
Abstract
Aim
We aimed to conduct a systematic review evaluating the effectiveness of interventions used by physiotherapists on the intensity, frequency and duration of migraine, tension-type (TTH) and cervicogenic headache (CGH).
Methods
We performed a systematic search of electronic databases and a hand search for controlled trials. A risk of bias analysis was conducted using the Cochrane risk of bias tool (RoB). Meta-analyses present the combined mean effects; sensitivity analyses evaluate the influence of methodological quality.
Results
Of 77 eligible trials, 26 were included in the RoB assessment. Twenty trials were included in meta-analyses. Nineteen out of 26 trials had a high RoB in >1 domain. Meta-analyses of all trials indicated a reduction of TTH (p < 0.0001; mean reduction −1.11 on a 0–10 visual analog scale (VAS); 95% CI −1.64 to −0.57) and CGH (p = 0.0002; mean reduction −2.52 on a 0–10 VAS; 95% CI −3.86 to −1.19) pain intensity, CGH frequency (p < 0.00001; mean reduction −1.34 days per month; 95% CI −1.40 to −1.28), and migraine (p = 0.0001; mean reduction −22.39 hours without relief; 95% CI −33.90 to −10.88) and CGH (p < 0.00001; mean reduction −1.68 hours per day; 95% CI −2.09 to −1.26) duration. Excluding high RoB trials increased the effect sizes and reached additional statistical significance for migraine pain intensity (p < 0.00001; mean reduction −1.94 on a 0–10 VAS; 95% CI −2.61 to −1.27) and frequency (p < 0.00001; mean reduction −9.07 days per month; 95% CI −9.52 to −8.62).
Discussion
Results suggest a statistically significant reduction in the intensity, frequency and duration of migraine, TTH and CGH. Pain reduction and reduction in CGH frequency do not reach clinically relevant effect sizes. Small sample sizes, inadequate use of headache classification, and other methodological shortcomings reduce the confidence in these results. Methodologically sound, randomized controlled trials with adequate sample sizes are required to provide information on whether and which physiotherapy approach is effective. According to Grading of Recommendations Assessment, Development and Evaluation (GRADE), the current level of evidence is low.
Introduction
A reported lifetime prevalence of more than 90% indicates the global relevance of headache (1). The most common primary headache types are migraine and tension-type headache (TTH) (1), which are often referred to physiotherapy to support pharmacological treatment (2). A frequently reported secondary headache type seen in physiotherapy clinics is cervicogenic headache (CGH) (3,4).
National and international (5,6) guidelines focus primarily on pharmacological management. Supporting non-pharmacological approaches such as biofeedback, acupuncture, relaxation and physical therapy are also recommended but guidelines criticize the low level of evidence.
Existing systematic reviews evaluating the evidence for physiotherapy interventions are either outdated (7,8) or approach the topic from a pre-defined focus on specific interventions. The most recent publication focused on manual therapy for primary headache (9). It reported an effective reduction of symptoms in all six included trials. The authors stated that no trials on migraine or cluster populations were found, hence results included TTH only. A meta-analysis was not conducted. The same authors also conducted a systematic review on cervicogenic headache with similar results (3). Other reviews indicating the potentially beneficial effect of physiotherapy interventions did not use a systematic approach. Evidence-based conclusions cannot be drawn from these publications (10–12).
Hence, the purpose of this review is to provide an overview of the current evidence on the topic by using a systematic search strategy, evaluating the risk of bias of included trials, systematically extracting data from included trials and combining these in meta-analyses for mean treatment effects to inform clinical practice and guide future research.
Methods
This literature review was conducted and reported following the guidelines published by the Cochrane Handbook and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (13,14).
Eligibility criteria for trial inclusion
Types of studies
All randomized controlled trials (RCTs) comparing a physiotherapy intervention with a control group or an active intervention were considered for inclusion in the review. For cross-over trials only the first phase of the trial prior to crossing to the second intervention was included in meta-analyses. Case studies or uncontrolled trials were excluded. Trials had to be published in the English or German language.
