
Abstract
Background
As there are no biological markers, a detailed description of symptoms, particularly temporal characteristics, is crucial when diagnosing migraine aura. Hitherto these temporal aspects have not been studied in detail.
Methods
We conducted a prospective diary-aided study of the duration and the succession of aura symptoms and their temporal relationship with headache.
Results
Fifty-four patients completed the study recording in a diary the characteristics of three consecutive auras (n = 162 auras). The median duration of visual, sensory and dysphasic symptoms were 30, 20 and 20 minutes, respectively. Visual symptoms lasted for more than one hour in 14% of auras (n = 158), sensory symptoms in 21% of auras (n = 52), and dysphasic symptoms in 17% of auras (n = 18). Twenty-six percent of patients had at least one aura out of three with one symptom lasting for more than one hour. In aura with multiple symptoms the subsequent symptom, second versus first one or third versus second, might either start simultaneously (34 and 18%), during (37 and 55%), with the end (5 and 9%), or after (24 and 18%) the previous aura symptom. The headache phase started before the aura (9%), simultaneously with the onset of aura (14%), during the aura (26%), simultaneously with the end of aura (15%) or after the end of aura (36%).
Conclusion
We provide data to suggest that symptoms may last longer than one hour in a relevant proportion of auras or migraine with aura patients, and that there is a high variability of scenarios in terms of time relationship among aura symptoms and between aura and headache.
Introduction
Migraine is the third most common disorder in the world (1), with 30% of patients having migraine with aura (2). Over time aura has been evaluated with animal models, and in clinical, neuroimaging, vascular, and neurophysiological studies. In clinical studies many aspects have been well investigated, although the duration, the succession of symptoms, and their relation with headache have not been addressed in detail. A detailed description of the symptoms, including their temporal features, is crucial when diagnosing migraine aura, as there are no biological markers. Indeed the differential diagnosis includes cerebrovascular disorders, epilepsy and other life-threatening neurological conditions.
With respect to aura duration a recent systematic review of the topic (3) did not find any article exclusively focusing on the duration of the aura. The authors found 10 articles that investigated migraine with aura features, including the aura duration. Those studies have different limitations such as the fact that most of the studies are retrospective and some of the prospective studies did not use a diary completed during the attacks, putting them at risk for recall bias. Moreover, in some previous studies the diagnostic criteria for migraine with aura were dated or not clearly stated. The pooled analysis of data from the literature on aura duration showed that visual symptoms lasting for more than one hour occurred in 6%–10% of patients, sensory symptoms in 14%–27% and dysphasic symptoms in 17%–60%. Another study investigating the characteristics of migraine visual aura, including duration, has been published recently (4). In that study the design was retrospective, reporting that 6.6% of patients had a visual aura longer than 60 minutes, whereas 7.4% of patients did not remember the aura duration.
With regard to the timing of succession between aura and headache, this has been evaluated in one prospective study on 44 auras (5) and two retrospective studies on a larger number of auras (6,7). The succession of aura symptoms has been evaluated on nine auras in one prospective study (5).
Here we investigated by using a prospective diary-aided approach the temporal characteristics of migraine with aura including the duration and the succession of aura symptoms and the temporal relationship between aura and headache.
Methods
We recruited 176 consecutive patients affected by migraine aura at the Headache Centers of Pavia and Trondheim. The study received approval by the local ethics committees (C. Mondino National Neurological Institute, Pavia and REC-Central, Trondheim) and all patients signed an informed consent form. Enrollment started in October 2012 and ended in July 2014. Inclusion criteria were: i) patients affected for at least one year by migraine with aura fulfilling International Classification of Headache Disorders, second edition (ICHD-2) criteria (8) for 1.2.1 (G43.10) typical aura with migraine headache,1.2.2 (G43.10), typical aura with non-migraine headache, 1.2.3 (G43.104) typical aura without headache, excluding point 3 of C criteria (“each individual aura symptom lasts 5–60 minutes”) and where only one of point C1 or C2 had to be verified to fulfil C criteria; ii) age between 16 and 65 years. Exclusion criteria were: i) hemiplegic migraine; ii) brainstem aura; iii) pregnancy; iv) variation of the characteristics of aura and/or headache in the last six months; v) patients with >2 vascular risk factors; vi) history of myocardial infarction and/or transitory ischemic attack (TIA) and/or stroke and/or other thrombophilic disturbances; vii) patients with episodes that are not clearly differentiated from other disturbances (TIA, seizures).
