
Abstract
Background
Migraine is known to run in families. While some clinical studies have indicated that migraine is disproportionally transmitted through the maternal line, this has not been examined in a population-based setting.
Methods
We utilized a large, population-based cohort study from Norway, the HUNT Study. Using a cross-sectional design, our sample consisted of 13,731 parents and 8970 offspring. Logistic regression was used to calculate odds ratios with 95% confidence intervals for active migraine and non-migrainous headache in offspring, given active maternal or paternal headache.
Results
There was a significant association between maternal migraine and offspring migraine (odds ratio 2.76, 95% confidence interval 2.18–3.51). A weaker association (p = 0.004 for comparison with maternal migraine) was found between paternal migraine and offspring migraine (odds ratio 1.67, 95% confidence interval 1.33–2.28). For non-migrainous headache, there was a significant association between mothers and offspring (odds ratio 1.25, 95% confidence interval 1.10–1.43), but not between fathers and offspring.
Conclusions
Parental migraine is associated with offspring migraine, with a stronger association for maternal migraine. This may indicate maternal-specific transmission.
Keywords
Introduction
It has long been known that migraine runs in families, and first-degree relatives of migraine sufferers have a twofold increased risk of developing migraine themselves (1). Twin studies have estimated the heritability of migraine to 45% (2), indicating that genetic factors play a substantial role in this familial transmission. However, non-genetic familial influences may also contribute, as migraine has been linked to, among other factors, previous stressful events (3), socioeconomic status (4), smoking (5), alcohol consumption (inverse association) (5), overweight (5), physical activity (6), and anxiety and depression (3).
Studying migraine within well-characterized families may help delineate the mechanisms of familial transmission, such as selective influences from the mother or the father. Some clinical studies suggest that migraine is mainly transmitted through the maternal line (7–11), indicating a maternal-specific transmission. However, none of these studies included a control group, making interpretation difficult. Furthermore, no studies have examined familial transmission of migraine, separating mothers and fathers, in the general population.
Our aim was to clarify mother-offspring and father-offspring associations of migraine in the large, population-based Nord-Trøndelag Health Study.
Methods
Study population
The Nord-Trøndelag Health Study (HUNT) is a large, population-based cohort study carried out in Nord-Trøndelag county, Norway. In the Adult-HUNT surveys, all adult inhabitants (age ≥ 20) in the county were invited to participate, while in the corresponding Young-HUNT surveys, all adolescents in junior high and high school (age 13–19 years) were invited. In Adult-HUNT, data were collected using questionnaires, including more than 200 health-related questions, and clinical examinations. In Young-HUNT, data collection was mainly performed during school hours, and included self-reported questionnaires, structured headache interviews, and clinical measurements. The Adult-HUNT2 (1995–1997) and Adult-HUNT3 (2006–2008), together with the Young-HUNT1 (1995–1997), Young-HUNT2 (1999–2000), and Young-HUNT3 (2006–2008) Surveys constitute our study sample. An overview of the cohorts and participation rates is given in Figure 1.
