
Abstract
Introduction
To investigate tissue flow disturbance and hypoxia during migraine aura, we studied a case of familial hemiplegic migraine (FHM) using novel magnetic resonance imaging (MRI) techniques.
Case results
A 44-year-old male was admitted with suspected stroke because of confusion and aphasia. Initial gadolinium-based perfusion MRI showed a decrease in cerebral blood flow and an increase in capillary flow disturbances within the left hemisphere. Later during the prolonged aura phase, chemical exchange saturation transfer MRI indicated a drop in pH in the affected area. The patient was diagnosed with an R908Q mutation in the ATP1A2 gene causing FHM type 2.
Discussion
During prolonged aura in FHM, MRI shows reduced CBF, capillary flow disturbances and a possible pH drop that could indicate tissue hypoxia.
Keywords
Introduction
In classical migraine with aura, aura symptoms as propagating homonymous visual disturbances are followed by severe headache. The underlying physiological substrate of the aura symptoms remains poorly understood. Cerebral blood flow (CBF) is reduced during migraine aura (1), but CBF seemingly remains above accepted thresholds of ischemia (2). Nevertheless, imaging studies in migraineurs have revealed increased lactate levels (3), consistent with tissue hypoxia.
We recently pointed out that capillary flow disturbances may give rise to tissue hypoxia in the absence of “classical” ischemia by allowing a critical proportion of inflowing oxygenated blood to pass through the tissue at transit times that are too short to permit efficient extraction of its oxygen (4). Glucose is predicted to be less affected by this “physiological shunt” phenomenon than oxygen, favoring the production of lactate as a source of adenosine triphosphate (ATP), although CBF may be only moderately reduced. We have therefore hypothesized that migraine aura may cause severe metabolic disturbances despite inconspicuous CBF reductions.
Here, we test this hypothesis using gadolinium-based perfusion magnetic resonance imaging (MRI) and chemical exchange saturation transfer (CEST) MRI to detect capillary transit time heterogeneity (CTH), CBF, and changes in pH in a patient with extended aura symptoms due to an inherited form of hemiplegic migraine (familial hemiplegic migraine (FHM)).
Patient and methods
Case
A 44-year-old right-handed male presented with confusion and suspected stroke. On admission, he complained of headache, nausea, and photophobia, and the initial neurological evaluation revealed aphasia, but no motor or sensory disturbances. MRI was acquired between one and a half and four hours after symptom onset (exact onset time uncertain). T2-fluid-attenuated inversion recovery (FLAIR) and diffusion-weighted imaging (DWI) showed no signs of acute ischemia but only nonspecific white matter lesions. No acute angiogram was acquired, but perfusion MRI showed hypoperfusion in the left hemisphere. Based on the history and MRI, stroke was ruled out and no thrombolysis was given. Later the same day the patient developed a fever (38.0℃) and encephalitis was suspected. Because of ongoing clopidogrel treatment, no lumbar tap was performed and the patient was treated with a combination of acyclovir and ceftriaxone as a precaution. Next morning, the patient was still confused, had developed right-hand paresis and replied with “yes” and “no” only.
Symptoms persisted, and on day 7 he developed focal seizures that evolved into a generalized seizure and was treated with sodium valproate. On day 12, a second MRI was performed, including CEST imaging, a novel noninvasive technique sensitive to pH changes. Motor function slowly recovered and was found normal on day 9 after symptom onset. On day 23 the patient was discharged to a local inpatient neurorehabilitation hospital because of persistent aphasia. Four months later the patient was seen in the outpatient clinic and showed an improvement in speech but persisting memory and concentration problems. Twenty months after discharge, a follow-up MRI including CEST was performed.
Five years prior to admission the patient had a similar episode with fever, and confusion progressing to somnolence lasting several days. The patient was admitted and encephalitis was suspected; however, a lumbar tab showed normal cerebrospinal white cell count and no viral or bacterial infection could be found. Moreover, the patient had suffered from several shorter-lasting episodes with sensory disturbances in the arm and/or leg occasionally in combination with motor deficits; these episodes were initially suspected to be of vascular origin and the patient was treated with clopidogrel. Retrospectively these episodes were suspected to be aura symptoms and the clopidogrel treatment was stopped.
Family history and genetics
The patient’s daughter had been admitted at the age of 13 for headache and hemiparesis. Patient and daughter were later diagnosed with an R908Q mutation in the ATP1A2 gene, which is related to hemiplegic migraine. Mutations in the ATP1A2 gene affect the alpha-2 isoform of the Na+/K+-ATPase (sodium pump), which is primarily localized in astrocytes. ATP1A2 mutations have been shown to reduce Na+/K+-ATPase activity (5), and heterozygous ATP1A2-mutation mice have a lower threshold for induction of cortical spreading depression (CSD) and faster subsequent spread of CSD. These findings may be related to impaired glutamate clearance from the extracellular fluid and/or elevated extracellular potassium concentrations due to sodium pump failure.
