
Abstract
Background
Evidence on the association between headache and physical fitness is conflicting. The aim of this population-based study was to examine the relationship between peak oxygen uptake (VO2peak) and headache, including migraine and tension-type headache (TTH).
Methods
In the third Nord-Trøndelag Health study (HUNT3), VO2peak was measured by ergospirometry in a sample of 4631 healthy adult participants. Of these, 3899 (54% women) also answered headache questions. The cross-sectional association between headache and VO2peak was evaluated by logistic regression using a categorical approach based on quintiles. Scores in the upper quintile were used as reference.
Results
Participants age 20–50 years had significant trends of increasing prevalence of any headache (p < 0.001), migraine (p < 0.001), TTH (p = 0.002) and unclassified headache (p = 0.027) with lower VO2peak. The highest prevalence odds ratios (ORs) were found in those with VO2peak in the lower quintile: For any headache the OR was 2.3 (95% confidence interval (1.6–3.3), for TTH 1.8 (1.2–2.8), for unclassified headache 1.9 (1.1–3.8), and for migraine 3.7 (2.1–6.6). Similar results were also found among those who reported physical activity levels in accordance with current recommendations of the American College of Sports Medicine but nevertheless had low VO2peak. Being in the lowest VO2peak quintile was also strongly associated with migraine aggravated by physical activity (OR 4.1, 2.1–8.1). No significant association was found between VO2peak and headache for those 50 years or older.
Conclusions
In this large cross-sectional study, an inverse relationship was found between VO2peak and headache for adults younger than 50 years of age.
Introduction
In general, physical activity and physical fitness are inversely related to lifestyle-related diseases and mortality (1–4). However, the evidence regarding their effects on headache is limited and ambiguous (5). Although exercise is often recommended for patients with headache, many avoid exercise because it provokes attacks. On the other hand, physical inactivity has a well-known negative influence on health (6), and is a risk factor for headache (7).
The effect of physical exercise on migraine has been evaluated in some clinical studies (e.g. Santiago et al. (8), Totzeck et al. (9), Overath et al. (10) and Varkey et al. (11,12)), but to our knowledge no large-scale population-based study has evaluated the relationship between headache and physical fitness. To inform future guidelines regarding the role of physical activity, it is important to evaluate the relationship between headache and physical fitness measured directly as peak oxygen uptake (VO2peak).
The aim of the present population-based study was to examine the association between VO2peak and headache, especially migraine and tension-type headache (TTH), making use of comprehensive information allowing adjustment for possible confounding factors.
Methods
Study population
The third Nord-Trøndelag Health study (HUNT3) was performed between October 2006 and June 2008. All inhabitants of Nord-Trøndelag County 20 years and older were invited to participate. Details of this comprehensive health study are described elsewhere (13). A sample of self-reported healthy participants who passed a brief medical interview excluding those with cancer, obstructive lung disease, or cardiovascular disease, or on current blood pressure medication, were enrolled in the HUNT3 Fitness Study, which included measurement of VO2peak (14). Of 94,194 invited adults, 50,795 (54%) answered the first questionnaire (Q1) and participated in a brief medical assessment, and 39,690 (42%) of these answered the second questionnaire (Q2), which included headache questions. Details of non-respondents have been described previously (15). Among participants who answered Q1, 5633 volunteered to participate in the HUNT3 Fitness Study, and a total of 4631 participants completed a treadmill test measuring VO2peak, of whom 3899 also completed the headache questions (Figure 1).
Flowchart of participants in this study.
VO2peak
An individualized protocol was applied to measure VO2peak (2,14). Briefly, initial workload was individual and the speed was derived from warm-up (14). When the participants reached an oxygen uptake that was stable during 30 seconds, inclination or velocity on the treadmill was increased until exhaustion (14). A maximal test was considered when the oxygen uptake did not increase >2 ml·kg–1
Headache diagnosis
The HUNT3 Q2 questionnaire included 14 questions regarding headache designed to determine whether the person suffered from headache, and fulfilled the International Classification of Headache Disorders, second edition (ICHD-II) criteria for migraine and TTH (16). The diagnoses were mutually exclusive. A category of unclassified headache emerged as an exclusion diagnosis defined by a positive answer on the headache screening question, but without the necessary characteristics of migraine or TTH. The composite group of “any headache” consisted of participants with migraine, TTH, or unclassified headache. Participants with migraine were also subdivided according to their responses to the question about aggravation by physical activity. The validity of these questionnaire-based diagnoses and the prevalence of the various headache disorders have been reported previously (17,18): For any headache, the sensitivity was 88% and specificity 86% (kappa value 0.70, 95% confidence interval (CI) 0.61–0.79); for migraine, the sensitivity was 51% and specificity 95% (kappa values 0.50, 95% CI 0.32–0.68); and for TTH ≥1 days/month the sensitivity was 96% and specificity was 0.69% (kappa value 0.44, 95% CI 0.30–0.58).