Types of participants
Trial participants were adults with migraine, TTH and CGH. In the attempt to include all relevant trials, publications were also included if participants were described as having “mixed headache” or if populations were not classified but according to the clinical description likely to represent these headache types. Excluded were other primary headache types (e.g. cluster headache, short-lasting unilateral neuralgiform headache with conjunctival injection and tearing (SUNCT)) or secondary headache due to a pathology not located in the cervical spine. Further excluded were headache types of traumatic history such as whiplash-associated disorder because of the heterogeneity of pathologies (15). Trials on children and animal studies were also excluded.
Types of interventions
Trials were eligible for inclusion if the intervention was led by a physiotherapist and was a standard physiotherapy approach such as exercise, manual therapy, soft-tissue techniques, or strength and endurance training. Trials evaluating an intervention applied by a chiropractor, masseur, osteopath, psychologist, alternative healer, yoga teacher or acupuncturists were excluded.
Types of comparisons
Acceptable comparator interventions were any type of placebo intervention or any other active intervention as well as waiting list or standard care.
Types of outcome measures
Based on the results of a scoping search and in order to facilitate the combination of results in meta-analyses, trials were included that evaluated the effect of physiotherapy interventions on at least one of the following outcome measures:
–Intensity of headache measured on a visual analog scale (VAS) or numerical rating scale for pain. –Frequency of headache episodes measured as number of episodes or number of headache days within a defined period of time (e.g. within one month). –Duration of headache episodes measured in hours or days without relief.
Search methods for identification of studies
Information sources
Two researchers independently conducted a systematic search of electronic databases relevant to the medical and allied health professions literature. The cut-off date for the literature search was August 20, 2014. PubMed was used to search Medline, OVID to additionally search EMBASE and PsychINFO. Additional database searches were performed in the Cochrane Register of Controlled Trials (CENTRAL), Cumulative Index to Nursing and Allied Health Literature (CINAHL) and Physiotherapy Evidence Database (PeDRO).
Hand-searching included reference lists of previously identified reviews and of the newly acquired trial publications. The contents of all journals in which included trials were published (BMC Musculoskeletal Disorders; Cephalalgia; Clinical Journal of Sports Medicine; Clinical Rehabilitation; Headache; International Journal of Sports Medicine; Journal of Back and Musculoskeletal Rehabilitation; Journal of Exercise and Rehabilitation; Journal of Manipulative and Physiological Therapeutics; Journal of Orthopedic and Sports Physical Therapy; Journal of Pain and Symptom Management; Journal of Rehabilitation Medicine; NeuroRehabilitation; Pain; PloS One; Pain Medicine; Scandinavian Journal of Work, Environment and Health; Spine) as well as other key journals for physiotherapy (Manual Therapy, Physical Therapy) were searched.
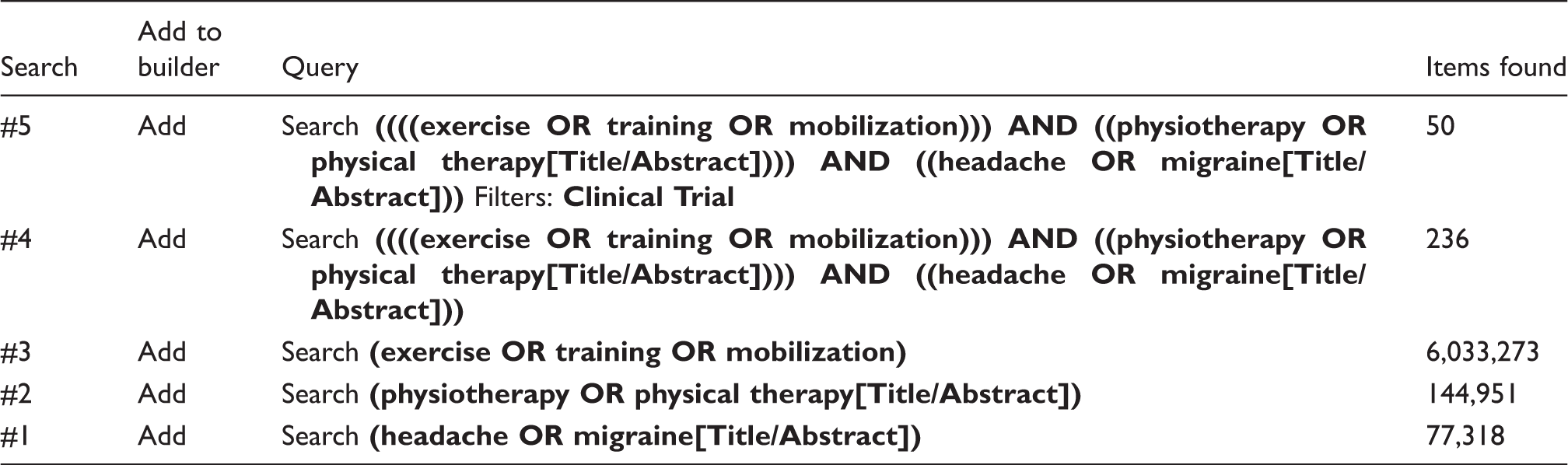
Literature search
Medical subject heading (MeSH) terms and natural language terms were combined in the search strategy. The search strategy included terms referring to the population studied, the intervention this review was focused on, the control intervention and the outcome studied. The following search terms were combined:
Population
adult AND (headache OR migraine)
Intervention
physiotherapy OR physical therapy OR exercises OR training OR manual therapy OR mobilization
Comparison
sham OR placebo OR control
Outcome
pain intensity OR frequency OR duration
Search strategy for PubMed (Medline).