Flowchart and participation rates. (a) Participated: Answered the headache questions. (b) Added participants (who had not participated in the previous studies).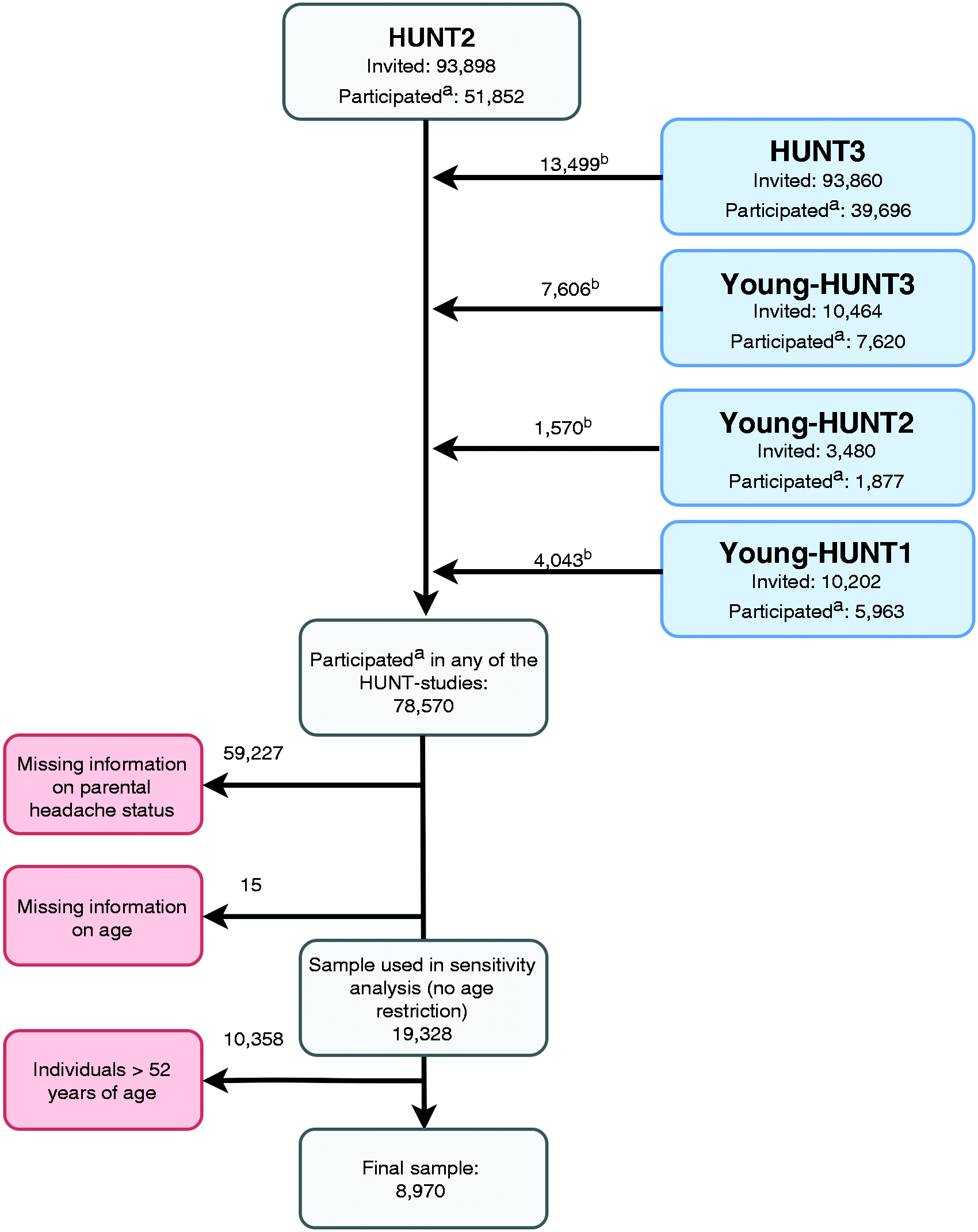
Family information from Statistics Norway enabled us to link the offspring's questionnaires with their parents' questionnaires through the use of personal identification numbers, specific to all Norwegian inhabitants. Statistics Norway also supplied information about the parents' education.
We used the surveys in a cross-sectional design. Since some individuals participated in more than one study, Adult-HUNT2 was chosen as the default dataset. We then added individuals consecutively from each of the following studies, if the individual had not participated in one of the previous studies: Adult-HUNT3, Young-HUNT3, Young-HUNT2 and Young-HUNT1. This means that we have offspring both from Young-HUNT and Adult-HUNT. In total, 78,570 participants responded to the headache questions in any of the studies. In this combined dataset, headache information from parents was linked to their offspring. In the main analyses we excluded individuals >52 years of age, as only current headache was assessed in the questionnaires, and because migraine prevalence decreases strongly after this age (12). Finally, we excluded individuals with missing information on age. Our final study sample consisted of 8970 offspring, 8015 mothers, and 5716 fathers. In a sensitivity analysis to examine how using an age-truncated sample ( ≤ 52 years) affected our analyses, we used a larger sample that included individuals of all ages (19,328 offspring, 16,999 mothers and 13,252 fathers).
Headache diagnoses
Headache, both in offspring and parents, was classified as migraine or non-migrainous headache.
In Young-HUNT, headache diagnoses were obtained through a structured interview, performed by trained nurses. The students were asked if they had experienced recurrent headaches over the past 12 months that were not related to cold, fever, or any other disease. Those who answered “no” constitute the headache-free control group. Those who answered “yes” were considered to have active headache, and were read two typical headache symptom history descriptions, one for migraine and one for tension-type headache and were asked to classify their headache(s) according to these. Those who did not classify their headache as migraine (tension-type headache only, or headache not resembling any of the two descriptions) were classified as having non-migrainous headache. These diagnoses were mutually exclusive. The headache diagnoses have previously been validated according to the criteria of the International Headache Society through clinical interviews by neurologists (13). For migraine, the positive and negative predictive values were 89% and 90%, respectively, and the change-corrected agreement (kappa) was 0.72 (CI 0.58–0.87).
