
Abstract
Background
Patients with traumatic spinal cord injury (TSCI) often suffer from different types of pain. However, headaches after TSCI have not been studied.
Aim
The aim of this article is to examine the occurrence of headache among patients with TSCI.
Methods
This cross-sectional study included individuals with TSCI from 1997 to 2012 in Estonia. Patients with TSCI were interviewed via telephone. The interview was based on a questionnaire specifically designed to identify headache type using the International Classification of Headache Disorders, third edition (beta version).
Results
There were 73 patients with a mean age 37.1 ± 10.6 years. The mean time since TSCI was 7.5 ± 4.0 years. The most frequently mentioned pain was headache (71%), followed by back pain (60%) and pain in neck (44%).
Headaches were more frequent after the trauma compared with the headaches before TSCI (71% vs 51%, p = 0.02). Headaches that arose after TSCI were not related to the concomitant brain injury (p = 0.15). The occurrence of headache did not depend on the severity or the level of the TSCI.
Eighty-five percent of patients had not contacted any physician and headache was not diagnosed.
Conclusions
This is the first study that evidentially shows that headache is the most prevalent pain condition after TSCI. Despite this, the majority of patients never consult a physician, nor is their headache diagnosed or appropriately managed. This indicates that further studies are needed to provide evidence regarding the prevalence and causes of headache and its impact on quality of life.
Introduction
Patients with traumatic spinal cord injury (TSCI) experience a number of secondary health conditions after the injury. Pain is one of most common symptoms and conditions (1). As TSCI directly affects the somatosensory system, the patients may experience different types of neuropathic pain. As pain among patients with TSCI is heterogeneous and the presence of pain decreases quality of life, each pain should be evaluated and treated (2). Despite the known fact that the lifetime prevalence of headache is as high as 89% in the general population (3), to our knowledge the occurrence of headaches after TSCI has never been systematically investigated (2,4).
The primary aim of this study was to examine the occurrence of headaches after TSCI. Secondary aims were to identify the characteristics of headache and to assess the predictors of headache in patients with TSCI.
Methods
This epidemiological, population-based, retrospective study included all known and consented Estonian individuals with TSCI from 1997 to 2012. The patients were identified from the Estonian TSCI database from 1997 to 2007 (5) and in addition from the list of patients in Haapsalu Neurological Rehabilitation Centre, the rehabilitation unit in Estonia managing patients with TSCI, from 2008 to 2012.
The patients with TSCI were interviewed via telephone in their native language (Estonian or Russian language). All individuals were contacted between February 2014 and April 2014.
Information such as demographics and injury-related data at the time of injury were obtained from medical records. The interview was based on a self-made structured questionnaire (Appendix 1) specifically designed to identify headache type using the International Classification of Headache Disorders, third edition (beta version) (ICHD-3 beta) (6). It consisted of pain history questions: Participants were asked to indicate the areas where they experienced pain and to rate the mean pain severity on a numeric rating scale (NRS). Further questions were related to headache. Once the presence of headache was defined, the participants were asked about the frequency, location and characteristics of the headache. The patients with headache could choose from the following alternatives: 1) less than once a month, 2) one to 14 days per month, 3) 15 days per month or more. Participants indicated the location of headache that was divided into seven head sections: temporal, crown, nape, neck, face, eye, and/or forehead.
The patients described their headache using the following descriptors: pressing/tightening, throbbing/pulsating, stabbing or lancinating. An 11-point (0–10) NRS was used to rate the intensity of the headache. Patients were asked about the preceding complaints/symptoms. A list of 11 complaints was given: visual disturbances (excluding diplopia), diplopia, paresthesias, speech disturbances, general fatigue or weakness, weakness of one side of the body or one extremity, dizziness, drowsiness, memory problems, mood disorders, other. To identify accompanying symptoms, patients chose from the list: no accompanying symptoms, nausea, vomiting, fear of light, fear of noise, fear of smell, aggravated by or causing avoidance of routine physical activity, stiffness of the muscles in head, neck or shoulder region, drowsiness, restlessness, agitation, signs on the same side with the pain: eye redness or lacrimation, nasal congestion or running nose, eyelid edema or drop, forehead or facial sweating, flushing, sensation of fullness in the area, changes in the diameter of the pupil.
