
Abstract
Objectives
This study explored the clinical characteristics of vestibular migraine in Chinese subjects and performed a field test of the criteria of the International Classification of Headache Disorders 3rd edition beta version.
Methods
Consecutive patients with vestibular migraine were surveyed and registered in a headache clinic during the study period. The diagnosis of vestibular migraine was made according to International Classification of Headache Disorders 3rd edition beta version. Assessments included standardized neuro-otology bedside examination, pure-tone audiogram, bithermal caloric testing, neurological imaging, cervical X-ray or magnetic resonance imaging, Doppler ultrasound of cerebral arteries and laboratory tests.
Results
A total of 67 patients (62 female/five male, 47.8 ± 10.3 years old) were enrolled in this study. The mean ages of migraine and vertigo onset were 32.2 ± 11.5 and 37.9 ± 10.1 years, respectively. The most common migraine subtype was migraine without aura (79%), followed by migraine with aura (12%) and chronic migraine (9%). The duration of vertigo attacks varied from seconds to days and 25% of patients had attacks that lasted less than 5 minutes. Among the patients with short-lasting attacks, 75% of these patients had ≥5 attacks per day within 72 hours. Auditory symptoms were reported in 36% of the patients. Migraine prophylactic treatments were effective in 77% of the patients.
Conclusions
Our study showed that the clinical features of vestibular migraine in China were similar to those of Western studies. The definition of vertigo episodes and migraine subtypes of vestibular migraine in International Classification of Headache Disorders 3rd edition beta version might be modified further. More than five vertigo attacks per day within 72 hours might be helpful as far as identifying vestibular migraine patients with short-lasting attacks.
Keywords
Introduction
Vestibular migraine (VM) is generally considered to be a primary headache syndrome that is characterized by episodic vertigo, onset during the third and sixth decade, predominantly in women, with or without auditory symptoms and responsive to migraine symptomatic and prophylactic treatment (1–3). VM is also known as ‘migraine-associated vertigo/dizziness’, ‘migraine-related vestibulopathy’ and ‘migrainous vertigo’ (4–6). A population-based study revealed that the lifetime prevalence of VM is 1%, which is the second most common cause of episodic vertigo after benign paroxysmal positional vertigo (BPPV) (4). However, most knowledge and understanding of VM comes from Western-based studies and the clinical features of VM in Asia are poorly understood.
The International Classification of Headache Disorders, 3rd edition beta version (ICHD-III beta) proposed the diagnostic criteria for VM (7) in 2013, but 30–50% of patients do not fulfil all of the criteria, such as the duration of vertigo attacks (1,4,8,9). Furthermore, standardized classifications of vestibular symptoms are essential to VM, which is based on a symptom-driven syndromic diagnosis. Therefore, it is important to field test the ICHD-III beta criteria.
We surveyed consecutive patients with VM in a headache clinic in China to explore the clinical characteristics of VM in Chinese patients and to field test the ICHD-III beta criteria.
Methods
We consecutively recruited all patients with headache and/or dizziness who were referred to the headache clinic of the First Affiliated Hospital of Chongqing Medical University during the study period (June 2013– December 2014). The local ethics board approved the study. All of the patients were informed about the purpose of the study and provided informed consent prior to participation.
The diagnosis of VM was based on ICHD-III beta (7) using a semi-structured face-to-face interview as described previously (10). Contrary to the ICHD-III beta criteria, vertigo duration was not necessarily confined between 5 minutes and 72 hours. Four neurologists (Y.X. Zhang, D.Y. Wang, J.J. Chen and L.X. Li) performed detailed interviews concerning vestibular features (type, duration, severity, etc.), shared triggers of migraine and VM, family history of migraine and chronic vertigo, associated migrainous and cochlear symptoms of each patient.
A neurologist (J.Y. Zhou) who specialized in neuro-otology performed standardized neuro-otology bedside examinations in all patients. Neuro-otology bedside examination consisted of eye movement, positional and balance tests. Eye movement tests included spontaneous nystagmus, gaze-evoked nystagmus in the horizontal and vertical plane, smooth pursuit, saccades and optokinetic nystagmus. Position tests included positional nystagmus in the Hallpike positions (the head is turned 45 ° to each side and moved backward) and left and right lateral supine positions. Balance tests included the Romberg test and tandem walk. Hearing was assessed in all patients using thumb-finger rubbing for each ear to screen for asymmetric hearing loss as described by Torres-Russotto et al. (11).