Study selection
Articles identified were selected independently by two reviewers (16) to minimize bias. In the first stage of study selection, the eligibility criteria were applied to the title and abstract of identified articles. In the second stage, the full text publications of potentially eligible articles were obtained and criteria reapplied. Strength of inter-reviewer agreement regarding study eligibility was expressed using Cohen’s kappa coefficient (17). In case of a disagreement between the two reviewers that was not resolved by discussion, a third reviewer was approached who subsequently decided whether the article should be included (16).
Data extraction and management
Data from included trials were collected and entered into a table with pre-specified headings (16) designed to meet the research objectives. The data extraction table contained the following data items:
Author, date and country of the trial study population; Type of headache investigated and diagnostic criteria; Type, duration, frequency of intervention(s) including numbers of participants in intervention group; Type of control intervention(s) and numbers of participants in control group; Outcome measure(s); Time point(s) of measurement(s).
Assessment of risk of bias in included studies
Included trials were critically appraised for potential risk of bias by two independent researchers using the Cochrane risk of bias (RoB) assessment tool (18). Strength of inter-rater agreement was expressed using Cohen’s kappa coefficient (17). If blinding of the patient or therapist was impossible for technical reasons, it was rated as “not applicable.” The domain “incomplete outcome data” was considered to induce a risk of bias if data were statistically analyzed per-protocol and losses to follow-up were 20% or higher (19).
Synthesis of results
All trials were included in the descriptive analysis. Meta-analyses were conducted for the outcome measures pain intensity, frequency and duration for each headache type individually using a random-effects model allowing for population and intervention parameters to vary between trials (20). For comparability reasons, only trials that compared physiotherapy interventions with a control group or usual care were entered into the meta-analyses. For these trials mean values and standard deviations (SDs) post-intervention were entered into the meta-analyses. If these were not reported, mean values were calculated from change over time, and SDs from confidence intervals (CIs) or standard errors. Trials that compared two active interventions were reported descriptively.
Including trials with high risk of bias domains in meta-analyses can lead to invalid conclusions (18). To explore the influence of methodological quality on meta-analysis results, sensitivity analyses were conducted that excluded trials with a high risk of bias rating in a minimum of one domain.
In order to define the most effective type of physiotherapy intervention for each headache type, sub-analyses were conducted for each headache type, each outcome and each type of physiotherapy intervention. Interventions were grouped into strength training, manual therapy (plus exercises), trigger point treatment, combined physical and psychological interventions (e.g. exercises combined with relaxation) and aerobic exercises.
The software used for the meta-analyses was Review Manager, version 5.0, Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2008.
Overall level of evidence
The overall level of evidence was evaluated using Grading of Recommendations Assessment, Development and Evaluation (GRADE) (21). The GRADE approach is used to formulate an overall conclusion on the level of evidence based on the methodological quality of included trials (21). Evidence based on RCTs with a low risk of bias is regarded as high while evidence from observational studies is regarded as low (22). Following specific criteria (e.g. imprecision of results indicated by wide CIs), the level of evidence from RCTs can be downgraded by one or two levels. Accordingly, the level of evidence from observational studies can be upgraded when specific criteria are fulfilled (22).
