
Abstract
Background: Migraine aura, made up of one or more neurological symptoms arising from the cortex or brainstem, is a complex neurological phenomenon. Visual aura is the most frequent aura manifestation. Studying the subjective components of visual aura makes it possible to identify common characteristics.
Objective: To thoroughly describe the characteristics of migraine visual aura in patients with migraine with aura.
Methods: We performed a retrospective, descriptive study of the visual aura of 122 migraine patients collected at two headache clinics in the Americas. This study was designed to determine the characteristics of a typical visual aura.
Results: The most common features of the visual aura in our study are that it occurs before the headache with a gap of less than 30 minutes, lasts 5 to 30 minutes, has a gradual onset, usually begins peripherally, is unilateral, and shimmers. Furthermore, the location of typical visual aura in the visual field has no fixed relationship to headache laterality, is slightly more often without color, and is often described as small bright dots and zigzag lines. Blurred vision, not typically considered to be an aura phenomenon of cortical origin, is in fact the most frequently reported visual symptom.
Conclusions: Migraine visual aura is heterogeneous and pleomorphic, and some of our findings run contrary to common beliefs.
Introduction
Migraine with aura (MwA) is estimated to occur in about 28% of migraineurs, based on the mean rate of ten population-based studies (1–10), ranging from 11.9% in Japan (2) to 44.3% in Croatia (1). Elementary visual phenomena are the most frequently described migraine aura, being reported by 92–99% of MwA patients (11–13).
Migraine visual auras may manifest in a myriad of ways. There are many aspects that must be considered: the frequency, consistency, uniformity, duration, timing, temporal relation to the headache, location in the visual field, and characteristics of the visual phenomena. The classical ‘fortification spectra’ (teichopsia), while generally considered typical of the ‘classical aura’, is not the most frequent visual manifestation (14).
A detailed description of the aura is essential to make the correct diagnosis of MwA. The differential diagnosis of aura includes transient ischemic attacks and epilepsy. Panayiotopoulos (15,16) has stated that the color of the visual hallucinations is a main feature to differentiate occipital seizures from visual auras, the former being usually multicolored, with circular/spherical forms, and the latter mostly black-and-white, with linear/zigzag lines. The color aspect of the visual auras has rarely been studied or documented in the medical literature (13,14,17). Russell et al. (17), in a prospective study of 54 attacks of migraine aura in 20 patients, reported colored auras in 13 attacks (24%).
The aim of the present study was to thoroughly describe the characteristics of migraine visual auras in MwA patients from two headache centers, in Southern Brazil and Northern USA.
Methods
This was a retrospective, descriptive study. From May 2009 to March 2010, we have evaluated 122 patients (102 women and 20 men) with the diagnosis of MwA using a structured questionnaire. All patients were seen consecutively at either the Clinica do Cerebro, Florianopolis, Santa Catarina, Brazil (72 patients) or the Ophthalmology Department of the University of Rochester, Rochester, NY, USA (50 patients). We have included all patients during this period who came to either a new evaluation or repeat office visit with the diagnosis of MwA. Patients who had MwA without visual symptoms were not included. Those with only blurred vision as visual phenomena were also not included. No patient refused to participate. Although the USA patients were seen at an Ophthalmology Department, the author (DIF) sees headache patients as a general neurologist with an interest in headaches, not only as a neuro-ophthalmologist. The mean age of respondents was 41.6 ± 13.9 years, ranging from 18 to 78 years of age.
The diagnosis of subtypes of MwA were made by two of the authors (LPQ and DIF), based on the second edition of the International Classification of Headache Disorders (ICHD-II (18).
The questionnaires were completed in the waiting rooms by the patients, and if there was any doubt about how to answer certain questions, this was discussed personally with the authors. The variables evaluated included: age; sex; the presence of other types of aura; age at the time of the first migraine and first aura; the frequency of visual auras; the timing of the visual auras in relation to the headache; duration of visual auras and of the free interval (the gap between the end of the aura and the onset of the headache); the pattern of the onset of visual auras; the starting location in the visual fields of visual auras; movement or ‘buildup’ (spreading of the visual auras to contiguous areas) of visual auras across the visual field; presence or absence of shimmering of visual auras; the laterality of visual auras and its relationship to that of the headache; the presence of colorful aura; the characteristics of the visual phenomena (checklist and drawing); the consistency of the visual auras over time; and the number of different patterns of visual auras. A copy of the questionnaire is provided as a supplementary data.