Potential confounders and effect modifiers
Among a wide range of health-related information included in HUNT3 (13), we have previously identified several important factors associated with headache (19) and VO2peak (14). In accordance with a preplanned strategy, the following variables were included as potential confounders or effect modifiers: age (five-year categories); gender, work status (three categories; a) full-time workers, b) part-time workers or c) unemployed, students, or household worker); body mass index (BMI) (continuous variable); smoking status (three categories; current daily smoking, previously daily smoking and never daily smoking); alcohol consumption (five categories); anxiety and depression measured by total Hospital Anxiety and Depression Scale (HADS) (continuous variable); and systolic blood pressure (continuous variable).
On the basis of three questions regarding physical activity, the population was divided into two groups depending on whether they reported a physical activity level that was in accordance with the current recommendations of the American College of Sports Medicine (ACSM) (20). Exercise in accordance with the recommendation was defined as: (1) exercise at high intensity for at least 30 minutes for at least two or three times per week or (2) exercise of medium intensity for at least 30 minutes almost every day. More details about the relationship between physical activity variables and VO2peak in the HUNT study are described elsewhere (21,22).
Ethics
This study was approved by the Regional Committee for Ethics in Medical Research, and the HUNT Study was also approved by the Norwegian Data Inspectorate.
Statistics
In the multivariate logistic regression analyses, we estimated the prevalence odds ratio (OR) with 95% CI for the association between type of headache and VO2peak using a categorical approach based on quintiles. Scores within the upper quintile were used as reference. We initially adjusted for age and gender, and subsequently for potential confounding factors identified previously, such as anxiety and depression, socioeconomic status evaluated by work status, smoking, and alcohol use (19). Potential confounding factors were included in the multiple logistic regression analyses separately or together, but were excluded from the final analyses if the OR changed less than 0.05. Potential interaction between two variables was evaluated by including the product of the variables in the logistic regression analyses, and the interaction coefficient was tested using Wald χ2 statistics. Total HADS score, BMI and smoking status stood out as important confounders, and therefore, all final analyses were adjusted for these factors in addition to age and gender. Participants with incomplete data for one or several variables were included (as a separate missing category) in all analyses to reduce the impact of response bias. In supplementary analyses, we evaluated the OR of different categories of VO2peak in the subgroup of participants who reported aggravation of headache by physical activity, and in those who reported physical activity as recommended by ACSM.
In order to evaluate the probability of a linear relationship between VO2peak and prevalence of headache subtypes (dose-response relationship), we included VO2peak as a continuous variable in a two-sided test of trend. Data analyses were performed with the Statistical Package for the Social Sciences, version 22.0 (SPSS, Chicago, IL, USA).
Results
Characteristics of the study population compared to the total HUNT3 population and HUNT3 participants without known cardiovascular disease, lung disease or cancer.

According to inclusion and exclusion criteria.
Reported physical activity level in accordance with the recommendations of the American College of Sports Medicine (18).
HADS: Hospital Anxiety and Depression Scale; VO2peak: peak oxygen uptake. HUNT3: third Nord-Trøndelag Health study. d, e, f, significantly different from the study population (p < 0.05, ≤0.01, ≤0.001).
For participants aged 20–50 years, lower mean VO2peak was found in those with migraine and TTH than in those who were headache free, whereas there was no difference in those older than 50 years (Figure 2). There was a significant interaction between age and VO2peak regarding OR for headache (p < 0.001), hence multivariate analyses were performed after stratifying for age.
Mean peak oxygen uptake with 95% CI related to headache status below and above 50 years of age.
TTH: tension-type headache; CI: confidence interval.
Odds ratio (OR) of headache related to quintiles of peak oxygen uptake (below 50 years of age).
