
Abstract
Following the recent discovery of neural calcium channel mutations in familial hemiplegic migraine, genetic linkage and association studies have been performed world-wide in an effort to unveil the genetic basis of the more common types of migraine too. Mutations in neural calcium channels, rnitochondrial DNA, serotonin receptors and transporter, dopamine receptors and genetic prothrombotic risk factors have been especially investigated and are discussed here. No unambiguous conclusions have, however, been reached. FHM remains an isolated success story in the quest for the genetic basis of migraine.
Introduction
That migraine has a genetic basis is an ancient view, but hard to substantiate due to migraine's wide prevalence, its variable symptoms and disease course, and the lack of laboratory markers and appropriate animal models. Several genetic epidemiological and segregation studies confirm, however, that migraines carry a significant hereditary risk (1–9). Migraine is now usually viewed as a polygenic multifactorial disease, having, that is, both environmental and genetic causative factors, with multiple genes involved and interacting. Other disorders with a high prevalence in the general population, such as diabetes mellitus, blood hypertension, mental illness, etc. are also considered multifactorial diseases, not conforming to the usual models of simple trait mendelian transmission. The multifactorial model itself, however, is not yet validated for migraine and FHM, a subtype of migraine with aura (MA) does conform to simple mendelian autosomal dominant transmission.
We examine here the recent findings obtained with the help of molecular biology techniques, which in our case include linkage and association studies and the cloning and sequencing of candidate genes for pathogenic mutations.
Linkage studies are powerful tools for tracking genetic traits due to single mendelian genes, but remain less effective when dealing with a multifactorial disease. In fact, they have proved useful in the identification of the genes responsible for FHM which is transmitted as a single trait disease, and which has now been transformed into the standard model for migraine pathogenesis. Association studies, which examine the preferential segregation of specific alleles of genetic markers with known genomic localization in ‘migraineurs’ against controls, are increasingly popular in migraine, but have not yet led to firm and unequivocal conclusions. FHM remains an isolated success story among the various migraine types, the only one for which the actual gene and mutations involved are known.
Familial hemiplegic migraine
Familial hemiplegic migraine (FHM) is classified within migraine with aura (MA) (10), and its genetic transmission is known to be autosomal dominant. While studying cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIIL), Joutel et al. (11) mapped FHM to the short arm of chromosome 19 within a 30-cm interval. The idea that CADASIL and FHM could be allelic disorders was soon dispelled (12, 13) and it became apparent that even FHM, a rare disease in itself, was heterogeneous, since only four out of nine families tested linked to chromosome 19 (14). The genetic heterogeneity of FHM was confirmed by Ophoff et al. (15) in five pedigrees, three of which only linked to chromosome 19. Interestingly, cerebellar ataxia and nystagmus were found in FHM pedigrees linking to chromosome 19. Penetrance in these families was incomplete, estimated at 80–90%; monozygotic twins could be discordant for the disease (16).
In 1996 it was recognized that FHM was caused by mutations in the calcium channel gene CACNL1A4 (later renamed CACNA1A), and that FHM was a disorder allelic to episodic ataxia type 2 (EA2, see later) (17). CACNA1A, the alpha 1 subunit gene of a neural P/Q type Ca2 + channel, locates to chromosome 19p13, and is composed of 47 exons covering 300 kb. This alpha 1 subunit forms the pore of the calcium channel. Ophoff et al. (17) described four different missense mutations R192Q, T666M, V714A and 11811L in FHM. More recently, several other missense mutations in CACNA1A have been reported, some of them associated with cerebellar ataxia (18–22, see Table 1); de novo missense mutations in the CACNA1A, Y1384C and T666M have also been observed in two sporadic cases with FHM and cerebellar ataxia (18, 23).
Familial hemiplegic migraine. Genotype-phenotype correlations

0 = absent
+ = present
All of these mutations mainly affect the pore or the voltage sensor parts of the ion channel. Interesting additional features observed were that mutation D715E was associated with essential tremor recurring in the FHM affected family, and that R1667W could be associated or not to progressive cerebellar ataxia. The most prevalent mutations are T666M and R583Q; T666M alone accounts for 50% of the families with FHM and ataxia (18, 20).