This study was approved by the University of Rochester Research Subjects Review Board (RSRB # 26944).
Results
The mean age at the time of the first migraine headache was 17.6 ± 9.9 years; and the first visual aura was 21.0 ± 11.4 years. Among the 122 patients, 101 (82.8%) had as their main diagnosis typical aura with migraine headache; 9.0% had typical aura with non-migraine headache; 4.9% had typical aura without headache; and 3.3% had probable migraine with aura. Eight patients (6.6%) had a second MwA diagnosis: six with typical aura without headache and two with probable migraine with aura (some attacks with prolonged visual auras). Only 40 (32.8%) patients reported having additional types of aura (36 sensory auras, 21 speech disturbances and 8 motor symptoms).
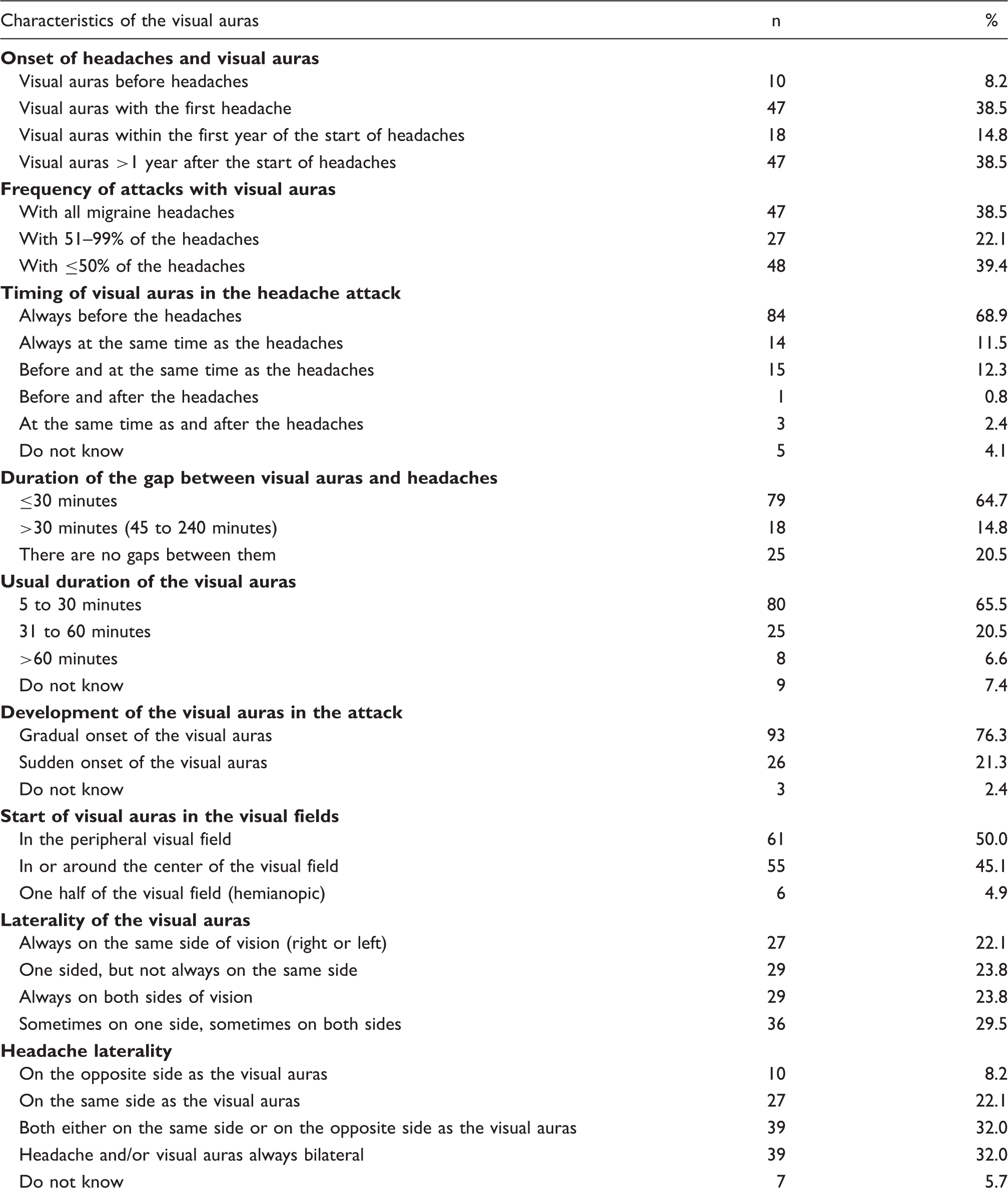
Distribution of patients according to some of the visual auras characteristics (n = 122)

The most common visual phenomena were blurred vision (54.1%) and small bright dots (47.5%). Only 41.8% described the classic zigzag lines and 16.4% the typical ‘C’ shape or crescentic form (Table 2). Figure 1 shows some of the patients’ drawings of their aura patterns. The majority of patients (73.8%) had just one aura pattern; a few had two to six different patterns of visual auras.
