
Abstract
Background
Vestibular migraine (VM), the common term for recurrent vestibular symptoms with migraine features, has been recognized in the appendix criteria of the third beta edition of the International Classification of Headache Disorders (ICHD-3β). We applied the criteria for VM in a prospective, multicenter headache registry study.
Methods
Nine neurologists enrolled consecutive patients visiting outpatient clinics for headache. The presenting headache disorder and additional VM diagnoses were classified according to the ICHD-3β. The rates of patients diagnosed with VM and probable VM using consensus criteria were assessed.
Results
A total of 1414 patients were enrolled. Of 631 migraineurs, 65 were classified with VM (10.3%) and 16 with probable VM (2.5%). Accompanying migraine subtypes in VM were migraine without aura (66.2%), chronic migraine (29.2%), and migraine with aura (4.6%). Probable migraine (75%) was common in those with probable VM. The most common vestibular symptom was head motion-induced dizziness with nausea in VM and spontaneous vertigo in probable VM. The clinical characteristics of VM did not differ from those of migraine without VM.
Conclusion
We diagnosed VM in 10.3% of first-visit migraineurs in neurology clinics using the ICHD-3β. Applying the diagnosis of probable VM can increase the identification of VM.
Introduction
Migraine is a common episodic or chronic neurological disorder, and is listed as the seventh leading cause of disability by the World Health Organization (1,2). Vertigo or dizziness occurs in 4%–51.7% of patients with migraine, and this association decreases the migraineur’s quality of life (3–5). Many illnesses, such as Ménière’s disease, somatoform vertigo, benign paroxysmal positional vertigo, transient ischemic attacks, syncope and orthostatic hypotension, vestibular paroxysmia, and episodic ataxia type 2 can cause vertigo or dizziness in patients with migraine (6–8). Among these, vestibular migraine (VM) or migrainous vertigo is recognized as a frequent and important cause of recurrent vertigo in patients with or without migraine (9–12).
Previous terms that described the specific association between migraine and vestibular symptoms include migrainous vertigo, migraine-associated dizziness or vertigo, migraine-related vestibulopathy, and benign recurrent vertigo (3,13,14). Consensus diagnostic criteria for VM and probable VM were published by the Barany Society’s Classification of Vestibular Symptoms and the International Headache Society (IHS) after a lengthy process (14–16). Vertigo was previously considered by the second edition of the International Classification of Headache Disorders (ICHD-II) to be only an isolated symptom in benign paroxysmal vertigo of childhood or an aura in basilar-type migraine (17). For research purposes, VM is now accepted in the appendix criteria of the third beta edition of the ICHD (ICHD-3β) as a disease entity (18).
The prevalence of VM based on various diagnostic criteria is 4.7%–29.3% in otolaryngology or dizziness clinics, but the prevalence of VM in headache or neurology clinics is not well known (11,14,19,20). One research group found that the prevalence of migrainous vertigo was 9% in a migraine clinic, and another group reported that 11.9% of patients with migraine in a headache clinic met the criteria for migrainous vertigo (4,14). Although the use of “VM” implies that the disease entity shares mechanisms with migraine, VM is underdiagnosed or unrecognized as a migraine subtype (3,21,22). Furthermore, the ICHD-3β diagnostic criteria for VM require five episodes of vestibular symptoms, but the previous criteria for migrainous vertigo required episodic or recurrent vestibular symptoms (14,17,18). Therefore, the prevalence of VM in headache or neurology clinics should be assessed using the ICHD-3β. In addition, the consensus diagnostic criteria for probable VM according to the Barany Society and the IHS are not included in the ICHD-3β; thus, probable VM should be assessed with field-testing of the ICHD-3β.
We conducted a prospective cross-sectional multicenter headache registry study in Korea to assess the prevalence and clinical characteristics of VM based on ICHD-3β criteria and of probable VM based on consensus diagnostic criteria.