FHM remains, however, genetically heterogeneous. Recently, Gardner et al. (24) established linkage on chromosome 1q31 in a four-generation German-American family with FHM, and Ducros et al. (25) established linkage to chromosome 1q21–23 in three families previously shown to be unlinked to chromosome 19. Later on, in the same family, Gardner et al. (26) established linkage also to a second more proximal region, 1q21–23, with the two regions, 1q31 and 1q21–23 separated by a region of non-linkage, suggesting that two separate genes may be responsible for FHM in this one family (so-called two-locus model). The CACNL1A6 calcium channel gene, a candidate gene for FHM, lies in the non-linked region in this family. Moreover, since only three out of seven families investigated by Ducros et al. (25) linked to chromosome 1, there is evidence for at least two more genes beside CACNA1IA being responsible for FHM.
Subsequent molecular genetic studies have addressed three main questions:
Does the phenotype of FHM linked to chromosome 19 (chromosome 19-linked FHM, FHM 19) differ from FHM linked to chromosome 1 (chromosome 1-linked FHM, FHM 1)?
Do the different FHM mutations in CACNA1A display similar or varying clinical features?
How do CACNA1A mutations modify the bio-physical characteristics of the channel?
Genotype-phenotype correlations in FHM19 and FHM1 show that the two conditions vary somewhat. Terwindt et al. (27) did not find any difference as to age of onset, frequency and duration of the attacks, and duration of hemiplegia during the attack, in 46 patients belonging to three FHM19 families vs. 20 patients of FHM unlinked to chromosome 19. Coma during the attack and the triggering by even trivial trauma were, however, more frequent in FHM19. Cerebellar ataxia was found only in FHM19, while benign infantile convulsions were found in one family unlinked to chromosome 19. Ducros et al. (28) studied 10 FHM19 (94 patients) and three FHM1 (24 patients) families, finding a high degree of intra- and interfamily variability, but permanent cerebellar symptoms only in 50% of the FHM19, and a lower penetrance in the FHM1 families. In five patients of FHM1 families, moreover, epileptic seizures occurred during the FHM attacks. More recently still (20), essential tremor has been added to the clinical features encompassed within the spectrum of FHM19(see above). It is at this moment evident therefore that cerebellar signs, including essential tremor, localize FHM to chromosome 19, whereas epilepsy and febrile convulsions localize to chromosome 1.
The different CACNA1A mutations responsible for FHM have, moreover, variable clinical expression (Table 1). In fact, Terwindt et al. (29) found cerebellar ataxia only in two FHM19 families harbouring the 11811LCACNA1A mutation (intragenic CAG expansions were absent), whereas ataxia remained absent in a family with the V714A mutation. Ducros et al. (18) found progressive cerebellar ataxia in FHM19 families harbouring the T666M and a new D715E mutation. The reasons for this variability remain obscure, but it appears that cerebellar ataxia in FHM is linked only to some CACNA1A mutations, which must therefore have peculiar pathophysiological mechanisms.
Finally, the mutated ion channel does display abnormal biophysical characteristics. Kraus et al. (30) introduced the four original human FHM19 mutations into the corresponding alpha 1 subunit of the rabbit calcium channel and studied the kinetics of the channels expressed in Xenopus oocytes. Three (T666M, V714A and I1819L) of the four mutations, all localized at the putative channel pore, modified the inactivation gating characteristics of the channel. This altered gating could be responsible for abnormal neuronal excitability in FHM. Hans et al. (31) introduced four FHM missense mutations into human alpha 1 subunits and studied the functional channels after expression in embryonic kidney cells. All four mutations altered the biophysical properties of the channels and their density, but in different ways: while R192Q increased density and open probability, T666M decreased both density and conductance of the channels. V714A and I1815L behaved still differently, indicating that these FHM missense mutations may result in both loss- and gain-of-function of the calcium channel, with different pathophysiological implications and disease mechanisms.