All the patients prospectively recorded the characteristics of three consecutive attacks in an ad hoc aura diary documenting the exact time for debut and remission of each individual aura symptom and of the headache. The patient was asked to describe each aura symptom to be sure of what was being experienced, and the main characteristics of headache attacks. In the evaluation of the succession of individual aura symptoms where two symptoms started simultaneously, we designated the first completing symptom as the first symptom (FS).
We collected only the diaries of patients who recorded the characteristic of three consecutive auras in their respective diaries.
Results
Patients
Of the 176 patients recruited, 54 completed the diaries during three consecutive auras for a cumulative number of 162 auras recorded. Of the remaining 122 patients, 27 dropped out and 95 did not complete three aura attacks and were therefore not included in the analysis.
The 54 patients with three evaluable aura diaries (46 from Pavia, eight from Trondheim) had the following characteristics: 83% were female (45/54), average age was 40 ± 14 (range: 18–65), the average age of onset of migraine with aura was 23 ± 11 (range: 6–60), average annual frequency of migraine with aura attacks was 23 ± 27 (range: 2–130). A total of 85% (46/54) of these patients had migraine aura with headache in all three attacks, 9% (five of 54) had attacks of both migraine aura with and without headache, and 6% (three of 54) had exclusively migraine aura without headache. Thirty-eight patients also had migraine without aura that started at an average age of 17 ± 8 (range: 7–45) while nine patients suffer also from tension-type headache. Twenty-two percent of patients (12/54) had a familial history of migraine with aura with first- and second-degree relatives being considered. Magnetic resonance imaging (MRI) of the brain was performed in 46 patients; 35 of those (76%) had normal MRI findings, 11 patients (24%) presented with white-matter changes and no other MRI abnormalities were found in any other patient.
Twenty patients out of 54 were treated with migraine preventives during the study period: Three patients were using beta-blockers (two atenolol, one propranolol), five calcium antagonist (four flunarizine, one cinnarizine), four amitriptyline, seven antiepileptic drugs (four topiramate, one valproate, two lamotrigine) and one a combination of antiepileptic drugs and beta blockers (topiramate and propranolol).
Auras
Out of 162 auras that were evaluated, visual symptoms occurred in 158 (97%), sensory symptoms in 52 (32%), and dysphasic symptoms in 18 (11%). The cumulative number of aura symptoms recorded is therefore 229.
The distribution of the various aura symptoms is shown in Figure 1. A total of 107 auras out of 162 (66%) had one symptom, 44 (27%) had two symptoms and 11 (7%) had three symptoms.
Venn diagram illustrating the distribution of the various aura symptoms in 162 auras.
Frequency of different combinations of aura symptoms with respect to the number of symptoms per aura and the order of appearance of each symptom.

V: visual; S: sensory; D: dysphasic.
All the diary data relative to onset and end of each symptom were complete except for a dysphasic symptom whose resolution was not noted as the patient fell asleep. In that case the time of headache onset was recorded as starting before the patient fell asleep.
Duration of aura symptoms
Visual
The median duration of 158 visual symptoms was 30 minutes (min) (interquartile range (IQR) 24.25–45 range 5–10,860 min). They fell in the following ranges: 0–10 min (n = 9; 6%), 11–20 min (n = 28; 18%), 21–30 min (n = 59; 37%), 31–40 min (n = 21; 13%), 41–50 min (n = 6; 7%), 51–60 min (n = 8; 5%), >60 min (n = 22; 14%) (Figure 2).

Distribution of duration aura symptoms subdivided in groups of a period of 10 min until the first hour. Visual symptoms (n = 158), sensory symptoms (n = 52) and dysphasic symptoms (n = 18). Twenty-two out of 158 visual symptoms (14%), 11 out of 52 sensory symptoms (21%) and three out of 18 dysphasic symptoms (17%) lasted for more than one hour.