Pure-tone audiogram (PTA) and bithermal caloric testing were performed in 24 patients with cochlear complaints. Cerebral CT or magnetic resonance imaging (MRI) was performed in 32 patients. Cervical X-ray or MRI, Doppler ultrasound of cerebral arteries and laboratory tests, such as complete blood count, blood lipid levels and fasting blood sugar level, were also performed when appropriate.
Possible differential diagnoses were excluded, such as previous ear surgery, retrocochlear neoplasm, Ménières disease (MD), vestibular paroxysms, BPPV, autoimmune inner ear disease, otosclerosis, otosyphillis, posterior circulation stroke and transitory ischaemic attack.
A neurologist (J.Y. Zhou) in our headache clinic generally treated patients with VM empirically with flunarizine (5 mg per day), topiramate (75 mg per day) or amitriptyline (25–50 mg per day) based on the specialist's judgements and patient's preferences. Seven patients received lifestyle adaptations exclusively for the treatment of low frequency headaches and vertigo attacks (less than one episode per month). Response to medication was recorded using face-to-face or telephone interviews after a 1-month treatment period: significant remission (≥50% reduction in moderate to severe headache or vertigo days), partial response and no improvement or worsening symptoms.
The referral system in China is quite different from the USA, UK and Canada. Patients have complete freedom to choose hospitals and physicians, as in Taiwan (12), i.e. they can seek care at tertiary care institutions regardless of the nature or severity of their illness. Therefore, all of our patients were self-referred and clinical manifestations of only headache or dizziness or both symptoms existed in our clinic. Our headache clinic has been operating since 2009.
Statistical analysis was performed using the SPSS 19.0 software package (SPSS Inc., Chicago, IL, USA). We grouped patients into two categories according to different chief complaints: headache chief complaint group; dizziness chief complaint group. Continuous variables are presented as means ± SD and Student's t-test was used to assess differences between two groups. Categorical variables are presented as frequency distributions (N, %), and Chi-square or Fisher's exact test was performed where appropriate. All statistical tests were two-sided and statistical significance was defined as 0.05.
Results
A total of 1705 patients with headache and/or dizziness visited the headache clinic during the study period. From this population, 403 patients had a lifetime diagnosis of migraine according to the ICHD and 67 patients were newly diagnosed with VM (62 female/five male, 47.8 ± 10.3 years, range 23–67 years). Thirty-two (48%) patients cited headache as their chief complaint and the remaining 35 (52%) patients cited vertigo as their chief complaint.
Table 1 shows the onset age of migraine and vertigo attacks. The onset age of migraine peaked in the third decade and vertigo attacks peaked in the fourth decade (Figure 1). Migraine preceded the development of vertigo in 34 (51%) patients by an average of 6 years. Migraine and vertigo occurred simultaneously in 24 (36%) patients and the other nine (13%) patients had vertigo several years before migraine. Family history of migraine and recurrent vertigo with unknown causes in first-degree relatives was reported in 25 (37%) and 20 (30%) patients, respectively. Shared trigger factors of migraine headaches and vertigo attacks were reported in 32 (48%) patients and the most common factors were sleep disturbance (56%), cold (47%), fatigue (19%) and noise (19%).
The distribution of onset ages of migraine headaches and vertigo attacks in patients with vestibular migraine. Clinical characteristics of vestibular migraine in 67 patients. One patient with CM had visual aura for 1–2 days per month. bMore than one answer available.

Migraine subtypes
Fifty-three (79%) patients had migraine without aura (MO), eight (12%) patients had migraine with aura (MA) and six (9%) patients had chronic migraine (CM). All MA patients had visual aura. Table 1 summarizes the clinical characteristics of VM.
Clinical characteristics of six patients with chronic migraine.