Methods
This study was based on a headache registry using the ICHD-3β for first-visit patients (HEREIN) study. The HEREIN study was a cross-sectional, multicenter headache registry study that used prospectively collected data obtained from consecutive first-visit patients with headache treated at the neurology outpatient departments of 11 hospitals in Korea between August 2014 and February 2015 (submitted). Among these 11 hospitals, nine hospitals joined this sub-study to assess the prevalence of VM; we selected patients with a primary headache disorder from the nine hospitals for this analysis.
The study design was proposed and reviewed in the regular educational meeting of the Korean Headache Society (KHS) after an application request for the ICHD-3β. This study was conducted at seven university hospitals (five tertiary referral hospitals and two secondary referral hospitals) and two general hospitals (secondary referral hospitals) throughout Korea (Seoul: four; Daejeon: one; Gyeonggi-do: two; Gangwon-do: one; Gyeongsangnam-do: one) in accordance with the Declaration of Helsinki and Good Clinical Practice. Consecutive patients visiting outpatient clinics for headache for the first time were enrolled in the present study by nine neurologists, and one neurologist managed the entire dataset. Board-certified neurologists with a special interest in the headache field conducted the study: Seven were directors on the KHS Board and the remaining two completed a headache or stroke fellowship.
Participants who complained of headache as the main reason for their outpatient visit included Koreans aged 19–100 years without any communication disabilities that would preclude taking a proper history. Exclusion criteria were the presence of other chief complaints besides headache; not Korean; significant communication issues related to hearing, speech, or cognition; and any other serious medical or psychiatric condition based on a physician’s evaluation.
This study protocol and informed consent or a use-of-information agreement form were reviewed and approved by the Institutional Review Board of each center. Each patient provided written informed consent prior to participating in the study or waived informed consent according to the decision of the Institutional Review Board of each center. The population for the inter-rater reliability calculation was composed of randomly selected individuals (n = 17) who participated in the study. The corresponding investigator presented clinical summaries of the cases at two regular consensus meetings. Each investigator independently reviewed the structured clinical summaries and subsequently reported the diagnosis by email. We assessed the level of inter-rater agreement with a simple categorical diagnosis (i.e. VM vs. others, VM or probable VM vs. others). We used Fleiss’ kappa values for the inter-rater reliability calculation.
Assessment of the VM diagnosis using the ICHD-3β
After an instructional meeting regarding use of the ICHD-3β, the headache disorders were classified according to these criteria by each investigator based on patient history, a neurological examination, and laboratory or neuroimaging studies, if needed. Cases that were difficult to diagnose were evaluated during the regular consensus meeting. The diagnosis of primary headache disorder was specified up to at least the second digit.
We also obtained a comprehensive neuro-otological history from and performed neurological examinations on all patients with migraine. The detailed interview for diagnosing VM included questions about clinical features (e.g. main type of vertigo and duration, frequency, severity, and history of migraine) according to the ICHD-3β and concomitant symptoms.
Diagnostic criteria for VM.

VM: vestibular migraine; ICHD-3: the third edition of the International Classification of Headache Disorders.
We assessed the prevalence of VM based on the ICHD-3β and that of probable VM based on previous consensus criteria (3,5). The main type and duration of vertiginous episodes were recorded. Vestibular symptoms were defined by the Barany Society’s Classification of Vestibular Symptoms (15). The patients chose one of the five main vestibular symptoms that qualified for a VM diagnosis, including spontaneous vertigo, positional vertigo, visually induced vertigo, head motion-induced vertigo, and head motion-induced dizziness with nausea. The duration of a vestibular episode was defined as the amount of time in which the attack lasted. The episode duration was defined as the total period during which short attacks recurred for patients in whom a vestibular episode tended to occur repeatedly during head motion, visual stimulation, or a head position change (18). The demographic and vestibular data of the patients diagnosed with VM were assessed and compared with those of patients with probable VM. Additionally, the clinical characteristics of patients with VM, including probable VM, were compared to identify patients who met the criteria for migraine but not for VM (non-VM).