Headache diagnoses in the Adult-HUNT Surveys were assessed using questionnaires and based on a modified version of the International Classification of Headache Disorders (ICHD II) (14). Subjects who answered “yes” to the question “Have you suffered from headache during the last 12 months?” were classified as active headache sufferers. Those who answered “no” constitute the headache-free group. Based on the subsequent headache questions (15,16), headache sufferers were classified as having migraine if they fulfilled the following three criteria: (a) headache attacks lasting 4 to 72 hours (<4 hours was accepted for those who reported commonly occurring visual disturbances before headache); (b) headache with at least one of the following characteristics: Pulsating quality, unilateral location, or aggravation by physical activity; (c) during headache, at least one of the following occurred: Nausea, photophobia and phonophobia. In addition, the participants were asked if they suffered from migraine; those who responded positively to this question were also included in the migraine group. Headache sufferers that did not fulfil the criteria for migraine were classified as having non-migrainous headache, and the diagnoses were mutually exclusive. The headache diagnoses have previously been validated by clinical interviews performed by neurologists. For migraine in HUNT2, the sensitivity was 69% and specificity 89% (κ = 0.59, 95% CI 0.47–0.71) (15). In HUNT3, the sensitivity and specificity for migraine were 49% and 96% respectively (κ = 0.51, 95% CI 0.34–0.68) (16).
In a secondary analysis, we stratified parental migraine into low-frequent (<7 days/month) and high-frequent migraine (≥7 days/month).
Potential confounders
Covariates for each subject were collected from the same survey as their headache status, except for parental level of education, which was available from Statistics Norway. Parental level of education was reclassified into three levels: Primary school, high school, and higher education. Combined anxiety and depression was assessed in Young-HUNT with the Symptom Checklist 5 (SCL-5) (17), using a mean score of >2.0 as cut-off. In Adult-HUNT, we used the Hospital Anxiety and Depression Scale (HADS) (18) using a total score of ≥15 as cut-off to assess combined anxiety and depression. Exposure to smoking at home while growing up was assessed in all five studies and used as a binary variable. Parental weight categories were classified as normal/underweight (BMI < 25), overweight (BMI 25–30) and obesity (BMI ≥ 30). Parental physical activity was classified according to hours of vigorous activity per week, where high physical activity was defined as ≥3 hours/week, moderate physical activity as 1–2 hours/week, and low physical activity as ≥1 hour/week. Since age was not linearly associated with migraine on the logit scale, it was categorized into 5-year groups.
Data analysis
All analyses were performed using a generalized mixed model with logit link, modelling dependencies within families through random effects, and other covariates as fixed effects. We estimated odds ratios (OR) and 95% confidence intervals (CI) for the association between maternal or paternal headache (exposure) and offspring headache (outcome), using headache-free offspring as controls. Separate analyses were performed for migraine and non-migrainous headache. We analysed daughters and sons both separately and combined. Secondary analyses were performed on low vs. high frequent migraine in parents. These analyses were not stratified on daughters and sons because of small sample sizes in each group. For comparison of the effect estimates of maternal and paternal headache, we analysed mothers and fathers in the same model, using a post-estimation Wald test to compare whether the estimates for mothers and fathers were equal. To explore how the use of an age-truncated sample (≤52 years) affected our analyses, we performed (a) a logistic regression analysis of parental age ( < and > 52 years) as predictor and parental migraine as outcome; and (b) a logistic regression analysis of the effect of parental migraine on offspring migraine, where individuals of all ages were included. Two-tailed p-values are reported, using 5% as a cut-off for statistical significance. Identification of potential confounding factors was based on a priori knowledge of possible risk factors for migraine and modelled with a Directed Acyclic Graph (DAG) to visualize causal assumptions (Supplementary Figure 1). The variables considered to be potential confounders from the DAG are listed under “potential confounders” above. We then used the Mantel-Haenszel method to quantify the confounding effect, using a ≥5% change between the adjusted Mantel-Haenszel OR and the crude OR as a cut-off for including the covariate in the final model. Sex and parental and offspring age were not analysed with Mantel-Haenzel, but included as covariates in all analyses, modelled as fixed effects, as migraine is known to vary greatly with sex and age (12). Analyses were performed using Stata/SE 14.1 for Mac (StataCorp LP, College Station, TX, USA).