Results
Study selection
A total of 77 studies were identified during the electronic and hand-search processes. After title/abstract screening, 50 studies were retrieved as full text articles (Figure 1). Full text screening excluded 23 studies that did not include a control group (12,23–31), did not use headache-related outcome measures (32–36), did not conduct a physiotherapy intervention (37–44) and one study (45) because it seemed to investigate the same study population as Mongini et al. (46), resulting in a total number of 26 included trials. Five of these could not be included in the meta-analyses since they compared two active interventions (35,47–50). One could not be included since results were reported as median and interquartile range and could not be converted (51). The inter-rater agreement of studies to be included in the systematic review during title/abstract and full text screening was very high, with kappa 0.83 (95% CI 0.67 to 0.99).
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram for trial inclusion.
Risk of bias
Risk of bias evaluation.

1: Sequence generation; 2: allocation concealment; 3: participant blinding; 4: therapist blinding; 5: assessor blinding; 6: incomplete outcome data; 7: selective reporting; 8: other risks of bias; +: low risk of bias, –: high risk of bias;?: unclear risk of bias; MT: manual therapy; NA: not applicable; SNAG: sustained natural apophyseal glides; US: United States.
Data extraction
Trial characteristics.

CGH: cervicogenic headaches; CMD: craniomandibular dysfunction; IHS: International Headache Society; TTH: tension-type headache; SNAG: Sustained natural apophyseal glides; PT: physical therapy; CD: compact disc; IASP: International Association for the Study of Pain; US: United States.
All trials focusing on migraine patients used aerobic exercise or multidisciplinary treatment as an intervention apart from one trial that included a relaxation group as well as an aerobic exercise group (52). Treatment approaches for TTH were more heterogeneous and included muscle techniques such as trigger point treatment (55), physical training (35), mobilization (63) and mixed physiotherapy approaches (47,48,53,69).
Interventions for CGH were primarily mobilization of the cervical spine (50,64,65,68) or a different technique plus mobilization of the cervical spine (49) but also included trigger point therapy (62), exercises (65), and physical training (61) (Table 3).
Synthesis of the results
Meta-analyses results for each headache type are shown in Figures 2–4. The results of sensitivity analyses evaluating the effect of methodological quality on the combined mean effects are detailed in Table 4. Sub-analyses for the different types of physiotherapy interventions are shown in Table 5.
(a)–(c) Meta-analyses showing the reduction in TTH intensity (top), duration (middle) and frequency (bottom). (a)–(c) Meta-analyses showing the reduction in migraine intensity (top), duration (middle) and frequency (bottom). (a)–(c) Meta-analyses showing the reduction in CGH intensity (top), duration (middle) and frequency (bottom). Meta-analyses results with and without inclusion of high risk of bias trials. CGH: cervicogenic headaches; CI: confidence interval; TTH: tension-type headache; VAS: visual analog scale. Hours without relief. P values in bold indicate statistically significant effects (p < 0.05). Meta-analyses results for individual physiotherapy interventions for each headache type. CGH: cervicogenic headaches; CI: confidence interval; TTH: tension-type headache; VAS: visual analog scale. P values in bold indicate statistically significant effects (p < 0.05).


TTH
Three trials (234 participants) were included in the meta-analyses (Figure 2 (a)–(c)) that evaluated the effect of a physiotherapy intervention compared to a control group of usual care (53,55,57). All of these trials had at least one high risk of bias rating; hence sensitivity analyses to evaluate the effect of methodological quality on outcome were not conducted. Combined results indicated statistically significant results for pain reduction only. The analyses of different types of physiotherapy interventions indicated a small but significant effect of trigger point therapy on the intensity of TTH (one trial) and of manual therapy (plus exercises) for the reduction of the frequency and duration of TTH (Table 5).