Statistics
SPSS for Windows, version 21.0 (IBM Corp., Armonk, NY, USA) software was used for the statistical analysis, and a p value < 0.05 was considered significant. Comparisons of the demographic and clinical data across diagnostic categories were performed with Student’s t-tests for parametric data and the Mann-Whitney test for non-parametric data. Categorical data were analyzed using chi-square statistics. We used Fleiss’ kappa value to calculate inter-rater reliability. The guidelines suggest that Fleiss’ kappa values >0.81 indicate excellent agreement, those of 0.80–0.61 indicate substantial agreement, those of 0.60–0.41 indicate moderate agreement, those of 0.40–0.21 indicate fair agreement, those of 0.20–0.01 indicate slight agreement, and those less than zero indicate poor agreement.
Results
Prevalence of patients with VM and probable VM
Of the 1627 patients in the HEREIN study, 1414 patients were included in the present study. No difference in age (47 vs. 46 years), proportion of females (62.6% vs. 65.9%), or proportion of migraineurs (42.9% vs. 41.2%) were found between the 1414 patients included in the VM study and the remaining 213 patients. According to the ICHD-3β criteria, 1231 patients suffered from primary headaches, classified as 1–4; 114 suffered from secondary headaches, classified as 5–12; and 69 suffered from other headaches, classified as 13–14 (Figure 1). The group with primary headaches included 631 patients with migraine, 375 with tension-type headache, 19 with trigeminal autonomic cephalalgia, and 206 with other primary headache disorders. Of the 631 migraineurs, 355 (56.3%) had migraine without aura, 40 (6.3%) had migraine with aura, 135 (21.4%) had chronic migraine, and 101 (16.0%) had probable migraine.
Algorithm of the VM classification used in this study. VM: vestibular migraine; ICHD-3β: the third beta edition of the International Classification of Headache Disorders.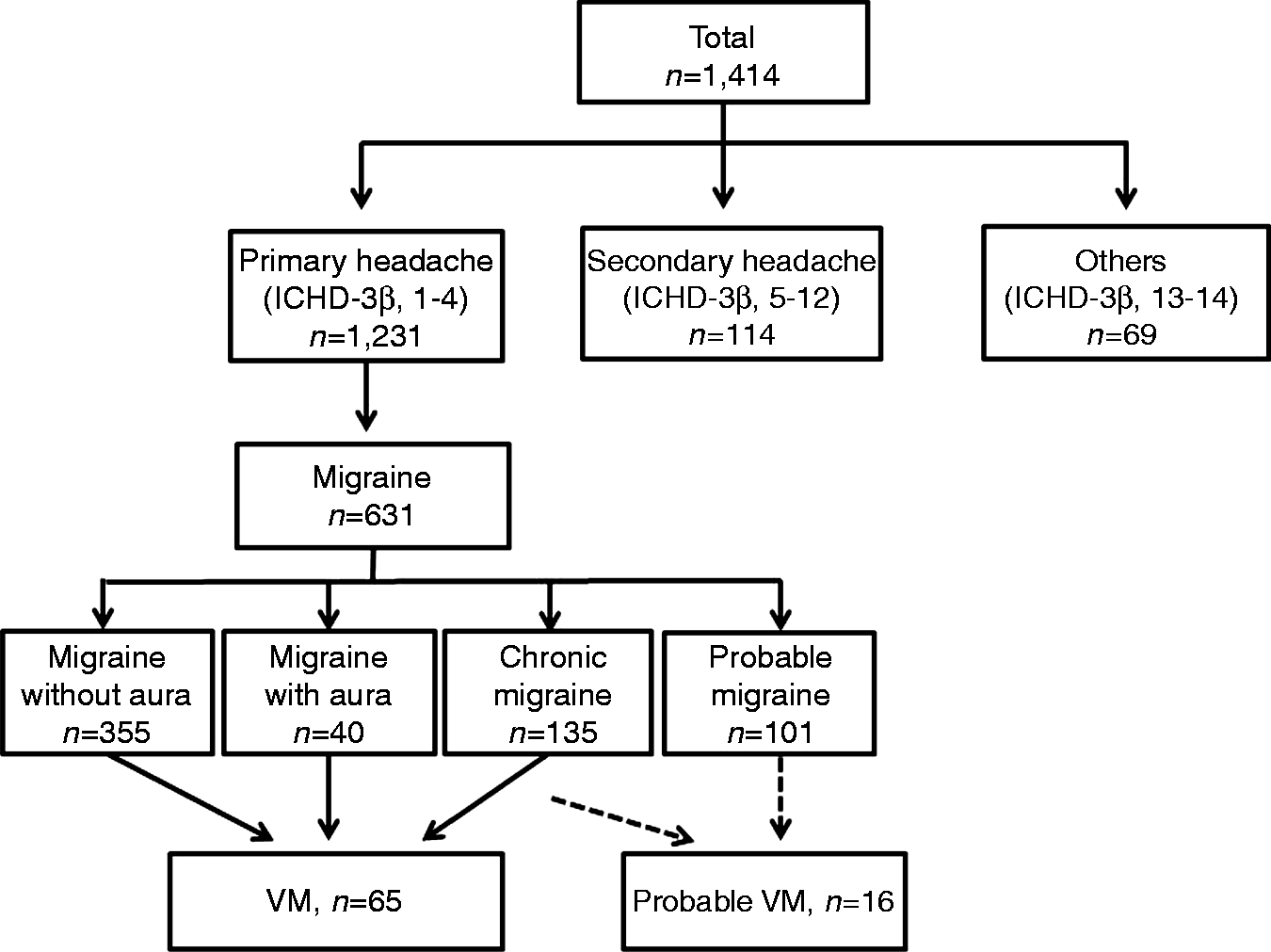
In addition, 65 patients were classified as having VM, and 16 patients were classified as having probable VM. Among the migraineurs, the frequencies were 10.3% for VM and 2.5% for probable VM (4.6% and 1.1%, respectively, of the total sample). The frequency of VM was 1.1%–17.2% in seven university hospitals and 5.3%–8.9% in two general hospitals. The frequencies of VM were 5.3%–15.2% in four secondary referral hospitals and 1.1%–17.2% in five tertiary referral hospitals.
