gender (male 18.4% vs. female 18.8%) or by age (Table 3a). In particular, no significant differences were found between prepubertal and postpubertal children (P = 0.28 in boys, P = 0.87 in girls) (Table 3b).
Prevalence of osmophobia in the study population, divided into six age subgroups
Prevalence of osmophobia in prepubertal and postpubertal children

Postpubertal age: in boys > 12 years, in girls > 11 years.
Characteristics of osmophobia
Osmophobia was reported before the attacks in 5.9% (3/51) of patients, before and during the attacks in 13.7% (7/51), during the attacks in 80.4% (41/51); no patient reported osmophobia after the resolution of the algic phase.
As regards personal history of headache, an altered perception of smells was usually described as a very early onset symptom, with the mean age at the onset of osmophobia (8.1 ± 3.3 years) greatly overlapping the mean age at the onset of headache symptomatology (8.1 ± 2.7 years). The frequency of osmophobia was described to be ‘always’ present in 72.8% of attacks, ‘often’ in 13.4% and ‘rarely’ in 13.8%.
The smell types that were reported with greater frequency were perfumes (63%), followed by food odours (53%) and tobacco smoke (30%). Lastly, all patients who reported odour as a trigger also reported osmophobia during attacks: the smell stimulus triggered the headache attacks in 12/51 of cases (23.5%) and in 11/42 of patients with migraine (26.2%) and in 1/9 of patients affected by TTH (11.1%).
Osmophobia and its relation to other symptoms
Osmophobia had a higher prevalence in the migraine group (25.1%) compared with patients with ETTH (8.3%, P < 0.0001). The same was true for photophobia (77.2% vs. 38.9%, P < 0.0001), nausea (73.0% vs. 5.5%, P < 0.0001), vomiting (46.7% vs. 0%, P < 0.0001) and phonophobia (72.5% vs. 56.5%, P < 0.02).
Moreover, among the 51 osmophobic patients, an association with at least three other symptoms was recognizable in 32 cases (63%), all suffering from migraine, and in no patient affected by TTH.
Diagnostic role of osmophobia
If the sensitivity and specificity values are calculated of the three possible associated symptoms (phonophobia, photophobia and osmophobia) required for the differential diagnosis of MoA and ETTH, osmophobia proved a symptom of poor sensitivity (27.1%), but very specific (92%), with a specificity greater than that of photophobia (61.4%) or phonophobia (45.5%) (Table 4). Specificity in diagnosing MoA was even greater when this symptom was associated with photophobia (95.5%).