The functional consequences of the CACNA1A mutations may be, however, even more complicated. This P/Q calcium channel is expressed mainly in presynaptic endings in the cerebellum and brainstem (and also at the neuromuscular junction), and its function is consistently modulated by interaction with other receptors, regulatory proteins (32) and neurotransmitters such as serotonin (33). Precisely how these interactions and how abnormalities in neuronal calcium traffic trigger the metabolic cascade responsible for FHM remains unclear. Conceivably, abnormal neuronal excitability could trigger the sustained depolarization responsible for spreading depression, and abnormal Ca2+ entry could ultimately result in mitochondrial Ca2+ accumulation, energy failure and final neuronal cell death, apparent as cerebellar atrophy. Finally, it must be remarked that the animal version of FHM may exist: mutations in the mouse equivalent of CACNA1A are found in the ‘tottering’ and ‘leaner’ mouse, characterized by a phenotype of ataxia and seizures (34), and altered calcium channel currents are displayed by Purkinje cells of the ‘leaner’ mouse (35). Mice cannot complain of migraine, but this interesting animal model lends credit to Terwindt et al.'s contention (36) that migraine, ataxia and epilepsy may all represent a spectrum of calcium channellopathies.
Episodic ataxia type 2 and spino-cerebellar ataxia type 6 (SCA-6).
In EA-2, two different mutations both disrupting the reading frame of the gene were originally reported by Ophoff et al. (17). Other mutations have since been reported in EA-2 (37). Later on, expansions of the CAG repeat at the 3' terminus of the CACNA1A gene resulting in truncated protein were found in pedigrees with autosomal dominant SCA-6 (38). The three pathological conditions, FHM19, EA-2 and SCA-6 all therefore represent allelic channellopathies due to different CACNA1A mutations. While FHM19 and FHM1 differ somewhat in their phenotype, clinical overlap among the three allelic CACNA1A channellopathies is increasingly evident. At first, missense mutations seemed to account for FHM19, protein truncation because of frame shift or abnormal splicing for EA2, and because of CAG repeats for SCA6 (39). In effect, six of seven new mutations reported in 10 familial and 14 sporadic EA2 cases (37) predict truncated or aberrant proteins, seemingly indicating that EA2 mutations are specific.
However, Yue et al. (40) in 28 probands with the EA2 phenotype discovered four new point mutations, only three predicting a truncated protein, and two new CAG 22-repeat expansions, concluding that EA2 results from both point missense and CAG expansion mutations; three families with SCA6 with CAG repeats had central positional nystagmus and episodic ataxia responsive to acetazolamide, features of EA2 (41), and downbeat nystagmus, typical of EA2, was the predominant clinical feature of SCA6 too (42); progressive ataxia of the SCA6 type was shown in a family with a new CACNA1A 1152np point mutation but without any CAG repeat (43); in a family with 23 CAG repeats in the CACNA1A gene, the phenotype varied from episodic to progressive ataxia, and in another with intergenerational allele size change, a 20 CAG repeat (expansion in the intermediate range) was associated with episodic, while a 25 CAG repeat was associated with progressive ataxia phenotype (44). Therefore, EA2 and SCA6 may blur into the same disease, with different phenotypes related to polyglutamine repeats of different (and varying through the generations) length and to different point mutations.
Finally, in one family with EA2 and a truncating R1547X mutation, two out of 14 carriers had clinical features of recurring hemiplegia, indicating some degree of overlap also between FHM and EA2 (45). Moreover, even though until now only point mutations seem to account for IFHM, progressive cerebellar ataxia and cerebellar atrophy are recognized features of FHM19, seemingly connecting FHM and SCA6. The clinical features of FHM, SCA6 and EA2 do therefore overlap. The full expression of these three allelic diseases shall be better appreciated only when pedigrees with distinct mutations are analysed in detail.
Migraine as a channellopathy
The successful unravelling of the genetics of FHM has naturally led to the proposition that the FHM19 locus might be involved in the pathogenesis of the more common forms of migraine.
This was suggested by the fact that obligate carriers in FHM19, or carriers of the FHM mutations themselves, manifested MA or migraine without aura (MO) but no hemiplegic features (reduced penetrance). Hovatta et al. were the first (46) to examine this hypothesis by means of linkage studies in four Finnish families with MA and/or MO. They obtained negative lod scores with markers for a region of 50 cM flanking the FHM locus on chromosome 19, thus excluding it as a site of migraine in their genetically isolated population. May et al. (47) tested the transmission of the highly informative marker D19S394, very close in terms of genetic distance to the FHM locus, in 28 families with MA or MO. Though linkage was not significant, sibling-pair analysis showed that affected siblings shared the same marker allele more frequently than chance; this led to the conclusion that the FHM locus on 19p13 is implicated in the more common forms of migraine.