The frequency of VM differed according to migraine subtype. Comparisons of the frequencies of VM according to the four migraine subtypes revealed that the most common group was chronic migraine in VM (12.1% with migraine without aura vs. 7.5% with migraine with aura vs. 14.1% with chronic migraine) and probable migraine in probable VM (0.6% with migraine without aura vs. 1.5% with chronic migraine vs. 11.9% with probable migraine). The relative frequencies of VM and probable VM according to migraine subtypes are shown in Figure 2 (p < 0.001).
Relative frequencies of VM according to the subtypes of migraine. The frequencies of VM and probable VM according to the four subtypes of migraine were significantly different (p < 0.001). VM: vestibular migraine; migraine wo aura: migraine without aura; migraine w aura: migraine with aura.
Clinical characteristics of VM based on the ICHD-3β
The mean age of the 65 patients with VM was 40.3 years, and 79.7% of this group was female. The distribution of the accompanying migraine diagnoses according to the ICHD-3β was migraine without aura (43, 66.2%), chronic migraine (19, 29.2%), and migraine with aura (three, 4.6%). The most common symptoms that qualified for a diagnosis of VM were head motion-induced dizziness with nausea (24, 36.9%), spontaneous vertigo (17, 26.2%), positional vertigo (14, 21.5%), and head motion-induced vertigo occurring during head motion (10, 15.4%). No patient presented with visually induced vertigo as a vestibular symptom accompanying the VM. The median duration of vestibular episodes was 180 minutes (range, 60–630 minutes, interquartile, 25%–75%), and the VM durations were 5–60 minutes (25, 38.5%), 1–24 hours (36, 55.4%), and 24–72 hours (four, 6.2%).
Comparison of clinical characteristics between patients with VM and patients with probable VM or non-VM
Comparison of clinical characteristics of patients with VM and patients with probable VM.

p < 0.05, statistically significant relationship between VM and probable VM. Results expressed as median and interquartile 25%–75%. Numerical variables were compared using the Mann-Whitney test, and categorical variables were compared using chi-square tests. VM: vestibular migraine; MOH: medication-overuse headache; ICHD-3β: International Classification of Headache Disorders, third beta edition; VAS: visual analog scale; n: number of patients.