Four trials compared two active interventions (35,47,48,63): Carlsson et al. (1990) compared acupuncture and physiotherapy interventions (relaxation, exercises, education, tape) and reported significantly more pain reduction in the physiotherapy group after 10–12 sessions (reduction of −1.21 (SD 0.9) on a one-to-five scale versus a reduction of −0.54 (SD 1.01) in the acupuncture group (p < 0.05)) (47). Two manual therapy techniques were applied in the study by Demirturk et al. (2002). Results indicated no statistically significant difference regarding pain intensity between the groups after connective tissue mobilization or Cyriax vertebral mobilization (63). Söderberg et al. compared three interventions: acupuncture, physical training and relaxation training. The only significant between-group difference after the final of 10–12 treatments was significantly more headache-free days (p < 0.01) and headache-free periods (p < 0.05) in the relaxation group compared to the acupuncture group. Pain intensity and duration were reduced in all groups but not significantly different across groups (35). Van Ettekoven and Lucas (2006) evaluated additional craniocervical exercises to a physiotherapy intervention and found that frequency, duration and intensity were not significantly different between groups immediately after the six-week intervention but all three outcome measures differed significantly at six-month follow-up (48). Data from the trial by Torelli et al. (70) were not entered into the meta-analyses because of the reporting of results and the trial design. Physiotherapy interventions compared with an observation period in this crossover-trial was reported to reduce frequency of headache episodes but did not change the severity of the headache or the duration of the episodes after an eight-week intervention period.
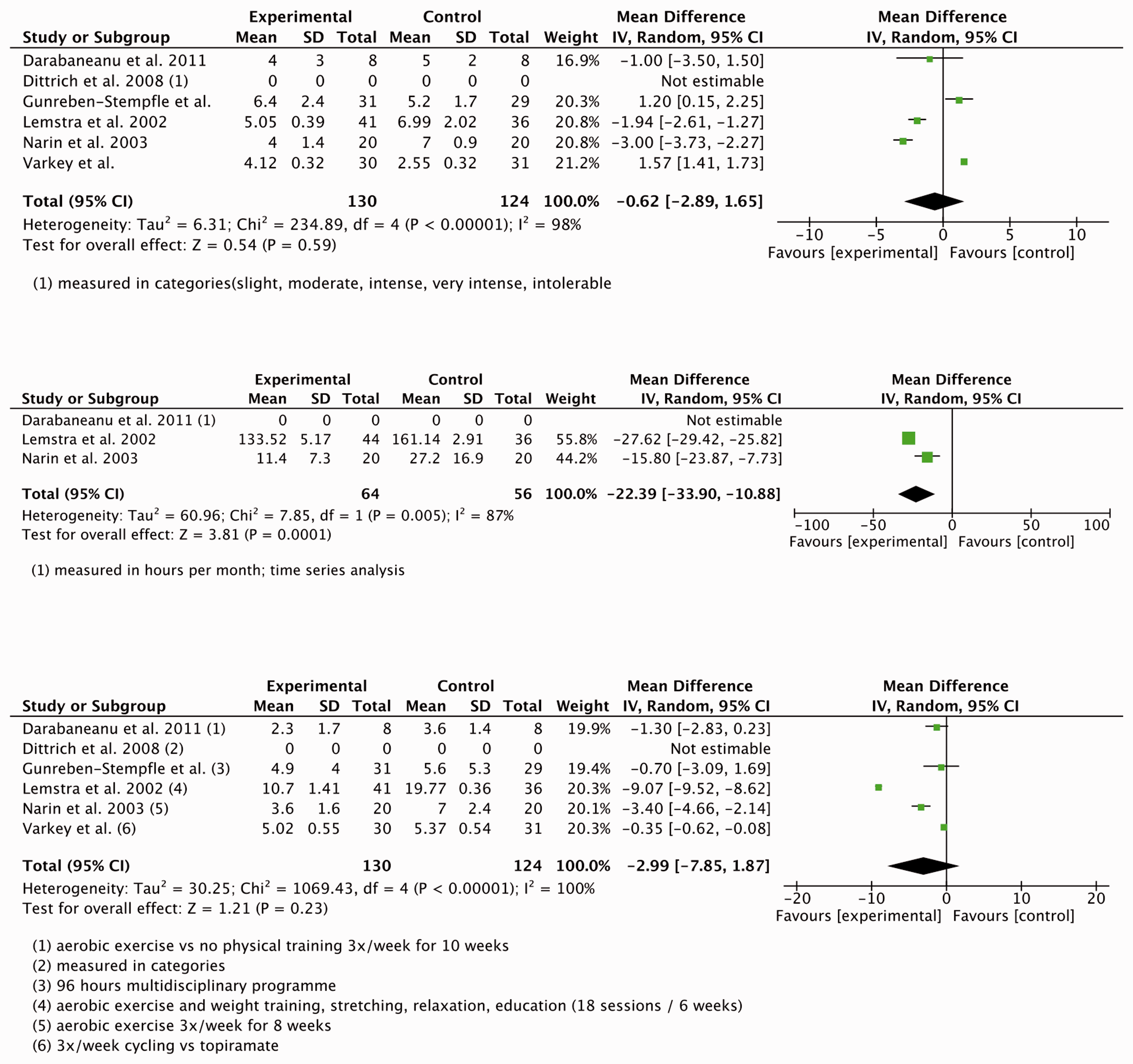
Migraine
Five trials (316 participants) were included in the meta-analyses (52,56–58,66) (Figure 3 (a)–(c)). Combined results for pain intensity, frequency and duration were statistically significant in the two trials with a low risk of bias. Including three additional trials with high risk of bias ratings did not result in statistically significant changes (Table 4).