Based on the history, clinical work-up, and genetic test, the patient fulfilled the International Classification of Headache Disorders, third edition (ICHD-3) criteria for hemiplegic migraine. However, as no spinal tap or angiogram was performed during the described episode, other causes such as stroke or infection cannot be totally ruled out.
MRI
MRI was performed on a clinical 3T Philips® Achieva 3TX system. The patient was scanned at admission using our standard acute imaging protocol for suspected stroke, which includes the following sequences: DWI, T2 FLAIR, T2*, and dynamic susceptibility-contrast (DSC) perfusion imaging (6).
Amide proton transfer (APT) CEST MRI was performed as described previously(6). APT/CEST is a noninvasive MRI technique sensitized to the base-catalyzed proton exchange rate between protein-bound amide groups and water (7). This exchange rate is sensitive to pH, and the method therefore provides a noninvasive contrast that is sensitive to tissue acidosis.
Image and data analysis
Post-processing of the DSC, DWI and CEST APT data was performed using in-house modules run in SPM8 (Statistical Parametric Mapping, Wellcome Trust Centre for NeuroImaging, Institute of Neurology, University College London, UK) and MatLab (MathWorks, Natick, MA, USA). Perfusion data were analyzed by a parametric approach (8) that estimates the distribution of capillary transit times in each image voxel, and determines the mean and standard deviation of these distribution in the form of parametric means transit time (MTT) and CTH maps, respectively (9). Averaged DWI images and grayscale apparent diffusion coefficient (ADC) maps were generated from the DWI data to assess cytotoxic and vasogenic edema.
CEST
CEST data were analyzed using the asymmetry approach in which the APT-induced dip at +3.5 ppm from the water resonance is compared to the signal intensity at the opposite side of the water peak (e.g. −3.5 ppm) (10). As water/amide proton exchange rates are base-catalyzed over a physiological range, in ischemia expected acidosis leads to a reduced exchange rate and the water signal measured at +3.5 ppm (S+3.5) is attenuated (e.g. higher asymmetry: S−3.5–S+3.5). It should also be noted that such APT CEST effects are highest in white matter, as exchange is more favorable between amides on the peptide backbone and extracellular water in white matter than in gray matter, and also the concentration of myelin-based proteins is high in white matter.
Results
MRI at admission showed no signal changes on T2-FLAIR and no diffusion restriction on maps of ADC. Most of the left hemisphere was, however, hypoperfused, illustrated by prolonged MTT and increased CTH on DSC perfusion images (Figure 1(a) and (b)).
Acute perfusion-based MRI shows a left hemisphere increase in mean transit time (a) indicating a decrease in cerebral blood flow (CBF) and an increase in capillary flow heterogeneity (b) in the same area leading to an effective shunting of blood. MRI performed at day 12 shows cortical gray matter edema on T2-FLAIR (c) and DWI (d). MRI: magnetic resonance imaging; FLAIR: fluid-attenuated inversion recovery; DWI: diffusion-weighted imaging.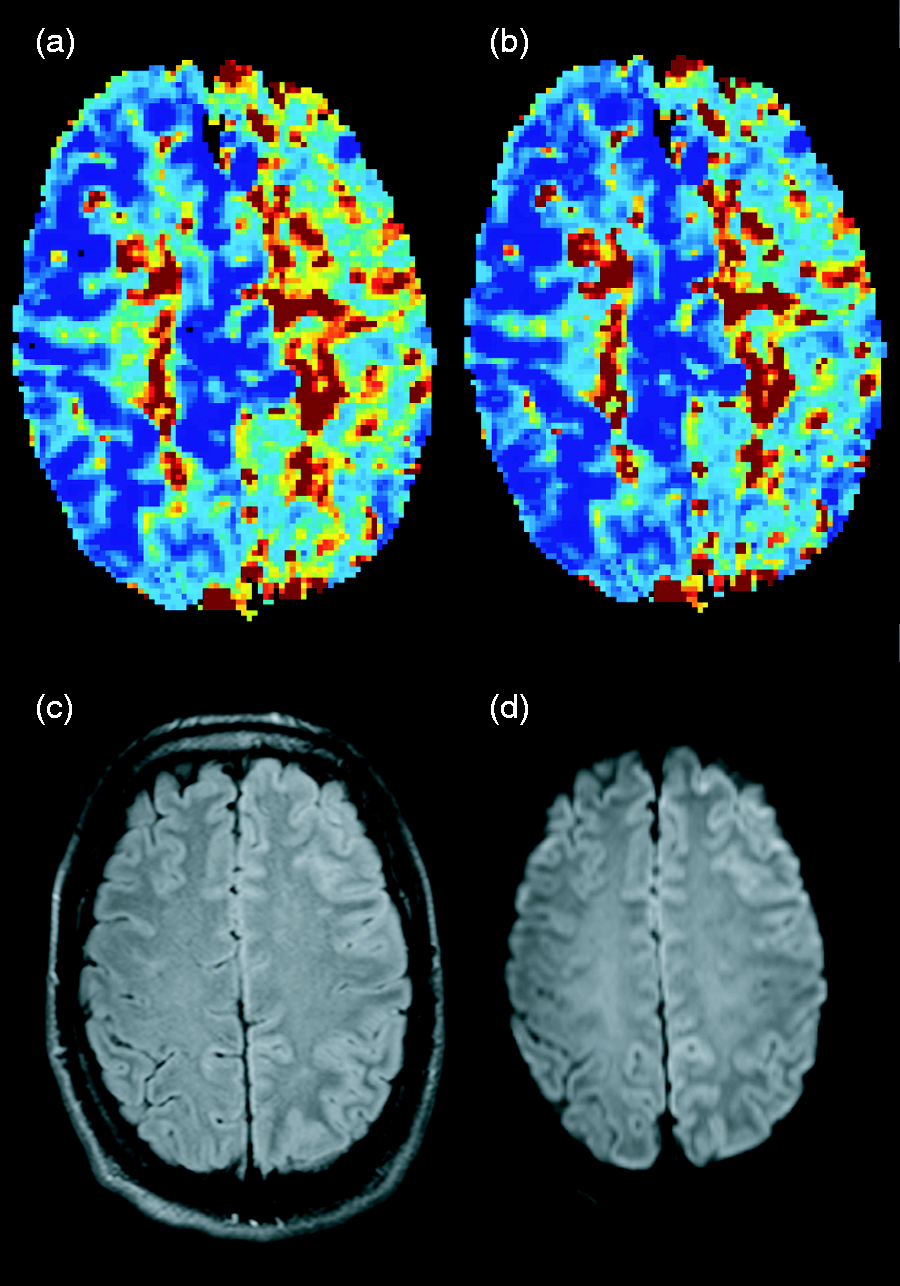