Examples of visual auras as depicted by the patients. Distribution of patients according to the characteristics of the visual phenomena (n = 122)

Discussion
This study has evaluated in detail many characteristics of migraine visual auras. It included patients with MwA from North and South America: Southern Brazil (Florianopolis, Santa Catarina) and Northern USA (Rochester, NY).
The great majority of patients had the diagnosis of typical aura with migraine headache. Only eight patients had two subtypes of MwA. To our knowledge, there are no other published studies classifying the subtypes of MwA according to the ICHD-II. Cologno et al. (19) reported a higher proportion of patients (19%) with two subtypes of MwA, as well as a 6% rate of migraine aura without headache. Eriksen et al. (11) also found 6% of migraine aura without headache, and Russell and Olesen (13) 4.3%.
In our sample, the mean age of onset of headache was lower than the mean age of onset of visual auras. This reflects the finding that in only 38.5% did the aura start at the same time of the first migraine headache. Queiroz et al. (14) have also reported 39% of headache and aura starting at the same time.
We found that visual auras occurred in every migraine attack in 38.5% of the patients. This was higher than previously reported by Queiroz et al. (19% (14)), and Kelman (21% (12)), but lower than the rates described by Russell and Olesen (62% (13)) and Eriksen et al. (64% (11)).
Regarding the timing of the aura, most of our patients noted that migraine visual auras occurred exclusively before the headache. Queiroz et al. (14) found this in 57%, Kelman (12) in 67.4%, and Russell and Olesen (13) in 92%.
The usual duration of the visual auras was 5 to 30 minutes. Similar findings were reported by Queiroz et al. (14) (59%), Kelman (12) (63%), Bana and Graham (20) (64.7%), Cologno et al. (21) (65.4%), Russell and Olesen (13) (69%), and Manzoni et al. (22) (75.6%). It is worth noting that many patients whose auras usually last 5 to 60 minutes during a typical MwA attack also have some attacks of visual illusions that are shorter than 5 minutes and/or longer than 60 minutes.
Similar to the studies of Eriksen et al. (11,23) (69% and 81%) and Russell and Olesen (13) (91%), the majority of our patients noted a gradual onset of visual aura symptoms.
Although it is classically described that visual auras originate in or adjacent to the center of the visual field, half of our sample indicated that their visual auras began in the periphery. Eriksen et al. (11) reported that ‘visual aura more often started peripherally than centrally in the visual field’ (49% and 28%, respectively). Queiroz et al. (14) also found a higher proportion (56%) of visual auras starting in the periphery of the visual field.
Unilateral auras were described by the majority of our sample. Eriksen et al. (11) found unilaterality in 62%, Eriksen et al. (21) in 62.5%, and Russell and Olesen (13) in 69%.