Sub-analyses for the different types of physiotherapy interventions indicated that aerobic exercises or the combination of physical and psychological interventions (such as relaxation) resulted in a reduction of the duration of migraine attacks (Table 5).
However, Darabaneanu et al. reported no significant difference between a group that had received aerobic training and a control group (58). This trial could not be entered into the meta-analysis since the authors had conducted a time series analysis and measured duration in hours per month.
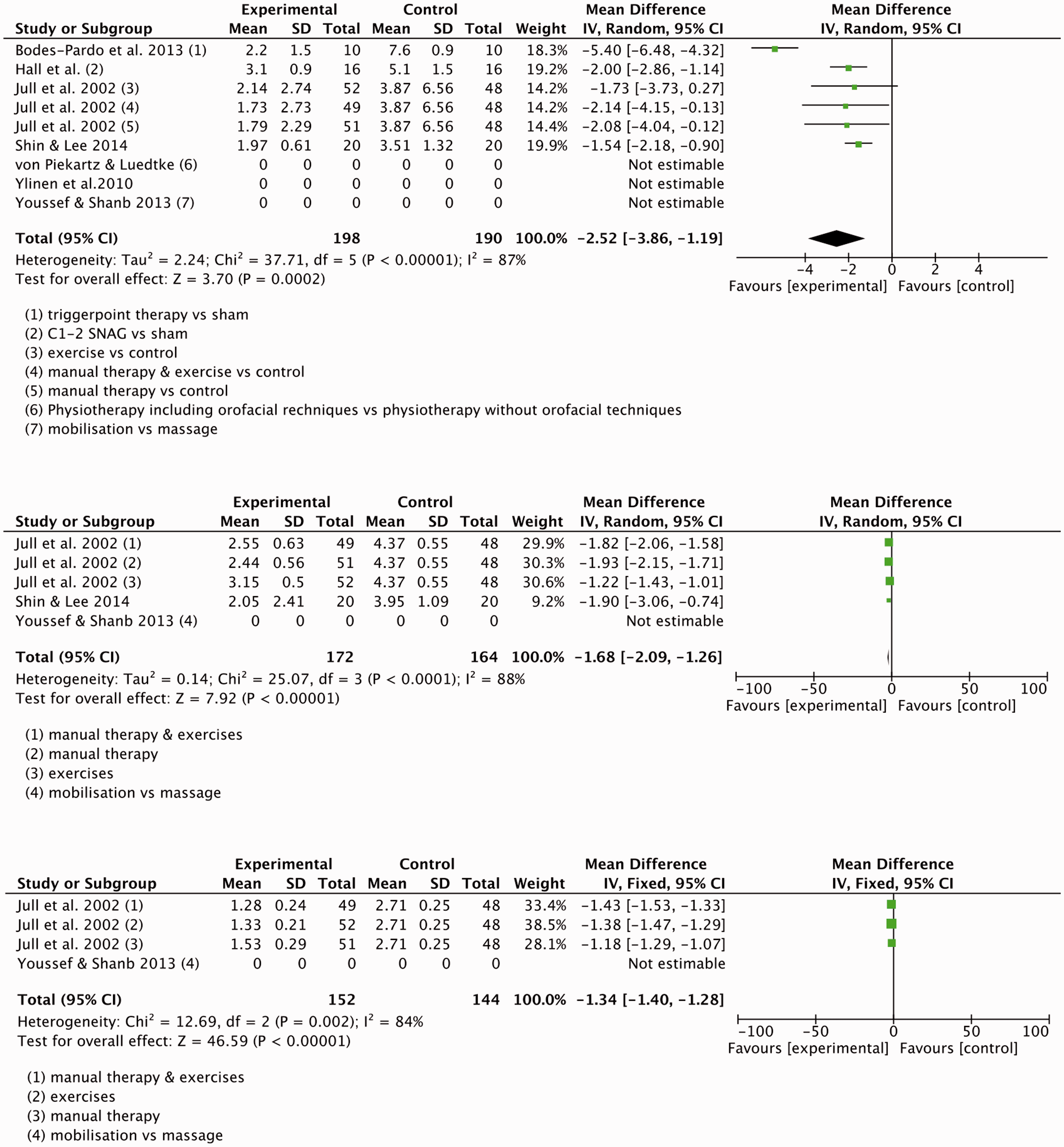
CGH
Four trials (388 participants) that evaluated the effectiveness of interventions used by physiotherapists compared to a control group or usual care were combined in meta-analyses (62,64,65,68) (Figure 4 (a)–(c)). The combined mean effect for pain reduction, reduced frequency and duration were statistically significant with and without inclusion of high risk of bias trials (Table 4).
Sub-analyses for the different types of physiotherapy interventions indicated that manual therapy resulted in a reduction in intensity, frequency and duration of CGH. Trigger point therapy reduced the intensity of CGH (Table 5).
Youssef and Shanb compared mobilization and massage as an intervention to reduce the duration of CGH. Mobilization resulted in a significantly larger reduction of headache duration in this trial (p = 0.008) (50).
Mixed headache populations
Four trials evaluated change in headache intensity after a physiotherapy intervention compared to a control group or standard care (59,60,61,69). The combined mean results were statistically significant for the reduction of frequency and duration but not for pain intensity (Table 4). Two large trials (2225 participants), investigating a workplace intervention for the reduction of headache and neck pain, dominated the combined results for trials evaluating frequency of headache in mixed or undefined headache populations (46,65). Retrospective analyses indicated that two-thirds of the participants suffered from TTH and one-third from migraine, but results were not distinguished by headache types.
Discussion