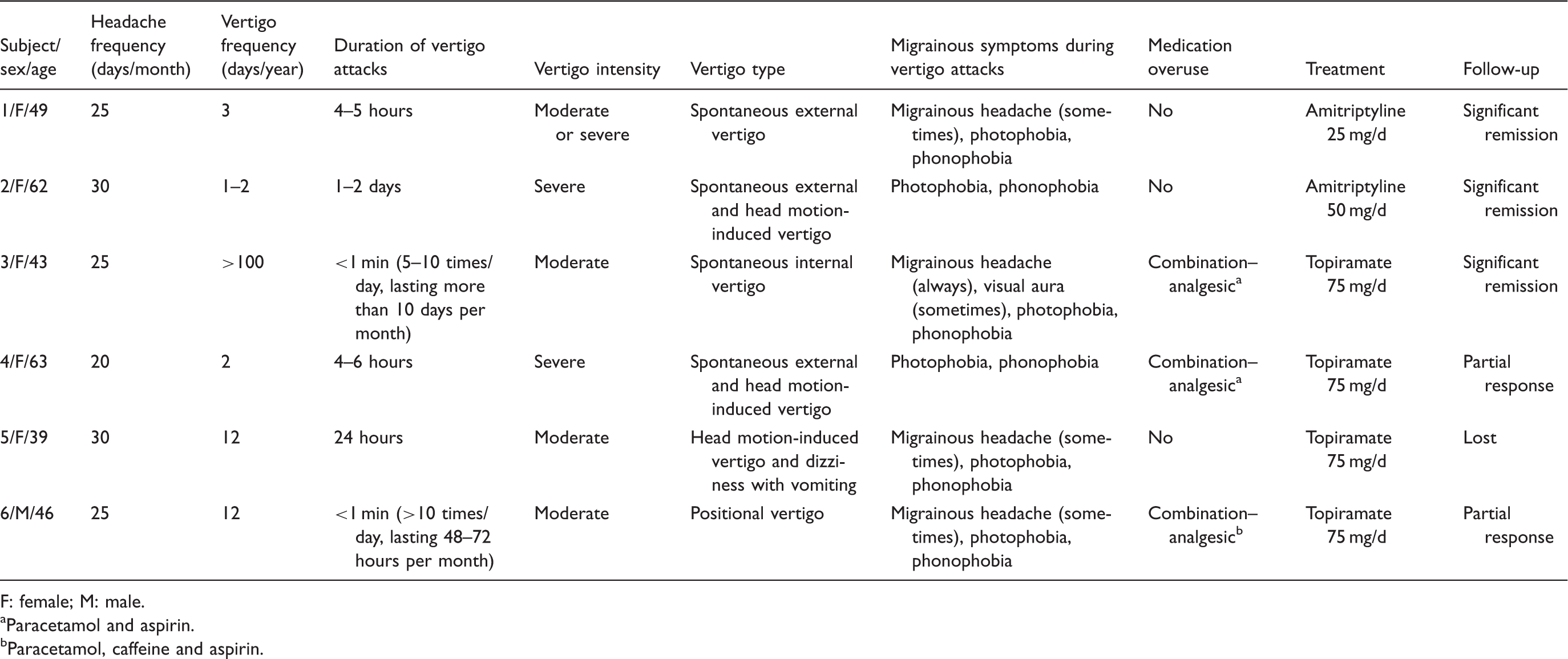
F: female; M: male.
Paracetamol and aspirin.
Paracetamol, caffeine and aspirin.
Clinical characteristics of vestibular symptoms
The most common type of vertigo was spontaneous vertigo (85%), followed by positional vertigo (18%). The duration of vertigo attacks was highly variable and ranged from several seconds to 5 days. Fifteen (22%) patients had vertigo episodes lasting 5–60 minutes. Eighteen (27%) patients had vertigo attacks in the range of 5 minutes to 72 hours (Figure 2). Twelve (18%) patients had pure positional or spontaneous vertigo attacks that lasted less than 5 minutes and nine of these 12 (75%) patients had recurrent (≥5 attacks per day) vertigo attacks within 72 hours. The remaining three patients had sporadic vertigo attacks.
Duration of vertigo attacks in patients with vestibular migraine.