Participation was based on informed, written consent, and the study was approved by the Regional Committee for Medical and Health Research (#2015/463/REK Central). In addition, the HUNT Study was approved by the Norwegian Data Inspectorate.
Results
The final study population consisted of 8970 offspring, 4830 females and 4140 males, who had available information about headache status from at least one parent. In total, 13,731 parents were included: 8015 mothers and 5716 fathers. Among the offspring, 15.3% of the females and 6.3% of the males had migraine, while 29.5% of the females and 18.4% of the males had non-migrainous headache. Among the parents, 21.8% of the mothers and 10.1% of the fathers had migraine, while 35.8% of the mothers and 26.1% of the fathers had non-migrainous headache.
Characteristics of the offspring, grouped by headache status.
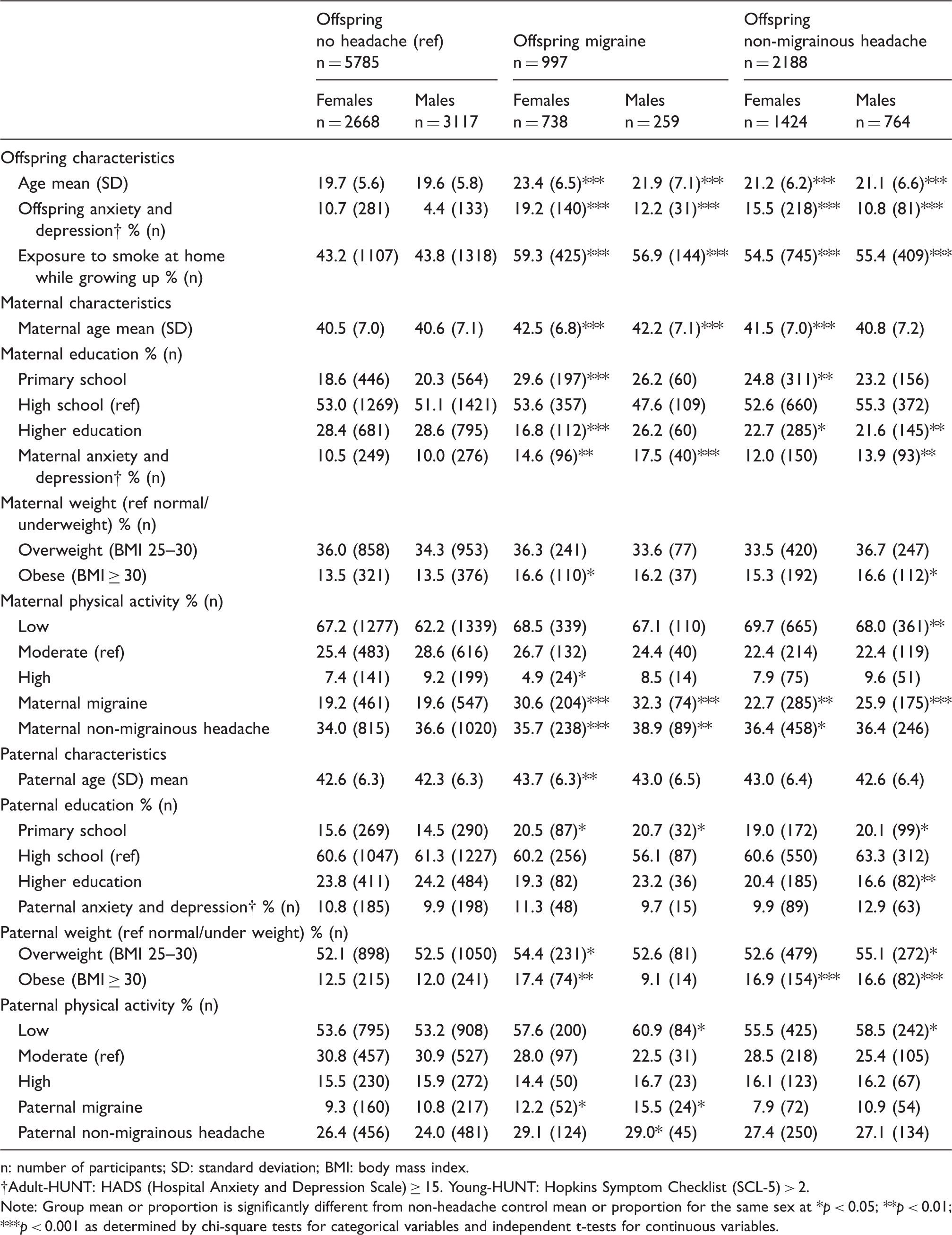
n: number of participants; SD: standard deviation; BMI: body mass index.