Inter-rater reliability for the diagnosis of VM
Fleiss’ kappa value for the VM diagnosis was 0.97. Fleiss’ kappa value for all VM diagnoses (VM or probable VM vs. others) was 0.90. The kappa values in this study suggested excellent inter-rater agreement.
Discussion
This prospective, first-visit, outpatient-based, multicenter study in Korea found the following: 1) the prevalence of VM was 10.3% in migraineurs, and 2.5% of these patients suffered from probable VM. The prevalence of definite or probable VM was 5.7% among patients with headache who visited the neurology clinic for the first time. 2) The prevalence of VM according to the four migraine subtypes could be compared because of the large number of migraineurs (n = 631). The most common group was chronic migraine in VM and probable migraine in probable VM. 3) No differences regarding clinical characteristics were found between patients with migraine with VM/probable VM and those with non-VM migraine.
This study had several strengths. We applied the appendix criteria for VM during clinical practice at the neurology outpatient clinics in several hospitals at the same time, and the VM kappa value was excellent for clinical purposes. The prevalence of VM is presented with the prevalence of other migraine subtypes and other primary headache disorder subtypes. VM was a relatively common diagnosis among the 1231 patients with a primary headache disorder; VM was more common than migraine with aura, and VM was between the eighth and ninth most common subtypes of the 25 subtypes of primary headache disorder based on the second-digit diagnosis.
The prevalence of VM
The prevalence of VM in previous studies was dependent on different diagnostic criteria and study populations. Prior to the current diagnostic criteria, the prevalence of VM was 9%–11.9% in headache clinics, 4.7%–29.3% in otolaryngology clinics, and 6%–25.1% in specialized dizziness clinics (4,11,14,19,20,23). Only one study assessed the prevalence of VM based on the consensus criteria formulated by the Barany Society and the IHS; 4.2% were assigned to the definite VM group and 5.7% to the probable VM group in a tertiary referral otolaryngology clinic (12). In a population-based survey, the lifetime prevalence of VM was nearly 1%, with a one-year prevalence of 0.89% (3). Another community-based study reported that the one-year prevalence of VM was 5% in women aged 40–54 years (24). We enrolled patients with headache who visited a multicenter outpatient neurology department for the first time using ICHD-3β criteria and found that the prevalence of VM was higher than that in patients from otolaryngology clinics; therefore, VM might be a common and significant diagnostic entity in neurology clinics.
VM has been increasingly recognized as a frequent cause of recurrent episodic vertigo, but it has been underdiagnosed in clinical settings owing to the absence of generally accepted diagnostic criteria. According to the ICHD-3β, VM requires that more frequent episodes (at least five) must fulfill the duration criterion (5 minutes–72 hours) and have greater severity (moderate to severe) compared with the criteria proposed previously by Neuhauser et al. (14). Additionally, the ICHD-3β criteria include the criteria only for VM and exclude those for probable VM. The consensus criteria issued by the Barany Society and the IHS include both definite and probable VM. Previous VM studies reported significant benefits of prophylactic treatment regardless of VM subtype, and half of patients with probable VM met the criteria for definite VM as the disease progressed (10,12,25,26). Therefore, we included probable VM, and the prevalence of VM was 12.8% in this study when it was broadly defined to include the probable subtypes.
Subtypes of migraine and VM
In this study, the prevalence of VM in patients with chronic migraine was 14.1%, which was higher than that of migraine with aura (7.5%), and the statistical difference may be due to this result. The association between VM and migraine with aura is still debated, as some studies have found a connection (3,27), whereas others have found that patients with migraine without aura had VM more often (20,28).The prevalence of VM in patients with chronic and probable migraine was not assessed before application of the ICHD-3β. Previous studies reported a mean 8- or 19-year difference between the onset of migraine and the onset of vestibular episodes of VM (26,27). Although further investigation is needed, the prevalence of relatively long-duration chronic migraine compared with that of episodic migraine may explain the higher proportion of patients with VM. In addition, the ICHD-3β does not have criteria for probable VM, and therefore vestibular symptoms in patients with probable migraine were classified only as probable VM using the consensus diagnostic criteria of the Barany Society and the IHS.