Migrainous symptoms during vertigo attacks
Photophobia (87%) and phonophobia (85%) were the most frequently reported migrainous symptoms during vertigo, followed by headache (64%). Aura was reported in only nine (13%) patients and all of these patients had visual aura. The temporal association of migrainous headaches and vertigo attacks was highly variable. Vertigo attacks in 23 (34%) patients were always associated with migrainous headache. Migrainous headaches were associated with vertigo attacks occasionally in 20 (30%) patients and migrainous headaches never occurred with vertigo attacks in 24 (36%) patients. All patients avoided routine physical activities and head motions that might aggravate vestibular symptoms during symptomatic episodes.
Cochlear symptoms and audiometric findings
Cochlear symptoms were experienced in 10 (15%) of the 24 patients with cochlear complaints at the time of the episode. Only three patients had unilateral tinnitus and the rest of these patients had bilateral cochlear symptoms. Three of the patients who had sensorineural hearing loss had an MD-like vertigo and showed atypical hearing loss: symmetric, mild hearing loss with a down-sloping pattern that involved low frequencies (average hearing level at 0.5–3 kHz between 25 and 35 dB) and peaked at high frequencies. One patient had atypical MD-like vertigo: recurrent short spontaneous or positional vertigo. All patients had normal bilateral caloric responsiveness and canal paresis <24%. Therefore, VM was the likely diagnosis.
Treatment
Sixty-one patients received medications (flunarizine n = 46, amitriptyline n = 7 and topiramate n = 8). Ten patients (flunarizine n = 8, amitriptyline n = 1 and topiramate n = 1) were lost to follow-up during the initial 1-month treatment period and three patients discontinued flunarizine due to rash (n = 1) and drowsiness (n = 2). The other 48 patients were treated with flunarizine (n = 35), amitriptyline (n = 6) and topiramate (n = 7). Thirty-seven (77%) of these patients had significant remission, seven (15%) patients had a partial response and four (8%) patients had no improvement.
Field testing of the ICHD-III beta criteria
Diagnostic criteria of vestibular migraine in ICHD-III beta and the percentages of patients who fulfilled each criterion.
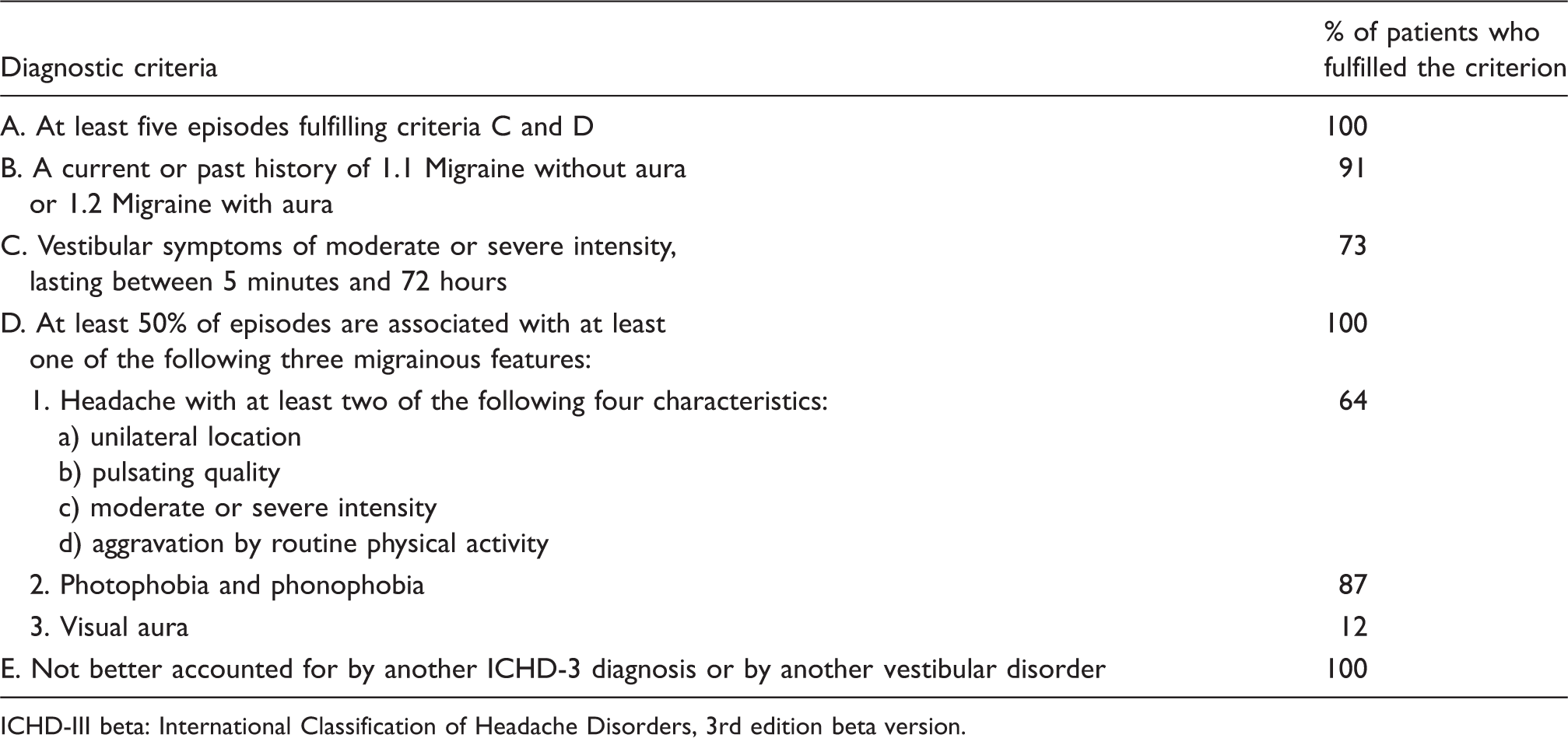
ICHD-III beta: International Classification of Headache Disorders, 3rd edition beta version.
Discussion
This study presented the first field testing of the ICHD-III beta for VM in China. The female predominance in this study was similar to that of previous studies (1,5,6,8). The peak onset age of migraine in patients with VM was older than that of patients in dizziness clinic-based studies in Germany (32 vs. 20 years old) (1,4,13). Vertigo attacks appeared on an average of 6 years after migraine in 51% of patients, which was consistent with previous studies (1,4).