The second MRI on day 12, during the persistent aura period, demonstrated hyperintense cortical gray matter on T2-FLAIR and DWI images in most of the left frontal and parietal lobes, possibly reflecting vasogenic cortical edema (Figure 1(c) and (d)) as ADC maps showed no hypointensity as would be expected in cytotoxic edema. The APT-asymmetry images showed at this point a clear signal increase consistent with a pH drop in the white matter of the left frontal and parietal lobe (Figure 2(a)). These regions had been affected by hypoperfusion on the initial MRI 12 days earlier. At the 20-month follow-up the observed changes on the APT maps (Figure 2(b)) and the cortical edema had normalized and no new stroke lesion was present.
Chemical exchange saturation transfer MRI shows a possible decrease in pH within the left hemisphere during the aura (a). The observed abnormality normalizes at the final follow-up (b).
Discussion
This study used multimodal MRI to investigate changes in cerebral perfusion and pH during the prolonged hemiplegic aura in a patient with FHM2. MRI CEST/APT imaging 12 days after onset of symptoms showed changes consistent with tissue acidosis in the affected hemisphere despite the absence of ischemia on previous MRI. Possibly the initial widespread perfusion abnormalities are caused by CSD propagating through the gray matter. That tissue metabolism is compromised by the combination of low flow and capillary flow disturbances is supported by the increase in APT/CEST signal. The observed increase in APT-asymmetry intensity (Figure 2(a)) points to a decrease in pH giving rise to a decrease in exchange of amide protons.
As none of the MRI techniques are directly sensitive to CSD, it is unknown whether the prolonged aura is due to a persistent cortical depression, re-entry of subsequent waves of CSD, or is unrelated to CSD altogether. From the CEST images the pH changes seems localized to white matter, which is somewhat surprising since CSD spreads in the gray matter. This could be due to a limitation of the technique as the APT CEST effect is inherently highest in the white matter. Moreover, voxels localized in gray matter will tend to suffer from a partial volume effect with CSF lowering the sensitivity of the technique. Thus the lack of visible CEST/APT changes in gray matter does not rule out a pH drop in the area.
In conclusion, combined CTH and CEST/APT imaging revealed changes consistent with tissue hypoxia caused by capillary flow disturbances in a patient with prolonged FHM. In addition to reduced pH the observed CEST/APT changes could be affected by changes in tissue water, protein content or magnetization transfer effects (11,12). It should be noted that the perfusion and metabolic images were collected 12 days apart. The apparent drop in pH could be caused by the intermittent seizure or cortical edema. Nevertheless, CTH and CEST imaging in sporadic or familial migraine may help elucidate the origin of aura symptoms during CSD in migraine and related conditions.
Article highlights
Gadolinium-based perfusion magnetic resonance imaging (MRI) shows capillary flow disturbances during aura in familial hemiplegic migraine. During prolonged aura in familial hemiplegic migraine, chemical exchange saturation transfer MRI indicates tissue acidosis in the affected hemisphere.
Footnotes
Funding
This work was supported by the Danish Ministry of Science, Technology and Innovation’s University Investment Grant MINDLab (JUB and LØ).
Conflict of interest
None declared.