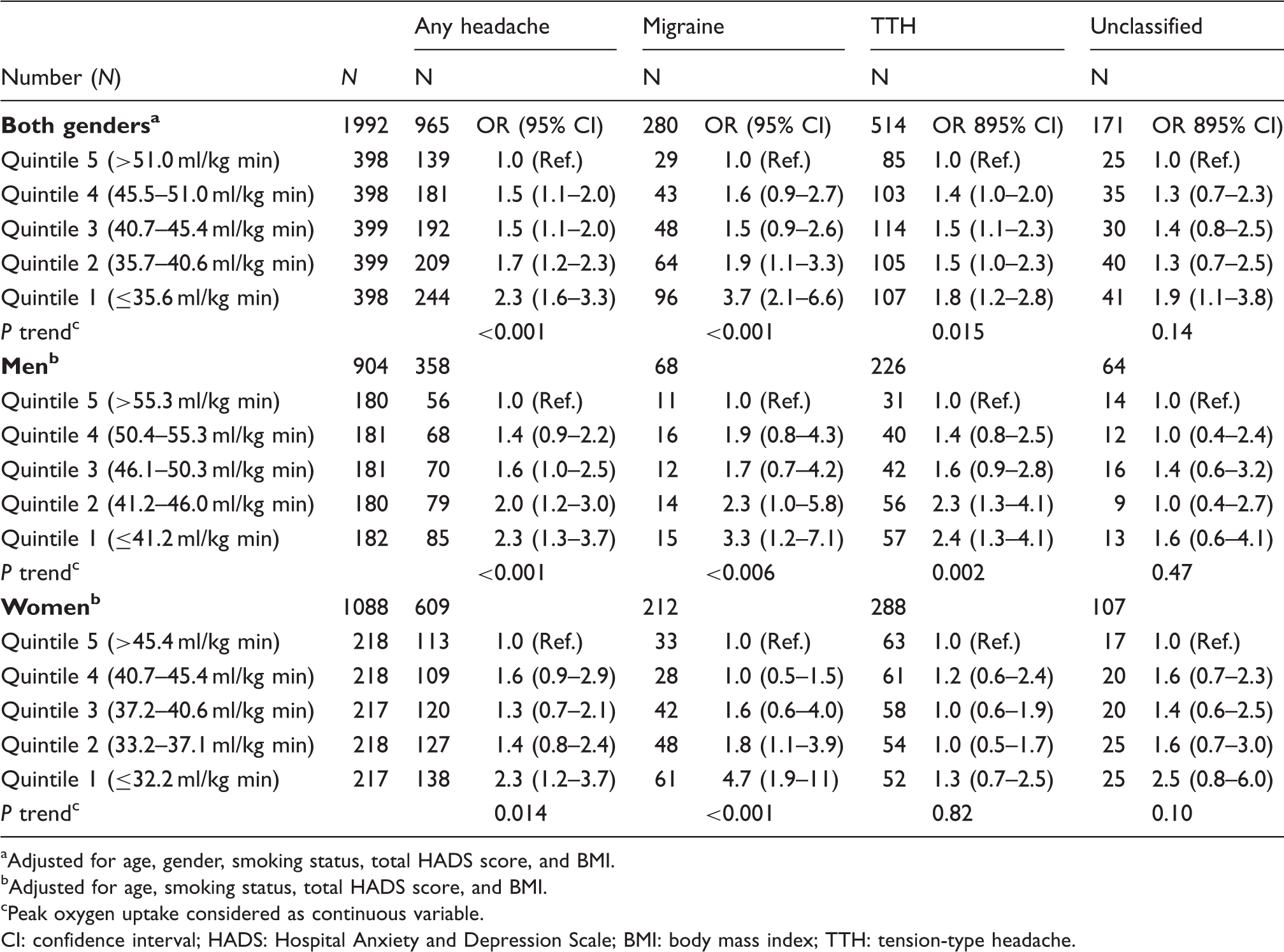
Adjusted for age, gender, smoking status, total HADS score, and BMI.
Adjusted for age, smoking status, total HADS score, and BMI.
Peak oxygen uptake considered as continuous variable.
CI: confidence interval; HADS: Hospital Anxiety and Depression Scale; BMI: body mass index; TTH: tension-type headache.
Odds ratio (OR)1 of headache related to percentiles of peak oxygen uptake (50 years of age or older).

Adjusted for age, gender, smoking status, total HADS score, and BMI.
Peak oxygen uptake considered as continuous variable.
CI: confidence interval; HADS: Hospital Anxiety and Depression Scale; BMI: body mass index; TTH: tension-type headache.
Migraine and influence of physical activity recommended by the ACSM
In the Fitness sample 385 (19.2%) out of 1992 participants age 20–50 years reported physical activity as recommended by the ACSM. Among these, higher prevalence of any headache (OR 2.9, 1.1–8.0) and migraine (OR 6.1, 1.3–29.4) were found for VO2peak scores in the lower quintile. Among the 1609 participants with physical activity below the ACSM recommendations, any headache was twice as likely (OR 2.0, 1.3–3.0) and migraine three times more likely (OR 3.1, 1.5–6.2) for VO2peak scores in the lowest quintile.
Migraine aggravated by physical activity
Participants age 20–50 years in the lowest VO2peak quintile were strongly associated with migraine aggravated by physical activity (OR 4.1, 2.1–8.1).