Nyholt et al. (48) also found positive linkage lod scores, cosegregation and excessive allele sharing for markers in or around the FHM19 locus (a 12.6 cM region) in a large family with typical migraine (though not in the other three families examined), concluding that mutations in or around this locus were involved. These conclusions were amplified in the concept of migraine as a channellopathy (49). This concept, which derives from the striking advances made by means of molecular genetic studies of the periodic paralyses and episodic ataxias, is particularly attractive in migraine, in that it represents migraine as a disease of neural excitability with a threshold for the triggering of the attacks, a concept for which there is clinical and electrophysiological evidence (50), and which may explain the comorbidity of migraine with epilepsy and the episodic ataxias in man and animals (36).
Other studies contradict, however, a widespread role of the CACNA1A in the causation of common migraine. We could not find evidence of a positive linkage to CACNA1A in 14 Italian families with typical migraine (51) and the CACNA1A mutations responsible for FHM were not found by us in 12 familial cases with MA and 15 with migraine stroke (52). Likewise, Kim et al. (53) sequenced the entire 47 exons (and adjacent introns) of the CACNA1A gene in nine propositi of families with autosomal dominant transmission of migraine and episodic vertigo, selected because of the clinical resemblance with FHM and episodic ataxia, but found no mutation. The role of the CACNA1A gene in the causation of the more common migraine types thus remains unsettled. Until now, no family with non-hemiplegic migraine has been reported to harbour the CACNA1A FHM19 or other mutations. This speaks against a widespread involvement of this gene in typical migraine. Migraine, however, is likely to be genetically heterogeneous, and more studies in different families and populations are required for a definite conclusion.
The involvement of the FHM locus on chromosome 1 remains untested. We excluded linkage to CACNLB1, the gene for the betal subunit of the P/Q type Ca2+ channel in our pedigrees with MA and MO (51), and to sodium SCNA1, SCNA2, SCNA3 and SCNA6, potassium KCNA5 and KCNA6, and calcium CACNL1A1 ion channels genes located on chromosomes 2 and 12 (54).
Migraine as a disorder of mitochondrial function
Migraine with aura and migraine stroke are recognized features of the so-called mitochondrial encephalomyopathy, lactic acidosis and stroke-like (MELAS) syndrome (55), due to point mutations at codons 3243, 3271, 3252 and others of the mitochondrial DNA (mtDNA). Altered respiratory chain enzymatic activity and abnormal phosphorous magnetic resonance spectroscopy studies of energy metabolism, led to the hypothesis that a dysfunction of mitochondrial oxidative metabolism could underlie the common migraine types too (56). Mochi et al. apparently excluded that the mtDNA could be involved, since their segregation analysis did not support a maternal cytoplasmatic inheritance pattern in migraine (5). Other steps in mitochondrial function could, however, be involved, since mtDNA codes for only 13 mitochondrial proteins, and mtDNA may exert modifying influences on the phenotype.
Several searches have nonetheless been made for mtDNA mutations in migraine, usually with negative results, even in families of migraine transmitted according to a pattern compatible with maternal inheritance (see Table 2). Likewise several positive findings have been subsequently disproved. MtDNA studies suffer from a recognized difficulty, e.g. the variable degree of mutated mtDNA genome in different tissues of the organism (degree of heteroplasmy), and the relative inaccessibility of nervous tissue for analysis in migraine. MtDNA mutations may in fact be absent in the blood, but present in muscle or brain, or be present early on and then tend to disappear with age, as in the case of the Pearson and MELAS mutations. However, Ojaimi et al. (64), while confirming the absence of the MELAS, MERRF and Leber hereditary optic neuropathy (LHON) mutations in their patients with MA or juvenile stroke, found that the 4216 and 13708 mtDNA mutations, both secondary (that is having an adjunctive pathogenic role) mutations in LHON, were more frequent among patients below 35 years of age or with juvenile stroke, and hypothesized that accumulation of so-called ‘minor’ mtDNA mutations could contribute to the pathogenesis of migraine and in particular of stroke in young age.