Of the 122 patients, 76 had unilateral auras and unilateral headaches, at least in some migraine attacks. Only ten of them noted their headaches were always contralateral to the auras. This low proportion (8.2%) may be due to recall bias. But it is noteworthy that additional 32% reported headaches both either on the same side or on the opposite side of the visual auras. Queiroz et al. (14) described this contralaterality in only 16% and Manzoni et al. (22) in 48.7%. Russell et al. (17), in a prospective recording of migraine auras, reported that the headache was contralateral to the visual aura in 27 of 52 attacks (52%). Olesen et al. (24) have also prospectively studied headache and aura laterality, including regional cerebral blood flow (rCBF). They found that changes in rCBF are virtually always unilateral, and aura symptoms originate from areas with low blood flow. Unilateral abnormalities in rCBF were significantly associated with ipsilateral or bilateral headache; unilateral aura was significantly associated with contralateral or bilateral headache; and unilateral abnormalities in rCBF and aura symptoms were mostly contralateral to each other. Sanchez del Rio et al. (25), with perfusion weighted imaging, also observed unilateral blood flow decrease limited to the hemisphere contralateral to the hemifield of the visual aura, and the headache of all patients studied were ipsilateral to the occipital hypoperfusion. Bilateral headache, and even contralateral headache, may develop because of stimulation of midline structures (vessels, sagittal sinus), which receive bilateral innervation; in addition, both the brainstem and the thalamus receive bilateral input to some extent (24,25).
The high percentage of our patients experiencing colorful aura refutes the notion that the color of an unformed visual hallucination is a major distinguishing feature between MVA and occipital epilepsy. The previously held concept was that visual auras are usually black-and-white, and occipital seizures are commonly multicolored (15,16). This is clearly not the case, and the presence or absence of color cannot be used clinically to distinguish these entities. The exact percentage of patients in the population experiencing colorful auras remains uncertain, as ours was a clinical-based, retrospective study, subject to selection and recall bias. Russell et al. (17), in their prospective study, reported colored auras in only 24% of the attacks. Russell and Olesen (13) found colorful visual auras in 36%, in a population-based study, similar to our results.
Descriptions of the visual phenomena of MwA are found widely in the literature, as physicians’ self-observations (26–29), in clinical settings (12,14,19,20,22), and even in population-based studies (11,13). Although the ‘typical aura’ described is the fortification spectra, with zigzag lines and a ‘letter C or crescent’ shape, this is not the most frequent description of visual auras by patients ‘in real life.’ In our study, the most common visual symptom was ‘blurred/foggy vision’. However, this visual disturbance alone was not considered a visual aura; all patients with blurred vision also reported having other types of visual illusions. The smaller percentage of blurred vision (27%) from the study of Queiroz et al. (14) probably represents ascertainment bias. The pathophysiology of this symptom is uncertain.
The second most frequent visual hallucination was ‘small bright dots,’ which is similar to the 42% found by Queiroz et al. (14). Other commonly described visual phenomena were ‘zigzag/jagged lines’, ‘flashes of bright light (photopsias)’, ‘blind spots’, ‘flickering lights’, and ‘as looking through heat waves or water’. Zigzag lines were noted by 58% of the Eriksen et al. patients (23) and by 81% of Russell and Olesen’s patients (13). We had a surprisingly high rate of the corona phenomenon (an extra edge around people and objects), given that this was described by only 2% in the Queiroz et al. study (14). Other relatively common complex visual hallucinations included seeing things ‘like a mosaic’ and as if ‘things were farther away than they really were’. Complex visual auras have been frequently described in the medical literature (30–36).
The strengths of our study include a large number of patients from two different countries, and the level of detail afforded by the questionnaire. There are some limitations that need to be acknowledged regarding the present study. The first one concerns to the source of patients, who were clinic-based, and we cannot extrapolate our findings to the general population. Most previous studies about MwA were performed in tertiary care centers, (12,14–17,19–22), however; only two studies were population-based (11,13). Although most of our patients had experienced migraine visual aura for years and provided detailed descriptions of their experiences, our study may be limited by recall bias as questionnaires were completed based on patients’ recollections of their previous migraine attacks. A more accurate description of the characteristics of their MwA episodes would be best obtained using a prospective aura log (17), where patients would use a chronometer, describe and draw their visual auras when, or just after, the visual phenomena had occurred. This will be considered for future studies.
In conclusion, migraine visual auras are very heterogeneous and pleomorphic. Based on our study, a ‘typical’ visual aura occurs before the headache, with a gap of less than 30 minutes; lasts 5 to 30 minutes; has a gradual onset; and arises in the peripheral visual field. It is unilateral; moves across the visual fields and shimmers; has no fixed relationship to headache laterality when it is unilateral; is black-and-white (but can be colored); and is often described as blurred vision, small bright dots, and zigzag lines.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
There is no conflict of interest related to this study.