Somatosensory
The median duration of 52 sensory symptoms was 20 min (IQR 15–45, range 5–1440 min). They fell in the following ranges: 0–10 min (n = 9; 17%), 11–20 min (n = 18; 35%), 21–30 min (n = 9; 17%), 31–40 min (n = 3; 6%), 41–50 min (n = 0), 51–60 min (n = 2; 4%), >60 min (n = 11; 21%) (Figure 2).
Dysphasic
The median duration of 18 dysphasic symptoms was 20 min (IQR 10–50, range 5–105 min). They fell in the following ranges: 0–10 min (n = 5; 27%), 11–20 min (n = 4; 22%), 21–30 min (n = 2; 11%), 31–40 min (n = 1; 6%), 41–50 min (n = 2; 11%), 51–60 min (n = 1; 6%), >60 min (n = 3; 17%) (Figure 2).
The raw distribution of duration of each aura symptom is reported in Figure 3.
Distribution of duration of all aura symptoms. Note that six symptoms (four visual and two sensitive) are not reported as a technical matter as they lasted for more than 420 minutes.
Aura symptoms lasting longer than one hour
As shown in Figure 2, visual symptoms lasted for more than one hour in 22 out of 158 auras (14%), sensory symptoms in 11 out of 52 (21%), dysphasic symptoms in three out of 18 (17%). When considering the aura symptoms as a whole (n = 229), 36 symptoms lasted for longer than one hour (15%). Their duration fell in the following ranges: one to two hours (n = 18), two to four hours (n = 7), four to eight hours (n = 5), 8–24 hours (n = 2), >24 hours (n = 4).
In 29 out of the 162 auras (18%) there was at least one symptom longer than one hour. Out of these 29 auras, in 23 (79%) there was only one symptom lasting for more than one hour, in five auras (17%) there were two symptoms each lasting for more than one hour while in one aura (4%) there were three symptoms each lasting for more than one hour.
Out of the 29 auras with at least one symptom lasting for more than one hour, 12 were auras with one symptom, 12 auras with two symptoms and five were aura with three symptoms.
Fourteen patients out of 54 (26%) experienced at least one aura symptom lasting for more than one hour in at least one of the three attacks. Of these 14 patients, six had all three auras with at least one symptom lasting for more than one hour, while eight (14% of the total 54 patients) experienced the same aura symptoms lasting for more than one hour in one attack and for less than one hour in another attack out of the three.
We performed an analysis to evaluate if there was any demographic or clinical variable associated with having suffered at least one “prolonged aura”, an aura with at least one symptom lasting for more than 60 min, out of three attacks (n = 14 of 54 patients). We included age, gender, presence of headache associated with aura, frequency of migraine with aura attacks, age of migraine with aura onset, duration of illness, co-occurrence of migraine without aura or tension-type headache, age of migraine without aura onset, use of migraine-preventive therapy, familial history of migraine with aura and white-matter lesions on MRI in the analysis. In univariate analyses, none of the clinical parameters was significantly associated with the fact of having experienced a “prolonged aura” (Supplementary Table 1).
Succession of aura symptoms
Auras with at least two symptoms
In 55 out of 162 auras (34%) there were at least two symptoms (44 auras with two symptoms and 11 auras with three symptoms): In 19 auras (34%) the second symptom (SS) started simultaneously with the first symptom (FS) (scenario 1 Figure 4); in 20 auras (37%) the SS started during the FS (scenario 2 Figure 4); in three auras (5%) the SS started when the FS stopped (scenario 3 Figure 4), in 13 auras (24%) the SS started after a free interval of time (median duration 15 min, IQR 5–30 min) after the end of FS (scenario 4 Figure 4). Data relative to the interval between onset of FS and onset of SS are: median 10 min, IQR 0–30 min (mean 21 min, SD 26 min, range 0–120 min). The frequencies of different symptoms with respect to their order of appearance are reported in Table 1.