Sensitivity and specificity of accompanying symptoms in patients affected by migraine without aura or episodic tension-type headache
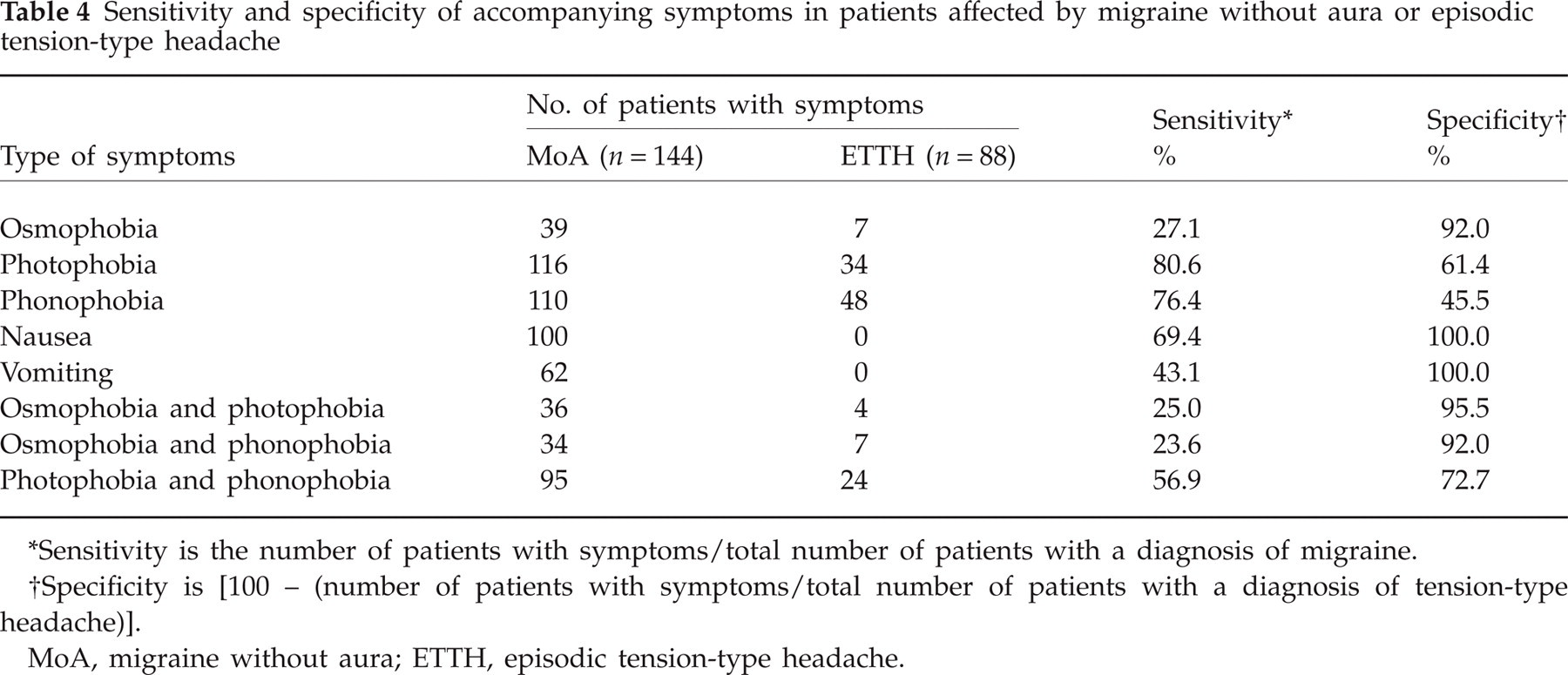
Sensitivity is the number of patients with symptoms/total number of patients with a diagnosis of migraine.
Specificity is [100 – (number of patients with symptoms/total number of patients with a diagnosis of tension-type headache)].
MoA, migraine without aura; ETTH, episodic tension-type headache.
Considering the positive predictive value (i.e. the probability of an osmophobic patient suffering from migraine as diagnosed from the presence of the analysed symptom), osmophobia showed a greater value (82.3%) when compared with photophobia (74.1%) or with phonophobia (65.5%), occupying third place after vomiting (100%) and nausea (95.3%) (Table 5).
Positive predictive value (PPV) and negative predictive value (NPV) of various accompanying symptoms for the diagnosis of migraine

TTH, tension-type headache; PPV, the probability of a diagnosis of migraine, given the presence of the symptom in question; NPV, the probability of a diagnosis other than migraine, given the absence of the symptom in question.
Discussion
This is the first systematic study on osmophobia in juvenile primary headache sufferers, and results are in agreement with the research data on adults patients (5–10, 23, 24). In this latter group, data have been recently reported (6) in an attempt to validate the possible diagnostic utility of osmophobia in the differential diagnosis of migraine from TTH, in accordance with the appendix of the ICHD-II classification (1).
After the first analysis of Blau and Solomon (8), which observed osmophobia in 40% of migrainous adults during attacks, recent studies in the adult population have reported a prevalence of this symptom of between 24.7% and 47.7% of cases (5–10, 24). A previous study in adults (25) reported that hypersensitivity to odours may be found even in TTH, although with a much lower frequency than in migraine (13% vs. 46%). However, a recent study in a larger and ‘pure’ population (i.e. MoA, MA and ETTH groups, without any patients with other concomitant forms of headache) has shown that osmophobia is reported during an attack only by migraine patients and not by those with ETTH (6).