The patients with headache were also asked about the presence of factors that could provoke their headache: cough, physical effort, sexual activity, traveling by plane, sleep, other. A list of factors affecting headache were presented to participants: no factors, certain drinks or food, alcoholic drinks, hunger, thirst, lack of water, stress/mental pressure, physical tension, stress, forced positions, working with a computer, looking at a screen, changes in sleeping pattern, weather changes, menstruation, touching or pressing some areas of the head/face, brushing teeth, chewing, traveling at high altitude, other.
The patients reported whether they were taking any abortive medications and if they did, what did they use and how often. Participants were asked if they had had headaches before the TSCI. If participants previously presented their complaint of headache to a physician, they were asked if the headache was diagnosed and what the diagnosis was.
The study was approved by the Research Ethics Committee of the University of Tartu, Estonia.
Descriptive data are presented as number, percentage, mean and standard deviation. We used the t-test for continuous variables and Chi-square test for differences of categorical data. A statistical level of significance of 5% was used (p < 0.05).
Results
Patients’ basic characteristics.

UNK: unknown; AIS: American Spinal Injury Association Impairment Scale; MVA: motor vehicle accident.
Seventy-one patients (97.3%) reported having some kind of pain. The most frequently reported pain was headache (71.2%, Figure 1). Men and women reported headache equally (p = 0.39). Back pain and neck pain were also quite frequent. Headache was an isolated condition in only two patients. Headache was more frequent after the trauma than before (52 patients (71.2%) after vs 37 patients (50.7%) before TSCI, p = 0.02). The patients who had had headache before TSCI were younger (34.3 ± 10.1 years vs 40.0 ± 10.6 years, p = 0.02), but the age of the patients who experienced new headache post-TSCI was not significantly different from the rest of the group (39.5 ± 10.0 years vs 36.5 ± 10.8, p = 0.33). The headaches that arose after TSCI were not related to the concomitant brain injury (p = 0.15).
Regions of pain in patients with traumatic spinal cord injury.
The mean severity of headache was 6.9 ± 4.1 and there was no difference between men and women (p = 0.34).
There was no statistically significant difference between the level of injury and headache (p = 0.99). The occurrence of headache did not depend on the severity of the TSCI (p = 0.14).
Headache characteristics after traumatic spinal cord injury.

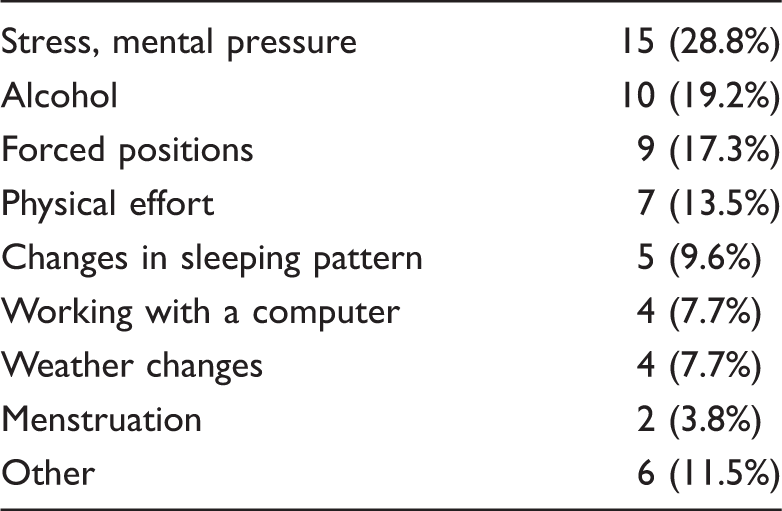
Provoking factors of headaches in patients with traumatic spinal cord injury.
Types of headache in patients with traumatic spinal cord injury.

The new headache was tension-type headache in eight patients (53.3%), migraine in six (40.0%) and other primary headache in one patient (6.7%). The mean duration between the TSCI and the first new headache attack was very variable, starting from an abrupt onset after the trauma and reaching up to five years after the event. However, most of the patients could not recall an exact time of the first attack after the TSCI (66.7%).