Migraine syndromes in VM were restricted to MO and MA according to the ICHD-III beta, instead of migraine in the 2001 Neuhauser criteria (4). Six patients in this study had a current history of CM and three of these patients also fulfilled the criteria of medication over-use headache. Notably, CM was not considered to be a migraine complication (7) and CM might also be a migraine subtype of VM. Different VM treatments should be considered because CM is more debilitating than episodic migraine (14). The proportion of MA in this study was much lower than MO, which is unlike previous studies (1,9). Nevertheless, the ratio of MA to MO was approximately 1:10 (15–17) in our previous study and two population-based studies in China and Taiwan, which was significantly lower than in other regions (18–20). These differences may be caused by the different referral system in China and population settings. Further prospective studies that include a dizziness diary are recommended (21).
VM was definitively defined in 2001 (10), but the definitions of vestibular symptoms are diverse among clinical researchers (1,4,22). The collection of precise descriptions of the vestibular symptoms as defined in ICHD-III beta was a troublesome process (23) and all of the vestibular symptoms reported by our patients could be classified into the current categories, i.e. spontaneous, positional, head motion-induced and visual. Our patients did not report other types of vertigo. Spontaneous vertigo (including external and internal) was always well reported by patients, but head motion-induced dizziness with nausea was often confused with other non-specific dizziness, e.g. motion sickness. The most common vertigo type was spontaneous vertigo, followed by positional vertigo. This finding is similar to previous observations (1,8,9).
The duration of vestibular symptoms was highly variable and ranged from seconds to days. Twelve patients (18%) had pure short-lasting positional or spontaneous vertigo attacks and similar results were also reported in several dizziness clinic-based studies (1,4,6,13,24). Short-lasting vertigo attacks might be confused with BPPV. Note that episodes with recurrent vertigo attacks occurred within 72 hours in 75% of our patients, whereas the duration of BPPV generally lasted several weeks to months (25). Additionally, 2.7% of patients with positional vertigo in the dizziness clinic were actually VM patients (24). Therefore, recurrent short-lasting vertigo attacks within 72 hours and ≥5 attacks per day might be a helpful diagnostic criterion to distinguish BPPV and VM.