The proportion of patients with probable VM in our study was lower than that reported previously. Our study included only patients with migraine, whereas previous studies used less-strict criteria or included patients with non-migraine headache and patients with additional vestibular disorder diagnoses (12,16). We identified patients as probable VM if they met the criteria for vestibular episodes of VM and they met all but one criterion for migraine. The deficient IHS criteria classified as probable migraine were number of headache attacks (50%), duration of attacks (25%), presence of accompanying symptoms (16.7%) and headache characteristics (8.3%) in probable VM patients. Some patients are headache free for years before VM manifests (25,26). The headache is attenuated when the migraine is accompanied by vertigo compared with the usual migraine attack (9). Using the probable VM diagnosis will increase recognition and proper treatment of VM disease entities; thus, it should be considered for inclusion in the next version of the ICHD-3β (19).
Vestibular symptoms in VM
The most frequent vestibular symptoms in a large population-based survey were spontaneous rotatory vertigo, followed by positional vertigo in patients with VM (67% vs. 24%) (3). In our study, participants chose one main symptom among the five vestibular symptoms that qualified them for a VM diagnosis based on the ICHD-3β; the most common vestibular symptom in patients with VM was head motion-induced dizziness with nausea, and the most common symptom in patients with probable VM was spontaneous vertigo. Our data are consistent with the wide variability in the duration of vestibular episodes. The duration of attacks can vary from a few seconds (10% of patients) to several minutes (30% of patients), several hours (30% of patients), and even up to a few days (30% of patients); however, vestibular episodes < 5 minutes are not included as VM in the ICHD-3β (22). According to our data, 55.4% of patients with VM experienced episodes lasting 1–24 hours, whereas 62.5% of patients with probable VM experienced episodes of 5–60 minutes. The neural mechanisms of VM remain unclear, and the variability in the symptoms and clinical findings during and between attacks suggests that migraine interacts with the vestibular system at various levels (20,26,27).
This study had several limitations. First, it was cross-sectional in design with no long-term longitudinal follow-up data. VM is a heterogeneous and evolved condition that has a temporal relationship with vestibular symptoms and headache. Therefore, use of a headache diary should be considered in longitudinal studies. Second, our data did not assess information about the impact of VM. A prospective longitudinal VM study including information regarding impact or disability may be warranted. Third, our study was conducted in nine hospitals, and the VM frequency varied among hospitals. When we excluded the investigator who reported the lowest VM prevalence in the inter-rater reliability assessment, the Fleiss’ kappa value was the same (0.97). Although the diagnostic reliability of the investigators did not differ, the selection bias could have affected the results because the clinical settings were different. Therefore, this difference should be considered in future multicenter studies.
In conclusion, we described the prevalence and clinical characteristics of new diagnostic criteria for VM based on the ICHD-3β, which can be widely used in outpatient clinical settings. VM is relatively common among first-visit patients with migraine and should be included in the standard ICHD criteria. Additionally, including probable migraine in the accompanying migraine diagnosis of VM or considering incorporating it into a broader diagnostic category, such as probable VM, should be discussed when planning the next version of the ICHD-3β.
Clinical implications
We applied the newly developed criteria for vestibular migraine (VM) based on the appendix criteria of the third beta edition of the International Classification of Headache Disorders (ICHD-3β) in a prospective, multicenter headache registry study. VM was diagnosed in 10.3% of first-visit migraineurs in neurology clinics. VM was relatively common among first-visit patients with migraine and should be considered a subtype of migraine in the standard ICHD criteria. Comparisons of the frequencies of VM according to migraine subtype revealed that the most common were chronic migraine in VM and probable migraine in probable VM. Therefore, probable migraine should be included as an accompanying migraine VM diagnosis or broader diagnostic category should be developed, such as probable VM in the next ICHD version.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported in part by a grant from the Korean Headache Society.