Abortive medications for headache were used in 48% of patients and ibuprofen was the most often used medication (28%). The majority of these individuals (64%) reported taking analgesics more than once per month.
Discussion
This study showed that headache after TSCI is the most frequent pain-related condition. In our study, approximately half of the patients reported having headache before TSCI, 71% of participants reported headache in the chronic phase after the TSCI. That is more frequent compared to the period before the injury.
Pain is one of the most frequent complaints after TSCI. The reported prevalence ranges from 19% to 96% (4,7–10). The authors of previously published reports discuss that heterogeneity of investigated cohorts or the pain determinants of the studies’ confounders represent certain difficulties in defining an exact pain prevalence (4).
In patients with TSCI, pain typically consists of many subtypes (2). To our knowledge, headaches after TSCI have never been explored in a systematic study. Possible reasons for that may be related to a general underestimation of the influence of headaches on patients’ quality of life, a lack of acknowledgment that headache can represent not only a rather harmless episode, but also a serious chronic condition that is underdiagnosed and often mismanaged. A further possible source of underestimation is related to a selected design of previous studies on pain after TSCI. Pain definition strictness determines the prevalence rates (4). When asked about chronic pain, headache might be excluded from the list, due to an attempt to find the most disturbing pain or determine the prevalence of pain. Such an example is the investigation published by Felix et al., who reported in their study that the head was the least frequent pain location (2.9%) compared to back (29.5%) (2). This particular study has several methodological limitations in terms of patient selection (inclusion criteria were defined by the authors as “individuals with traumatic SCI and chronic pain of more than 6 months duration” and the recruitment was advertisement based). This selection bias probably resulted in a marked underestimation of prevalence of headache in their sample. In addition it was not clear how “chronic head pain” was defined. The authors also did not look into the occurrence of episodic headache that can often be as debilitating as chronic headache, as it was out of the scope of their study. Hence, the strengths of our study are the absence of pre-selection, direct questioning of all participants and the use of internationally accepted classification of headache disorders for defining headaches in our group (6).
Almost half of the patients’ headache descriptions in our study matched with tension-type headache and one-third had signs of migraine. Taking into consideration the prevalence of primary headaches (11), migraine was more prevalent as a new headache after the trauma. Post-traumatic headache was not diagnosed in our sample although traumatic brain injury was documented in 15.5% of cases.
One may speculate that the major provoking factor for inducing headache after TSCI might be related to reduced physical activity, leading to muscle tensions, which are often associated with provoking headache. At the same time patients with TSCI are usually devastated psychologically and it is important not to ignore the psychological components that may influence pain behavior (8). The most frequent headache-provoking factors in our study turned out to be mental stress and alcohol. This is a practical finding giving physicians enough reason to emphasize these factors when dealing with persons with TSCI.
The only secondary headache that we could establish from the interview was headache attributed to AD. The headaches after TSCI can often be related to symptoms of AD. The AD reaction may cause life-threatening conditions like seizures, intracerebral or subarachnoidal hemorrhage or arrhythmias that ask for prompt relief of afferent stimulation causing the reaction (12–14). AD is a reaction all health professionals interacting with TSCI patients should be aware of, and they should ask the patient about the presenting symptoms.
Literature analyses in PubMed using the search phrase “headache and spinal cord injury” results mostly in articles related to AD. Headache attributed to AD after TSCI has been described as sudden onset, severe, accompanied by hypertension, flushing of skin above the level of injury or sweating above the injury (15). ICHD-3 beta defines headache attributed to AD as headache of sudden onset that develops in temporal relation to the rise of systolic blood pressure of ≥30 mmHg and/or diastolic pressure ≥ 20 mmHg. The headache is severe, usually of a pulsating quality, and it can be accompanied by cranial diaphoresis at the level of TSCI (6). The frequency of AD varies from 19% to 70% and is more frequent among individuals with cervical TSCI and complete spinal cord lesions (14). Headache as a symptom of AD is noted in more than half of these patients (12). AD occurs predominantly in patients with cervical or high thoracic TSCI (above Th6), and individuals with complete TSCI are at greater risk. Consistent with earlier studies, we found that 13% of our patients had headache attributed to AD. However, among at-risk populations with cervical or higher thoracic spinal cord injury, the prevalence was 19%. Stimuli (painful or non-painful) originating below the level of TSCI are the potential precipitators of an episode of AD. The list of provoking stimuli for AD is long: bladder distension, urinary tract infection, bowel distension, urologic procedures, gastric ulcers, pressure ulcers, ingrown toenail, burns, trauma or surgical procedures, etc. (15).