Different scenarios of time relationship between aura symptom B in relationship to aura symptom A. Scenario 1: B starts simultaneously with A; scenario 2: B starts during A; scenario 3: B starts when A stopped; scenario 4: B starts after a free interval of time after the end of A.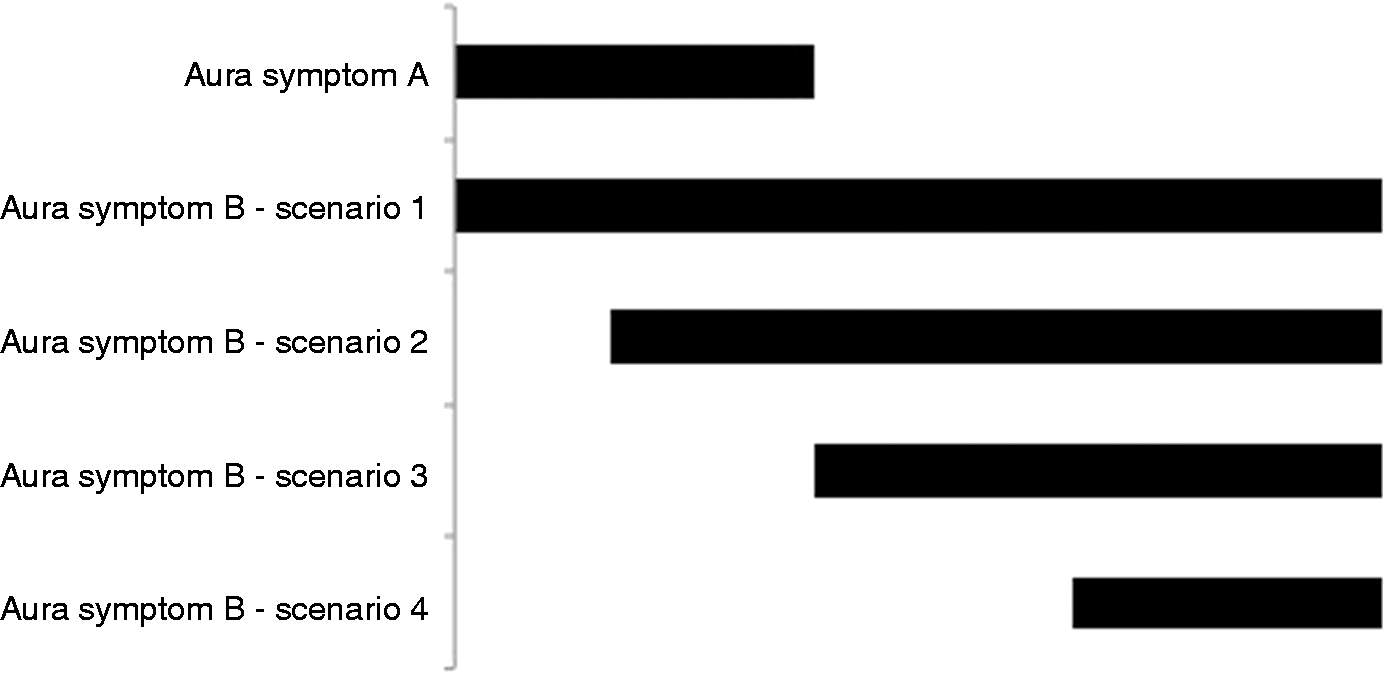
Auras with three symptoms
In 11 auras there were three symptoms: In two auras (18%) the third symptom (TS) started simultaneously with the SS (scenario 1 Figure 4); in six auras (55%) the TS started during the SS (scenario 2 Figure 4); in one aura (9%) the TS started when the SS stopped (scenario 3 Figure 4). In two auras (18%) the TS started after a free interval of time (median duration 70 min, IQR 50–90) after the end of SS (scenario 4 Figure 4). Data relative to the interval between onset of SS and onset of TS are the following: median 25 min, IQR 8, 75–35 min (mean 34 min, SD 39 min, range 0–130 min). The frequencies of different symptoms with respect to their order of appearance are reported in Table 1.
The succession of aura and headache
In 15 auras (9%) out of the total 162, headache was not present and in 31 auras headache was present but we do not have any information about its onset. Of the remaining 116 auras, in 10 (9%) headache started before aura (scenario 1 Figure 5); in 16 (14%) headache started simultaneously with aura (scenario 2 Figure 5); in 30 (26%) headache started during aura (scenario 3 Figure 5), in 18 (15%) headache started when aura stopped (scenario 4 Figure 5), and in 42 (36%) headache started after a free interval of time after the end of aura (scenario 5 Figure 5).