Adult-HUNT: HADS (Hospital Anxiety and Depression Scale) ≥ 15. Young-HUNT: Hopkins Symptom Checklist (SCL-5) > 2.
Note: Group mean or proportion is significantly different from non-headache control mean or proportion for the same sex at *p < 0.05; **p < 0.01; ***p < 0.001 as determined by chi-square tests for categorical variables and independent t-tests for continuous variables.
Mantel-Haenszel tests revealed no significant confounders, neither for migraine, nor for non-migrainous headache (data not given), and only parental and offspring age were included in the final models.
Association between parental and offspring migraine.
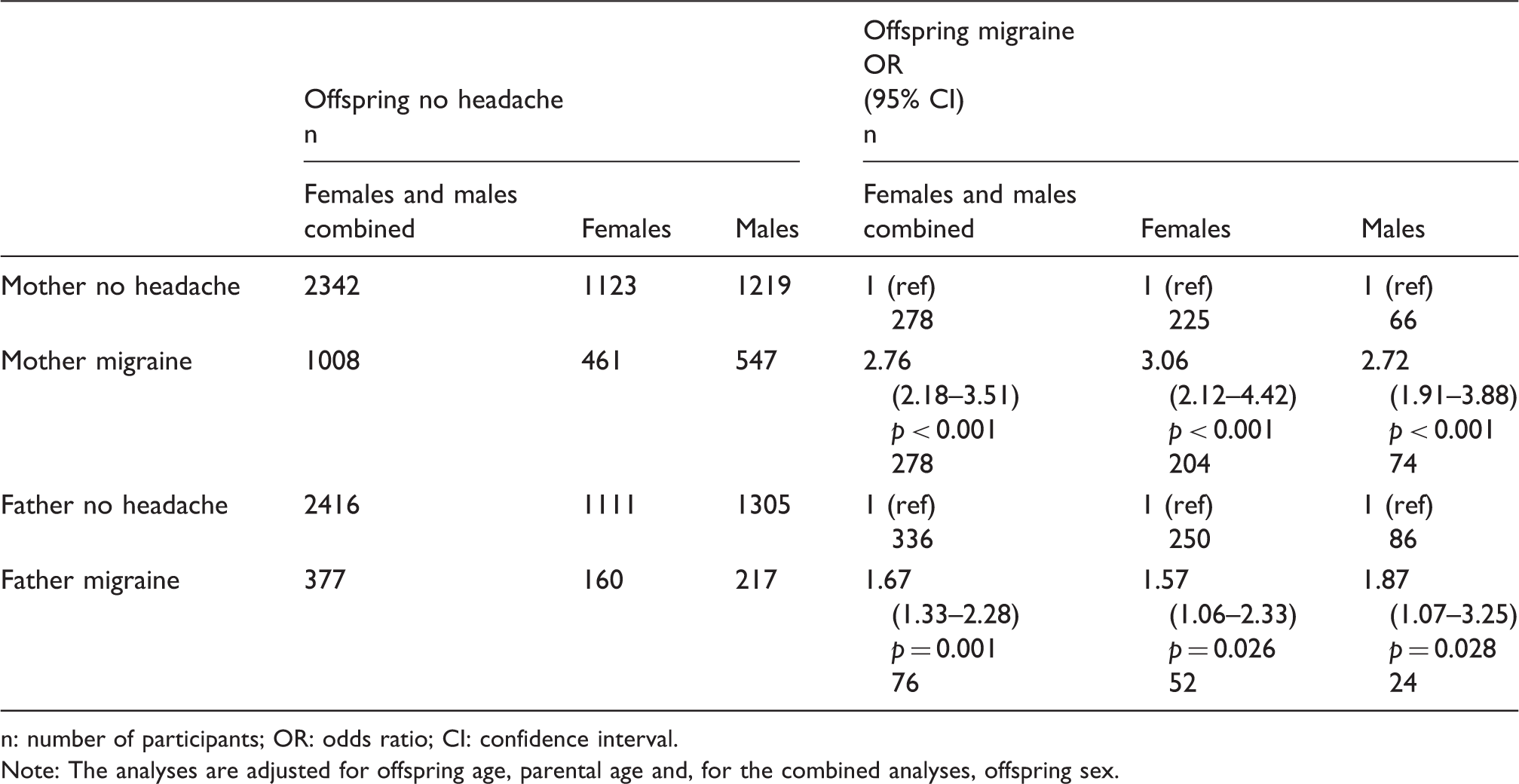
n: number of participants; OR: odds ratio; CI: confidence interval.