Although the majority of AD episodes are self-limited or asymptomatic, they can be life threatening. Therefore, greater awareness is crucial for early recognition and management of AD to prevent complications in people with TSCI.
About half of the patients in our study were using analgesics for headache. Taking analgesics against several pain types could increase the risk of medication-overuse headache (MOH). Unfortunately, we asked only about taking analgesics for headache and options were: none, less than one day per month, more than one day per month (Appendix 1). Therefore, it is impossible to draw inferences about the prevalence of MOH in our cohort.
Mechanisms that can lead to headache after TSCI are not well known but as chronic pain in general is a common problem after TSCI, headache probably involves similar changes. Several changes occur in the peripheral and central nervous system after TSCI (16). The probable explanation for the increased prevalence of headache after TSCI is that cephalic and generalized pain sensitivity may become abnormal after the injury (17,18). The patients’ pain threshold may be decreased, which can substantially increase the prevalence of headache. Also, as individuals with TSCI often overuse their muscles of the shoulder girdle, use poor seated posture, with the contribution of weakness and spasticity, their muscles’ metabolism is disturbed (1). This can sensitize nociceptive neurons, resulting in painful conditions not only in the muscle itself, but also in the head. Several aforementioned factors contribute to an increase in pericranial muscle activity, which is a suggested mechanism of episodic tension-type headache. In addition, central mechanisms are probably involved as well. It was shown that plastic and reorganizing brain changes do take place after TSCI, which has been demonstrated to be related to pain after TSCI (17,18).
One of the most troublesome findings of our study is that people in TSCI in Estonia have not contacted their physician with regard to their headaches. Only 15% of participants consulted a physician for their headache. This fact clearly represents the lack of knowledge about headaches, its burden and treatability within the population itself. Although it could be speculated that headache might not be a substantial problem for these patients, regarding the mean intensity of headache pain (NRS 6.9), it is unlikely. Hence the practical implication of this study is very clear: Every effort should be made not only to inform patients and raise the awareness within the health care system, but also to make active inquiries if patients with TSCI also have headaches.
The limitations of this study should also be considered. The retrospective design and methods used represent a risk of a recall bias, as many patients did not remember an exact onset of their headache or the characteristics of headaches. For instance, it may result in underestimation of post-traumatic headache because patients did not remember when the headache started, or lower prevalence of headache before the trauma for the same reason as the recall bias. Another limitation of the study is that we did not examine full comorbidity, including the psychiatric one. Therefore, headaches attributed to psychiatric disorder, including ones related to trauma, could not be diagnosed. The current study was specifically designed to investigate the prevalence of headache after TSCI, hence there is a possibility that other types of pain were less reported and therefore influenced the obtained results. Unfortunately we did not have a control group without TSCI in our study and there are no epidemiological headache-related data in Estonia, thus we cannot compare headache prevalence among TSCI patients with the general population. Relatively small sample size reduced the power and conclusiveness of some findings, bringing up the need for further studies, specifically looking into the topic of headaches’ occurrence after TSCI.
In summary, our study shows that headache is the most prevalent painful condition after TSCI. Despite this fact, headache is underdiagnosed and undertreated. There is a clear need to increase awareness at all levels in people with TSCI, and among all specialists who manage patients with TSCI, including primary care and neurorehabilitation doctors and last, but not least—headache specialists. Further studies are needed to provide evidence regarding not only the prevalence of headache, but its impact on quality of life of patients with TSCI.
Clinical implications
Headache is the most frequent pain-related condition after traumatic spinal cord injury. Headache is underdiagnosed and undertreated among patients with traumatic spinal cord injury. People who deal with patients after traumatic spinal cord injury should not forget to pay attention to headache that can represent a serious condition that decreases quality of life, or be a symptom of a life-threatening autonomic dysreflexia.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.