Different scenarios of time relationship between headache in relationship to aura. Scenario 1: headache started before aura; scenario 2: headache started simultaneously with aura; scenario 3: headache started during aura; scenario 4: headache started when aura stopped; and scenario 5: headache started after a free interval of time after the end of aura.
Data related to intervals between aura onset/end and headache onset in different scenarios.

Scenario 1: headache started before aura; scenario 2: headache started simultaneously with aura; scenario 3: headache started during aura; scenario 4: headache started when aura stopped; scenario 5: headache started after a free interval of time after the end of aura (see also Figure 5). Min: minutes.
Intra-patient variability
Of the 54 patients who completed the study, 35 patients experienced all three episodes of auras associated with headache, while others had at least one episode in which aura was not associated with headache (n = 6) or where we do not have any information about headache onset (n = 13). Of these 35 patients, 15 (43%) had the same scenario for the three auras—in particular nine out of the 10 attacks with scenario 1 fell into this group. Twenty patients out of 35 (57%) presented with at least two different scenarios. In this latter group of patients, the differences between scenarios out of three auras were minor. In fact the difference between the higher and lower number of the scenario (see Figure 5) presented for each patient was one in 13 patients (i.e. 2, 2, 1 or 4, 4, 3), two in six patients (i.e. 2, 4, 2 or 2, 2, 4) and three in one patient (1, 3, 4).
Discussion
This prospective, diary-based study of aura demonstrates two important clinical-pathophysiological findings. First, aura commonly, in about 20% of patients, lasts longer than an hour in visual, somatosensory and dysphasic presentations. Secondly, about one-third of patients with aura have two or more distinct brain areas involved. Lastly, in only one-half of patients is there the textbook progression of aura followed by headache. The data suggest, at the least, reconsideration of aura terminology as the ICHD is being revised to include the substantial group with longer aura duration. Moreover, aura pathophysiology and its relationship to headache need to be re-thought if current models fail to predict the clinical data in half of cases.
The distribution of aura symptom duration was not normal. Most of the symptoms lasted for 20–30 min as the median shows; indeed they can be longer than one hour in a significant proportion of auras (18%) and of patients (26%). These data are in line with the results of the systematic review on aura duration (3) although here we did not find relevant differences in terms of aura duration between the three aura symptoms. In the ICHD third edition beta (ICHD-3 beta) (9) “migraine with typical aura” 1.2.1, it is stated that “each individual aura symptom lasts 5–60 minutes.” Our data offer two options. First, does the one-hour limit need review? Secondly, and as an alternative, should the nosological entity defined as “migraine with prolonged aura” included in ICHD-1 (10) and dropped in ICHD-2 (8), be reintroduced in ICHD-3? With respect to the time limit of symptoms duration, we note our data show that 95% of aura symptoms (218 out 229) last between five min and four hours, while just 5% of symptoms (11 out of 229) lasted for more than four hours (five between four and eight hours, two between eight and 24 hours, four >24 hours). Indeed, for the first time we have provided consistent data that show that aura symptoms can last for more than one hour in a substantial proportion of migraine patients and migraine auras. We favor the one-hour rule as it does cover 80% of aura, and would have no effect on data from the last 25 years. Clinically, the result that migraine aura symptoms not infrequently exceed the one-hour limit should be disseminated widely to avoid unnecessary investigations.
We evaluated a succession of individual aura symptoms in 55 auras with at least two symptoms and 11 auras with three symptoms. We noted that the subsequent aura symptoms might either start simultaneously, during, with the end, or after, the previous aura symptom (see four scenarios in Figure 4). Only one previous prospective diary-based study (5) reported data on this issue, describing the time relationship of two symptoms in nine auras. They fell in scenario 2 (five out of nine) and in scenario 4 (four out of nine). In ICHD-3 beta it is stated “aura symptoms of these different types usually follow one another in succession.” We propose a change to “aura symptoms usually follow one another in succession, the second one starting during, with the end, or after, the previous aura symptom, although they can also start simultaneously.” We also noted that aura symptoms might occur in different order, and not just visual—sensory and dysphasic. This concept is reported in ICHD-3 beta although in the literature no studies reported data on this aspect.