Discussion
This large cross-sectional population-based study revealed an inverse relationship between VO2peak and headache in adults ages 20–50 years. This was evident both in those who reported physical activity as recommended by ACSM, and in those who did not.
Comparison with other studies
This is the first population-based study evaluating the relationship between primary headache diagnoses and VO2peak. Maximal oxygen uptake has been measured in some clinic-based studies of migraine (see, for example, Varkey et al. (11,12)), but reference data of VO2peak in headache patients from the general population are lacking. In the present study migraineurs had lower mean VO2peak than those who were headache free (Figure 2), and 40% of those with migraine who were younger than 50 years of age had VO2peak below 37 ml·kg−1
Interpretation
There may be several explanations for the particularly high prevalence of any headache and migraine among those with VO2peak scores in the lowest quintile, regardless of level of physical activity. In a cross-sectional design the direction of causality cannot be determined with certainty. The fact that the lowest VO2peak quintile was strongly associated with migraine aggravated by physical activity may at least partly reflect that people with migraine tend to avoid exercise that increase VO2peak because they have experienced that such exercise may trigger headache. This may indicate that low VO2peak is an effect of migraine. On the other hand, one may consider low VO2peak as a potential cause. Thus, one plausible explanation could be that participants with any headache and migraine get less increase in VO2peak from exercise training than headache-free individuals, i.e. they tend to be less responsive to exercise. It has been reported that nearly 20% of adult Caucasians demonstrated little or no change in VO2max in a standardized training program (24). The authors concluded that the trainability of VO2max was highly familial and included a significant genetic component (24). Thus, genetic factors predisposing both for migraine and low VO2peak may explain the inverse relationship between headache and VO2peak (25,26). Interestingly, an endothelial nitric oxide synthase gene polymorphism has been found to be important both for VO2max level and for migraine (27,28). Based on these results, it would be of great interest to investigate the long-term consequences of physical exercise on VO2peak through prospective studies comparing migraineurs to people who are headache free.
In general, regular exercise should be encouraged among headache patients because physical inactivity and low VO2peak are associated with increased mortality (2–4,29), and because exercise in the long run seems to prevent headache (7). Whether exercise regimens that are effective in improving VO2peak should be recommended for headache sufferers needs to be evaluated in a prospective controlled study.
Why the present study did not find any inverse relationship between headache and VO2peak for participants 50 years and older is unclear. Speculatively, participants with headache in the older age group did not avoid exercise more than headache-free individuals, making the fitness level equal. Alternatively, headache in the middle aged and elderly may become less responsive to the factors influenced by physical activity.
Strengths and limitations of the study
The major strengths of this study were the population-based design, the large sample size, objective measure of fitness by VO2peak, and the use of validated headache diagnoses. Although the sensitivity was good and specificity high both for migraine and TTH (18), some misclassification may have occurred. Most likely, the effect of such misclassification will be that differences between migraine and TTH are underestimated. In the multivariate analyses, we were able to adjust for a large number of potential confounding factors. However, the possibility of residual confounding can never be excluded.
Several study limitations should also be considered. First, as mention above, in a cross-sectional design it cannot be distinguished whether associated factors are causes or effects. Second, results should be generalized with caution, partly because only 42% of the invited adults answered the headache questionnaire, and partly because participants in the HUNT3 Fitness Study were healthy and free from cardiovascular disease, hypertension, and cancer. Health indicators clearly showed that the healthiest of the healthy were tested. Of particular relevance is the fact that participants using blood pressure medication were excluded from the HUNT3 Fitness Study. Hence, migraine patients on prophylactic beta blockers or angiotensin II receptor blockers were not included.
In conclusion, this large cross-sectional study demonstrated an inverse relationship between VO2peak and headache for adults younger than 50 years of age.
Clinical implications
An inverse relationship between peak oxygen uptake (VO2peak) and headache was found in adults age 20–50 years. The lowest VO2peak quintile was strongly associated with migraine. Exercise regimens that are effective in improving VO2peak should be recommended for headache sufferers.
Footnotes
Acknowledgments
The Nord-Trøndelag Health Study (The HUNT study) is a collaboration between The HUNT Research Centre, Faculty of Medicine, The Norwegian University of Science and Technology (NTNU); Norwegian Institute of Public Health; and the Nord-Trøndelag County Council. The HUNT Fitness study received funding from the K.G. Jebsen foundation.
Author contributions: KH conceived of the study and performed the statistical analysis. KH, UW, ØE, ML, and LJS all participated in the design and drafted the manuscript. UW took part in data collection. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interests with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.