Note: The analyses are adjusted for offspring age, parental age and, for the combined analyses, offspring sex.
Additional analyses were performed to examine the effect of using an age-truncated sample (≤52 years of age). Both mothers (OR 0.27, 95% CI 0.25–0.30, p < 0.001) and fathers (OR 0.40, 95% CI 0.35–0.46, p < 0.001) > 52 years of age had reduced odds of having migraine, compared to mothers and fathers ≤52 years of age. When parents of all ages were included in the analyses of the association between paternal headache and offspring headache, the estimates were still significant, but weaker compared to the main analyses, both for mother-offspring (OR 2.54, 95% CI 2.16–2.98, p < 0.001) and for father-offspring (OR 1.93, 95% CI 1.54–2.41, p < 0.001). The stronger association between mother-offspring than between father-offspring remained significant (p = 0.015).
Association between parental and offspring non-migrainous headache.
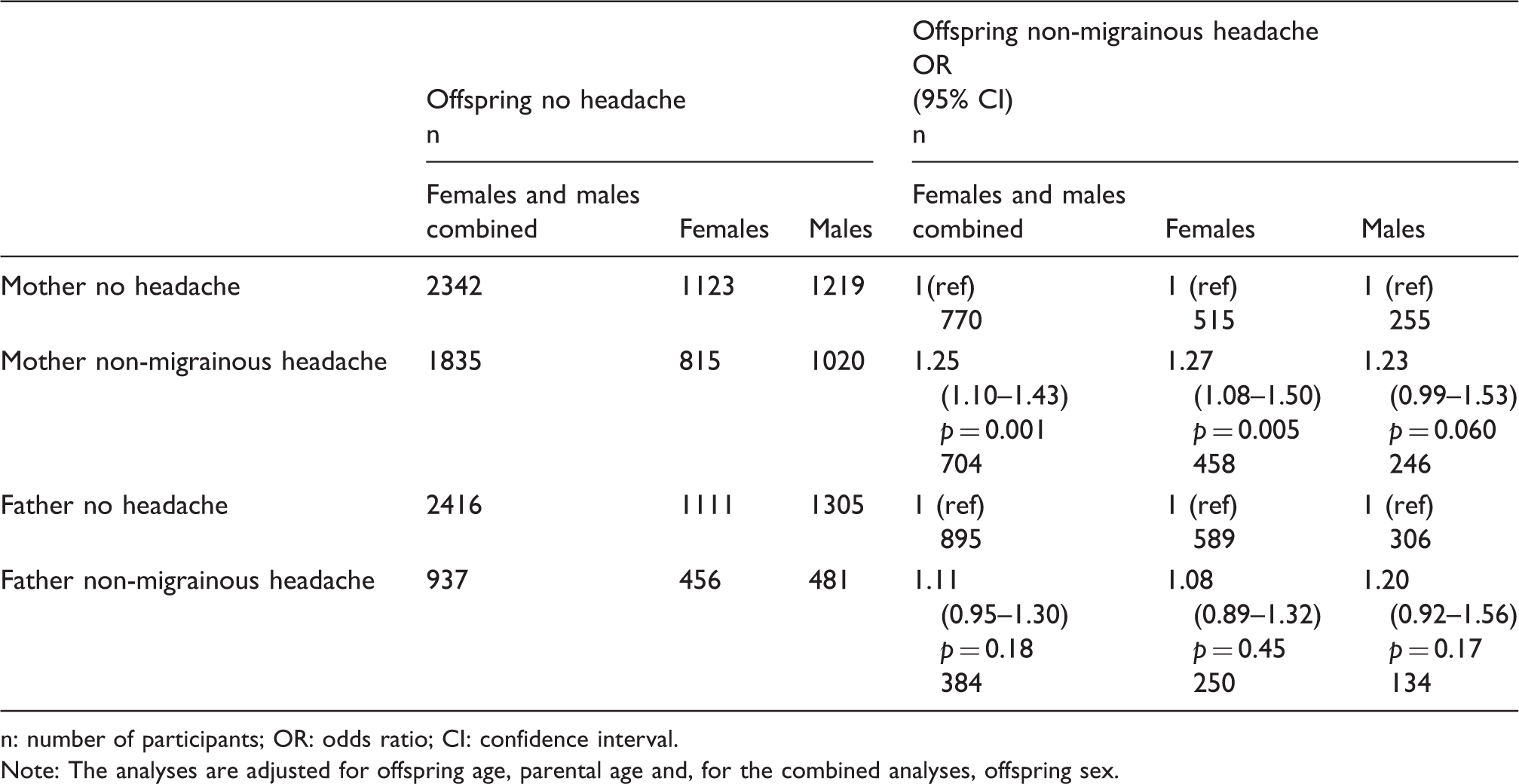
n: number of participants; OR: odds ratio; CI: confidence interval.