Twenty-three (34%) patients were referred to our clinic by a general physician, seven (10%) patients were referred by an otologist and 11 (16%) patients were referred by a neurologist. Unfortunately, none of these patients had been diagnosed with VM. The low diagnosis rate may reflect a lack of awareness of the symptoms of VM in China, similar to Germany (9). Another potential explanation for the low diagnosis rate is the coexistence of cochlear symptoms in VM. A survey of the members of the American Neurotology Society and the International Headache Society revealed that concomitant cochlear symptoms are one of the most challenging difficulties in the diagnosing of VM (26). Approximately one-third of our patients had cochlear symptoms and four of these patients had sensorineural hearing loss, which is consistent with previous observations (8,27). In contrast to MD (28,29), the cochlear symptoms in VM were not prominent and the sensorineural hearing loss was symmetric, mild and non-progressive, even after a median follow-up time of 9 years (8). Therefore, the coexistence of cochlear symptoms should not be used to exclude a diagnosis of VM.
Current knowledge of VM was primarily derived from dizziness clinic-based studies; 48% of our patients cited headache and 52% cited vertigo as their main reason for medical consultation because of the different referral system in China. Whether there are any differences between VM patients with different complaints is not known. All patients with CM in our study were in the headache chief complaint group. The headache group had significantly more headache days compared to the dizziness group (6.8 ± 9.2 vs. 1.4 ± 2.0 days; P = 0.001) and this figure remained significant after adjusting for CM (P = 0.013). The dizziness group had a slightly higher proportion of cochlear symptoms during episodes (26% vs. 3.1%; P = 0.032). There were no differences between these two groups in the associated migrainous symptoms, vertigo days or the response to medications.
Our study did not provide high level evidence for the treatment of VM, but it indicated that patients with VM benefited from an initial 1-month treatment period with prophylactic migraine medications.
There are some limitations to be considered. This study was a clinic-based study and the data could not be used to estimate the prevalence of VM in the general population. Many of our patients were in symptom-free episodes and the PTA may have missed subtle abnormalities during the acute phase. The nature of a retrospective study does not allow a precise aetiology of each vestibular symptom.
In summary, this study provided the clinical features and first field testing of VM in a headache clinic in China. VM in our study was a primary headache syndrome that was characterized by episodic vertigo lasting seconds to days, with an onset during the fourth decade of life and occurring predominantly in women. Auditory symptoms may occur, but these symptoms were not the chief complaints in VM. CM may also be a migraine subtype of VM according to the ICHD-III beta. The current classifications of vestibular symptoms were well organized when applied in clinical work. Short-lasting vertigo attacks (less than 5 minutes) were experienced in 25% of patients and most patients had core vertigo episodes within 72 hours. Migraine with aura in VM was rare in Chinese patients, and further studies using dizziness diaries should be considered.
Clinical implications
This research is of major importance for neurologists because vestibular migraine is a primary headache syndrome in headache clinics, and it is often misdiagnosed in China. This study details the clinical characteristics of VM in China. Our patients were different from Western studies in several aspects, including an older onset age and a lower proportion of MA. The definition of vertigo episodes and migraine subtypes of VM in the ICHD-III beta may be further modified. More than five vertigo attacks per day within 72 hours may be useful to identify VM patients with short-lasting attacks. Cochlear symptoms were reported in one-third of VM patients, and the sensorineural hearing loss was symmetric, mild and non-progressive. Therefore, the coexistence of cochlear symptoms should not be a reason to exclude VM.
Footnotes
Funding
This work was supported by the project of Chongqing Yuzhong District Science and Technology Commission [NO. 20120204], and the Natural Science Foundation Project of Chongqing Science and Technology Commission [NO. cstc2013jjB10009].
Conflict of interest
None declared.
Acknowledgements
Appreciation is expressed to the members of the headache clinic of The First Affiliated Hospital of Chongqing Medical University for their assistance in screening for eligible participants. The investigators also thank the subjects for their participation.