Frequency of the five different scenarios of time relationship between headache in relationship to the aura, in the studies available in literature and in the current one.

Scenario 1: headache started before aura; scenario 2: headache started simultaneously with aura; scenario 3: headache started during aura; scenario 4: headache started when aura stopped; scenario 5: headache started after a free interval of time after the end of aura (see also Figure 5).
Patients recorded time of onset/end of aura and headache during their occurrence.
The patients had to answer a question about the time relationship between onset of headache and aura (before, during and after) and to quantify the “duration before/after.”
Auras were 54 but in some auras data were not complete. *This value refers to scenarios 3, 4 and 5 together.
Our data prospectively verified criteria C4 of migraine with aura of ICHD-3 beta (9), “the aura is accompanied, or followed within 60 minutes, by headache” in 96% of cases in which headache started after a free interval of time after the end of aura. In ICHD-3 beta it is not noted that headache may start simultaneously or before aura onset, although this was documented in a significant proportion of auras (up to 21%), as shown by this study and the three previous ones reported in Table 3. Our study shows that patients usually present with the same or similar scenario(s) of succession of aura and headache during different auras. These data are particularly interesting if we consider that almost all the patients (75%) who have experienced scenario 1—headache starts before aura—retained the same scenario for all three auras.
The main limitation of this study is that patients were recruited from tertiary referral centers. One could then argue that in such a setting more difficult cases are seen or unusual aura is referred for evaluation. This would account for the longer or more complicated aura presentations. We cannot, therefore, be clear what the population proportion of these aura phenomena are with these data. This does not negate the observations’ accuracy, since all patients were reviewed by experts who re-took the history of secondary and aura-like presentations. Practically speaking the use of a detailed aura diary in a population-based study has its challenges, and population-based studies always have the issue of how detailed one can make the clinical evaluation. Despite selection bias, the overall pathophysiological message must remain one of caution since undoubtedly aura length, succession and relationship to headache are not one simple linear, time-restricted set of phenomena.
In conclusion, we performed the first study specifically designed to evaluate temporal aspects of migraine aura. It provides consistent results that give wider insight into aura phenomenology such as the fact that aura symptoms may be longer than one hour in a significant proportion of auras or migraine with aura patients, and into the high variability of the temporal relationship between aura symptoms and between the onset of aura and headache. We are confident that these data can provide reliable support in the clinical setting, the classification process, as well as the pathophysiological research in migraine with aura.
Clinical implications
Unless very important, aspects hitherto of temporal features of migraine with aura have not been studied in detail. Here we present data from an extensive, careful analysis of aura in a well-characterized clinical cohort. We provide data on duration that suggest aura is often longer than currently thought, careful documentation of succession of aura in patients with more than one manifestation, and new data on the relationship with headache that has been debated much from bench studies. Our data will press for improvements to the International Classification of Headache Disorders and offer new avenues for bench work as well as provide reassurance in clinical settings that seem more common than has been considered.
Footnotes
Acknowledgments
This study was carried out in collaboration with the University Consortium for Adaptive Disorders and Head Pain (UCADH), University of Pavia, Italy.
Declaration of conflicting interests
MV, ML, GS, NG, EG, MA, ST, GN, CT have nothing to declare. PJG reports grants and personal fees from Allergan, grants and personal fees from eNeura, personal fees from Autonomic Technologies Inc, grants and personal fees from Amgen, personal fees from Bristol-Myers Squibb, personal fees from AlderBio, personal fees from Pfizer, personal fees from Impax, personal fees from Dr Reddy, personal fees from Zosano, personal fees from Colucid, personal fees from Eli Lilly, personal fees from Medtronic, personal fees from Avanir, personal fees from Gore, personal fees from Heptares, personal fees from Nupathe, personal fees from Teva, personal fees from MedicoLegal work in headache, personal fees from Journal Watch, and personal fees from UpToDate, outside the submitted work.
Funding
This work was supported by grants from the Italian Ministry of Health to RC 2013–2015.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.