mtDNA studies in Migraine

A thread towards a role of mtDNA in the pathogenesis of the migraine stroke was also suggested by Majamaa et al. (61). They had previously found the MELAS mutation in 6% of their patients with juvenile occipital migraine stroke (65). They went on to analyse 29 juvenile patients with occipital stroke, in 18 associated with migraine and in six due to migraine stroke, and excluded the 8344, 8993, 11778 and the common mtDNA deletion in this material. However, analysis of the mitochondrial haplotypes showed that 83% of the migraine stroke patients had the U mtDNA haplotype (as defined by the 12308 np polymorphism), a higher proportion than the control Finnish (17%, P < 0.002), general migraine (25%, P < 0.04) and migraine without stroke populations (19%). They concluded that the U mtDNA haplotype is a risk factor for migraine stroke. MTDNA haplotypes (there are nine recognized among Europeans) are normal population polymorphisms, mainly used in genetic population studies, but they do seem to induce some non-pathological variations in mitochondrial function. They could exert a modifying influence on the phenotypic expression of some mtDNA or genomic mutations.
Finally, Ohno et al. (66) reported two mtDNA point mutations, in the tRNAGlu and 12S rRNA, in a 14-year-old patient with matrilinear three-generational FHM. Out of 46 patients examined, these same mutations were present only in a LHON patient also suffering from MO. The authors speculated that these mtDNA mutations could contribute to the pathogenesis of migraine, but, as they themselves admitted, a larger population of migraineurs must be analysed before reaching any serious conclusion. It is also of note that an mtDNA deletion was found by us in a case with migraine stroke (62) and an 8.1 Kb mtDNA deletion in cyclic vomiting syndrome, considered a migraine equivalent (69).
Migraine as a disorder of serotonin metabolism
The development of the serotonin(5-HT) hypothesis and the recent introduction into the therapeutic armamentarium of the several tryptan compounds acting preferentially at the 5-HT receptors have made the latter ideal candidate genes in the pathogenesis of migraine, though with little success so far. Linkage and association studies of the 5-HT2A, 5-HT2C, 5-HT1D, 5HT1B have in fact been uniformely negative (51, 70–72). Likewise, there is no relation between allelic distribution at the 5-HT1B and 5-HT1F receptor genes and therapeutic responses to sumatriptan (73, 74) (Table 3).
Serotonin receptor genes and migraine
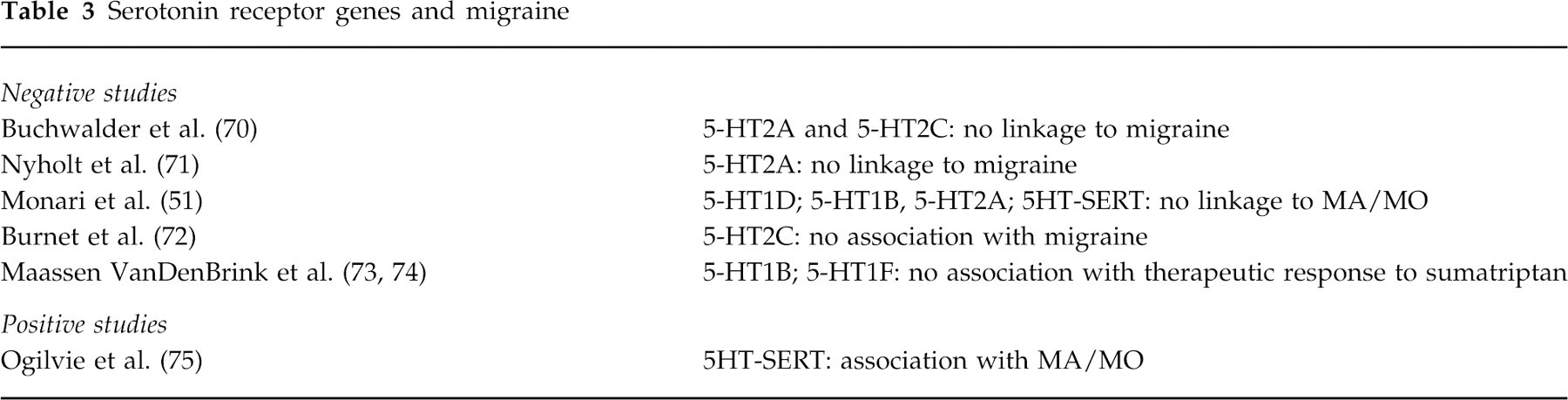
All of the examined 5-HT receptor genes are therefore unlikely to play a causative role in migraine, though of course they may become implicated at some later stage during the pathogenic cascade of the attack, say in the development of the pain. The only positive findings were reported by Ogilvie et al. (75) who studied the 5-HT transporter gene (5-HTSERT). The 5HT transporter uptakes 5-HT released in the synaptic space into the presynaptic terminal, and modulates 5-HT transmission and the therapeutic response to serotonergic drugs. The 5-HTSERT has also been implicated in the genetic mechanisms of schizophrenia, autism, alcoholism and drug abuse. Ogilvie et al. studied the distribution of the several allelic polymorphisms (characterized by variable numbers of intronic repeats) available in intron 2 of the 5-HTSERT gene, and found that 94 MA patients had an increased frequency of the STin2.12 and STin2.9 alleles, whereas 173 patients with MO had increased frequency of the STin2.12 allele alone. They concluded that susceptibility to MA and MO has a genetic component linked to the 5-HTSERT or to a locus nearby, and that MA and MO appear to be distinct genetic forms. However, we failed to find a role for this gene by linkage and sibling-pair analysis in our MA and MO families (51).