Since the publication of the Cochrane review by Bronfort et al. (2004) on non-invasive physical treatments for chronic/recurrent headache (7), the number of research reports has increased significantly. Published trials were less heterogeneous than in 2004 and allowed for a combination of results in meta-analyses. Combined mean effects confirmed the general conclusions by Bronfort et al. that non-invasive physical treatments seem to play a role in the prevention of headache attacks and reduction of headache symptoms.
Results from this current review further suggest that physiotherapy interventions may have a positive effect on all types of headache included in this review. None of the meta-analyses indicated a negative effect for physiotherapy interventions on any type of headache or any outcome measure; however, some of the combined mean effects were very small and possibly not clinically relevant. For example, the statistically significant reduction of the pain intensity in TTH was only −1.11 on a 0–10 VAS. We could not identify any publications that defined clinical meaningfulness in headache populations, whereas in other chronic pain populations, pain reduction was perceived as worthwhile if it reached at least 30% or 2.4 points on a 0–10 numerical scale (73,74). Clinically meaningful change has to be viewed in relation to the time, effort and costs of the chosen treatment approach, hence an effect of −0.80 on a 0–10 VAS (95% CI from −1.49 to −0.11) after a 96-hour multidisciplinary program compared to standard care seems too small to justify the resources (57). On the other hand, a reduction of 3.4 migraine days per month (95% CI from −4.66 to −2.14) may justify the effort of a three-times weekly aerobic and strength training program considering the low costs of physical training in relation to the potential side effects of pain medication. Furthermore, pain intensity, frequency and duration of attacks are only three of a variety of possible outcome measures and might not be sensitive enough to reflect patient perceptions of well-being. Other outcome measures such as quality of life (75), disability (75) or global perceived improvement (76) might provide more detailed information about treatment effects.