Note: The analyses are adjusted for offspring age, parental age and, for the combined analyses, offspring sex.
Discussion
In this population-based study, we found that both maternal and paternal migraine were significantly associated with migraine in their offspring. Mother-offspring associations were significantly stronger than father-offspring associations. The odds for migraine increased by 1.5-fold if the father had migraine, and by 2.9-fold if the mother had migraine, compared to those with headache-free parents.
These results suggest a stronger transmission of migraine from mothers to offspring than from fathers to offspring. This is in line with previous studies suggesting that migraine is mainly transmitted through the maternal line (7–11).
The association between parental and offspring migraine could be due to genetic or environmental factors. It is well known that parental behaviour is important for pain perception and pain behaviour of their children (19). Parental responses to their childrens' pain may influence their development and maintenance of pain (20). It could be postulated that mothers have a stronger influence on their childrens' pain behaviour than fathers, as they are more often the primary caregivers. However, such learned pain behaviour cannot easily explain the observed difference between migraine and non-migrainous headache, both being pain disorders.
Shared environmental factors within the family, causing migraine in both parents and offspring, could also be involved. However, twin and family studies of migraine have not been able to demonstrate an effect of shared family environment on migraine (21). In the present study, offspring with headache were older, and were more likely to have older parents, with higher BMI, lower physical activity, lower education level, more anxiety and depression, being exposed to smoking at home while growing up, and to have anxiety and depression themselves. While previous studies have found associations between headache and all of these factors (3–6), none of the parental and family factors examined in this study was found to affect the association estimates. The age differences are likely due to the prevalence of migraine increasing through adolescence and were adjusted for in the analyses by including age as a covariate.
The stronger maternal influence may alternatively result from genetic factors. Twin studies have estimated that genetic variation accounts for about 45% of the total variation of migraine (2), and, so far, genome-wide association studies have identified 38 risk loci (22).
Migraine is thought to result from the combined effects of genetic susceptibility and environmental risk factors. In a typical “threshold model” for developing disease, the lower risk of migraine in males (23) would need to be a result of a lower environmental risk load, as genetic risk factors are typically shared equally by male and female offspring. This in turn means that males with migraine are expected to have a higher load of genetic risk factors to overcome their otherwise lower propensity for developing migraine. This is termed the Carter effect; individuals of the less-commonly affected sex carry a higher genetic load and are therefore more likely to transmit the disease to their offspring (24). Consequently, males would be expected to pass on migraine to their children more often than females. The fact that the opposite pattern is observed in our study suggests that genetic mechanisms other than typical polygenic autosomal inheritance may be involved. Genetic transmission primarily through the maternal line may be caused by risk variants in mitochondrial DNA, which is inherited from mothers only, or from genetic imprinting. Mitochondrial inheritance or mitochondrial defects have been indicated in migraine (25), but no conclusions can be drawn from existing studies. Genetic imprinting is an epigenetic mechanism in which the phenotypic effect of a genetic risk variant depends on whether it is inherited from the mother or the father (26). Imprinting is implicated in several complex disorders (26), and it has been suggested that it is important in migraine (10). However, no studies directly examining imprinting in migraine have been published to date.