Migraine as a disorder of dopamine metabolism
Dopaminergic transmission has been implicated in the pathogenesis of migraine, with dopaminergic hypersensitivity underlying some symptoms, in particular the nausea and vomiting during the attacks (76). Antidopaminergic medications acting at the dopamine D2 receptor (DRD2) are indeed effective in the acute treatment of migraine. Several dopamine receptors are known (DRD 1–5) and different polymorphisms exist for DRD2. Association studies have been performed, again with some conflicting results.
Peroutka et al. (76) examined the susceptibility to migraine in 52 patients with MA, and found that migraineurs had a higher frequency of the DRD2 NcoI C allele compared to 121 controls (0. 84 vs. 0.7 1, P < 0.005); by contrast, 77 patients with MO did not show any significant variation in allele frequency. These data were taken to indicate that activation of the DRD2 receptor is implicated in MA, thus explaining the pharmacologic efficacy of antidopaminergic drugs. A corollary of this work is that MA and MO do not share common pathogenic mechanisms. Peroutka et al. (77) also found an increased incidence of MA, major depression, generalized anxiety, panic attacks and phobia in individuals with the DRD2 NcoI C/C genotype compared to the NcoI T allele (69% vs. 22% of 242 unrelated subjects, P < 0.00002), a result which could explain the well-known comorbidity of MA with major depression and anxiety.
Del Zompo et al. (78) studied 50 nuclear families with MO coming from Sardinia, a genetic isolate in Italy, by first identifying a subgroup of patients with ‘dopaminergic’ hyperactivity (because of yawning and nausea during the attacks, 23 patients out of 50), and then performing an association study by means of the transmission disequilibrium test (TDT), a powerful means in the face of geographical variability since it examines families in which the parental non-transmitted chromosomes serve as ethnically matched controls. No association was found between receptors DR3 and DR4 and MO; the association with DRD2 was likewise not significant for the entire sample. However, distribution at the DRD2 locus was found significantly different in the subgroup of ‘dopaminergic’ migraineurs (P = 0.004) with allele 1 of the DRD2 gene being in disequilibrium with the disease (P = 0.02). These results are not in contrast with Peroutka et al. (76) who reported no association between DRD2 and MO, because they apply only to a subgroup of migraineurs with MO clinically characterized by ‘dopaminergic hypersensitivity’ during the attack. They in fact explain some phenotypic features of the attack, but remain of course unhelpful as markers of migraine per se.
Any association between the D2 receptor NcoI allele with migraine was, however, denied by Dichgans et al. (79), who studied 47 patients with MA and 55 with MO and found that they had the same distribution as the Ncol C and T alleles reported for the normal white population (they did not examine controls). They objected, moreover, that the DRD2 NcoI polymorphism involves a silent His313His change (change of nucleotide but not of amino acid), the two alleles C and T resulting therefore in the same receptor molecule; and that, since C is the most frequent in the normal population, it is difficult to envisage a disease associated with the most prevalent allele. The problem therefore remains that the two DRD2 polymorphic alleles, though markers of genetic association at or around the DRD2 locus, cannot underlie or explain differences in receptorial function and consequently dopaminergic activity. Clearly more cogent data are needed to define the pathogenic role of the dopamine receptors in migraine, even as modifying genes, and to conclude that different mechanisms act indeed in MA and MO.