In the paediatric population osmophobia was reported in 20% of migraineurs, with a slight prevalence in males, whereas this symptom did not occur in the other headache groups studied, i.e. patients affected by primary stabbing headache, ETTH and CTTH, or secondary headaches (12).
In our study, the prevalence of osmophobia in young migrainous patients was similar (25.1%), but it was also seen in a minority of patients affected by TTH (8.3%). The presence of osmophobia in a small subgroup of our children with TTH has to be seen in the context that this form of headache may change to migraine during development. In childhood, the transformation from one form of primary headache to another has been demonstrated in a long-term follow-up study and, specifically, the evolution of TTH to MoA was seen from 8.9% (26) to 20.7% (20) and 38% (27).
One possible explanation for this changing pattern of childhood headache is the ‘continuum severity theory’, which considers primary headache a continuum between TTH and migraine (27). Another possibility is that this subgroup of young patients, presenting as TTH according to ICHD-II criteria (1), could be migraineurs who have not yet developed a full pattern of migraine. If so, osmophobia in phenotypically tension-type children could be the heralding symptom of migraine. Of course, this is just a hypothesis and will be verified only by following prospectively a cohort of such patients.
In our study, osmophobia was well integrated in the medical history of our young patients: it appeared early at the onset of their headache history and often lasted for the entire duration of the attack, in agreement with a recent study on adults (6).
It is known that in the adult population exposure to intense odours can trigger a migraine attack (8, 28–31), mainly in osmophobic patients (7, 24). In our 51 juvenile osmophobic subjects, smell stimulus triggered an attack much more frequently in migrainous patients, rather than in those affected by TTH. A previous study in a limited series of adult patients has reported that odours can trigger not only migrainous (61%), but also tension-type (24%) attacks (32). Recently, in adult migrainous patients, a high prevalence of interictal olfactory hypersensitivity was significantly associated with the presence of odour-triggered migraine, whereas no control subject presented such hypersensitivity (33). In order to understand how osmophobia is age-related, some authors have analysed migraine characteristics stratified by age in a large cohort of patients: osmophobia and perfume as a trigger of attacks from 16 to ≥ 50 years did not show any particular correlation with age (34). The strong association of several autonomic symptoms in our young osmophobic patients is a possible expression of increased cortical excitability in migraine patients (35) and might indicate widespread depression of central inhibitory mechanisms (36).
Recently, in a wide-scale study of migrainous children, the increased specificity of the new version of ICHD II (1) with respect to the previous version (International Headache Society) (37) was confirmed, despite the poor sensitivity (38). However, the modifications of the diagnostic criteria for paediatric migraine (i.e. the duration of an untreated attacks reduced to 1 h and the possible bilateral fronto-temporal location) could increase the overlap between the two most common type of primary headache, MoA and ETTH.
In our population, the analysis of the prevalence of osmophobia with regard to the other four associated symptoms confirms that it represents a more specific factor for the diagnosis of migraine than phonophobia or photophobia, as previously reported (4, 6, 36). Results from this first systematic study of osmophobia in childhood primary headaches are in general agreement with the adult literature, except for some differences. In children, osmophobia is prevalent in migrainous patients rather than in those affected by TTH with a ratio of 3:1. In our sample, osmophobia proved specific enough for the diagnosis of migraine, representing an additional diagnostic criterion in the differential diagnosis between MoA and ETTH even in childhood, as demonstrated in adult patients (6, 34).
This study presents some limitations due to the small size of our study population, the different sizes of the groups studied and the bias in selection of the patients that came to a third-level specialized centre. Nevertheless, this study lays the groundwork for future research on a larger population, with a prospective analysis of the complex relationship between osmophobia and different forms of primary headaches in juvenile patients.
Of note, a recent review (39) has highlighted the importance of olfactory disorders in a wide range of neurological disease and the relevance of their evaluation for diagnosis.