A limitation of this review is that trials in languages other than German and English were not considered. Furthermore, this review can provide only a trend toward the most effective physiotherapy approach for specific headache types because of the heterogeneity of techniques and methods used in the included trials. Not all types of physiotherapy interventions have been applied to all types of headache, and for some physiotherapy interventions results are based on a single publication. Sub-analyses for the different physiotherapy interventions showed that aerobic exercise and a combination of physical and psychological interventions was effective for the reduction of migraine attack duration; however, no trials were available that used either manual therapy, trigger point therapy, or strength training. Manual therapy showed a highly significant effect for the reduction of TTH frequency and duration, but these results were based on one trial, only. CGH had been treated only with manual therapy and trigger point therapy. Both techniques showed highly significant results. However, no evidence for the effect of aerobic exercises, strength training and combined physical and psychological interventions was available.
The choice of interventions for the treatment of migraine and TTH used in included trials seemed to be based on theoretical knowledge and beliefs rather than on the patient’s individual signs and symptoms identified by the treating therapist. These standardized treatment approaches do not reflect the clinical reasoning-guided physiotherapy practice that is postulated by the World Confederation for Physical Therapy (72). There is a clear need for more and better research to identify the role of, for example, the cervical spine, muscle tension, postural changes, stabilizing muscles and other physical aspects in different headache types, especially in migraine and TTH, and subsequently to develop treatment strategies that effectively target such clinical findings.
A further difficulty is the classification of headache types within trials. Most authors state that the International Headache Society (IHS) classification was used, but did not report who diagnosed patients and whether patients were excluded who did not fulfill all of the required IHS criteria. There is substantial overlap across headache types in the different classifications; for example, CGH is described as mostly but not always located unilaterally (71,77,78) and one study reported that 6% of TTH is associated with nausea (79) and therefore probably misdiagnosed as migraine. Moreover, patients might suffer from more than one type of headache (80). Especially the diagnosis CGH is difficult to prove since laboratory and imaging evidence, as suggested by the IHS classification, were not available in most trials. Interestingly, the efficacy of physiotherapy interventions in trials that defined their study sample as CGH was particularly high. The diagnostic title CGH implies a treatable pathology in the cervical spine. The exact source of the symptoms is unknown and could involve cervical muscles or cervical joints connected via afferents to the trigeminal nuclei (78).
In conclusion, physiotherapy is low cost, has nearly no side effects and seems beneficial for the reduction of most headache symptoms. It should, therefore, be considered to support the medical management of headache and migraine. Considering the time and effort that is required for some approaches, and the fact that efficacy is reached only after longer training periods (e.g. aerobic and strength training), patient preference for specific treatment approaches can play a role in the choice of the most appropriate physical treatment.
Using GRADE (22), the overall quality of published trials remains low. This can be interpreted as “future research is likely to change the results of this review.” Further RCTs of high methodological quality and including appropriate numbers of participants are required to evaluate the role of physiotherapy interventions in headache and migraine treatment. This is clinically and scientifically relevant, given that irrespective of evidence, most national and international treatment guidelines recommend and most patients currently receive some sort of physiotherapy as a treatment for headache.
Clinical implications
Physiotherapy interventions resulted in a statistically significant effect on the intensity of tension-type headache (TTH) and cervicogenic headache (CGH), the frequency of CGH, and the duration of migraine and CGH when combined in meta-analyses. Removing trials with high risk of bias domains resulted in an additional significant effect on migraine intensity and frequency. Statistically significant effects were identified for manual therapy for the reduction of TTH frequency and duration and for all outcomes in CGH, trigger point treatment for the reduction of the intensity of TTH and CGH, combined physical and psychological interventions as well as aerobic exercises for the reduction of the duration of migraine. The level of evidence for this effect based on methodological quality and external validity factors is low. Randomized controlled trials of high methodological rigor with adequate sample sizes are required to confirm the results of the meta-analyses.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the 7th Framework EU-project EuroHeadPain (#602633) to A.M. and an unrestricted scientific grant from the German Headache Society (DMKG) to K.L.