Strengths of this study include the use of a large and unselected population-based sample. Furthermore, the migraine diagnoses were validated and based on the ICHD criteria. The parents and offspring participated in the study independently, meaning they did not influence each other when answering the questions. The general health focus of the questionnaires decreases the risk of a specific selection bias in relation to headache diagnoses and made it possible to evaluate several potential confounding factors.
A limitation of the study is its cross-sectional design, rendering causal inference difficult. We assume that migraine is being transmitted from parents to offspring, through either genetic or environmental mechanisms. However, we cannot exclude the possibility of psychosocial factors having an opposite effect direction; that is, migraine in the offspring causing migraine in their parents. We believe, however, that this is likely to account for a minority of cases. Another limitation is that only active headache was assessed. Migraine prevalence decreases in middle age (12), and for women particularly post menopause (23). Including a large number of older parents, whose migraine had terminated, is likely to lead to a misclassification of migraine. Since the respondents were recruited separately and were unaware of our research hypothesis, such misclassification would likely be nondifferential; that is, independent of offspring headache status, resulting in a deflation of the association estimates. We aimed to limit this effect by excluding parents >52 years of age (median age for menopause for white women in industrialized countries) (27). The use of questionnaire-based headache diagnoses rather than clinical interview will lead to a degree of misclassification between migraine and non-migrainous headache. For adolescents, headache diagnoses also often change between migraine and other primary headache disorders as they grow older (28). The bias caused by misclassification is likely to result in an underestimation of any observed effect. In addition, non-migrainous headache includes a heterogenous group of headache disorders, making interpretations in this group difficult. From the validation study in HUNT2, it was found that 55% had tension-type headache (TTH) and 32% had migraine. The participation rates in the five studies ranged from 42% to 73% (Figure 1) and a selection bias, both in offspring and parents, cannot be ruled out. However, a non-participant study from the Adult-HUNT3, which had the lowest participation rate, found only minor differences between participants and non-participants regarding various conditions, including migraine and headache (29). Lastly, there may be unmeasured confounding factors, including family structure, non-paternity and adoption. For example, children growing up with only one of their parents will share less environmental factors and receive fewer social influences from the other parent. This could deflate the estimates for the other parent. Analysing children living with only one parent could also provide information about the relative genetic and non-genetic influences from the other parent. Therefore, future studies should ideally include information on family structure.
In conclusion, in this large population-based study we found that parental migraine was associated with migraine in their offspring, with a stronger association in mothers than in fathers. In contrast, non-migrainous headache showed weaker parent-offspring associations, significant only between mothers and offspring. While firm conclusions cannot be drawn from this study alone, the results are consistent with indications of a larger contribution from genetic risk factors in migraine and suggests the involvement of maternal-specific transmission; for example, through mitochondrial variants or genetic imprinting. Future studies should examine to what extent these mechanisms contribute to the development of migraine.
Supplemental Material
Supplemental Material1 - Supplemental material for Parental migraine in relation to migraine in offspring: Family linkage analyses from the HUNT Study
Supplemental material, Supplemental Material1 for Parental migraine in relation to migraine in offspring: Family linkage analyses from the HUNT Study by Sigrid Børte, John-Anker Zwart, Synne Øien Stensland, Knut Hagen and Bendik S Winsvold in Cephalalgia
Supplemental Material
Supplemental Material2 - Supplemental material for Parental migraine in relation to migraine in offspring: Family linkage analyses from the HUNT Study
Supplemental material, Supplemental Material2 for Parental migraine in relation to migraine in offspring: Family linkage analyses from the HUNT Study by Sigrid Børte, John-Anker Zwart, Synne Øien Stensland, Knut Hagen and Bendik S Winsvold in Cephalalgia
Footnotes
Key findings
Parental migraine is associated with offspring migraine.
Maternal migraine has a significantly stronger association with offspring migraine than paternal migraine.
Maternal migraine increases the odds for offspring migraine by 2.9-fold, while paternal migraine increases the odds for offspring migraine by 1.5-fold.
Acknowledgements
The Nord‐Trøndelag Health Study (the HUNT Study) is a collaboration between HUNT Research Centre (Faculty of Medicine, Norwegian University of Science and Technology NTNU), Nord‐Trøndelag County Council, Central Norway Health Authority, and the Norwegian Institute of Public Health.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the South‐Eastern Norway Regional Health Authority, grant 2015089 to SB; and the Research Council of Norway, grant 231187/F20 to BSW. The funding sources had no roles in the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.