Migraine and prothrombotic factor
Migraine may be associated with brain ischemia whose pathogenesis remains unexplained. Conceivably, either migraine as a diathesis leads in itself to thrombosis, or this comorbidity is due to the genetic association of two traits, segregating in common. Such a possibility has been examined by several investigators following the report of Kontula et al. (80) that the Arg5O6Gln factor V mutation (so-called factor V Leiden), an important and relatively common risk factor for venous thromboembolism, was more frequent among those survivors of brain or heart stroke who also had symptoms of migraine. The ensuing studies, however, conflict with such a contention and among themselves.
Haan et al. (81) screened 20 patients with migraine stroke and found only one case heterozygote for the Leiden mutation (the frequency of such a mutation ranges from 2 to 7% in different general populations). Haan et al. (82) also excluded that the prothrombotic G to A mutation at position 20210 of the prothrombin gene is associated with migrainous infarction. Corral et al. (83) screened 106 (including 49 MA) migraineurs for an array of recognized genetic prothrombotic risk factors comprising: the factor V Leiden, the factor II20210 G to A mutation, the decanucleotidic insertion/deletion in the promoter of factor VII, and the platelet alloantigens HPA-1 and HPA-2, without finding any significant association; the factor V Leiden, though occurring with a high frequency among MA patients (6.1%), did not reach statistical significance. On the contrary, D'Amico et al. (84), in an investigation for protein C deficiency, APC resistance, the factor V Leiden mutation and protein S deficiency in 83 patients with MA, 31 with ischaemic stroke and 124 healthy controls, found significantly increased percentages for both protein S deficiency and the factor V Leiden mutation in MA (4.87% and 12% vs. 0% and 3.2% in controls, P = 0.05 and P = 0.028, respectively) and ischaemic stroke patients, and concluded that these prothrombotic genetic abnormalities increase the likelihood of cerebrovascular disease in migraine.
We performed a similar screen for the factor V Leiden in a group of 57 children and adolescents below 18 years of age with MA, compared to 219 consecutive blood donors (85). We found the factor V Leiden mutation in 3.5% of the patients and 3.7% of the controls, without any significant difference; moreover, the two migraine patients with the Leiden mutation did not differ clinically from the others. Thus there is no conclusive evidence that either MA or migraine stroke are statistically associated with the factor V Leiden mutation. No study has, however, been dedicated to the familial cosegregation of migraine and the Leiden mutation. Therefore, these studies cannot truly address the question whether the random concomitance of the Leiden mutation with migraine modifies the clinical phenotype or represents an aggravating factor for the patient, at what age and under which circumstances.
Miscellanea
Pardo et al. (86) were the first to perform association studies in migraine, finding strong associations with group specific component GC 1F-1F and esterase-D ESD 2–2 phenotypes, located to chromosomes 4 and 13, respectively.
Griffiths et al. (87) made a linkage and association study for a polymorphism in the endothelial NO synthase (NOS3) gene in 91 migraineurs (vs. 85 controls) and four migraine pedigrees, without, however, finding any significant result. NOS3 seems therefore unlikely to play a genetic role in migraine. Peroutka et al. (88) investigated whether comorbidity of migraine with arthritis and heart disease could be attributed to complement C3, a protein involved in acute inflammation. Polymorphism frequencies for C3F and C3S in 137 migraineurs were similar to the control population, thus excluding C3 as a source of migraine susceptibility. C3F positive migraineurs had, however, an increased incidence of osteoarthritis (P < 0.0008) and hypertension (P < 0.01). Paterna et al. (89) reported preliminary findings on the association of MO with the ACE-gene deletion polymorphism. Martelletti et al. (90) found a decreased frequency of the HLA Class II DR2 antigen in MA compared to MO and controls, supporting the hypothesis of a protective role of DR2 antigens in MA. It is difficult to make conclusions from these works, since all of them need either completion or verification. Finally, two out of three large multigenerational migraine pedigrees showed significant excess allele sharing to Xq markers, localizing a migraine susceptibility locus to chromosome X and possibly explaining the increased risk of migraine in first degree relatives of male probands and even the increased female prevalence (91).
Migraine in other hereditary conditions
Migraine may recur in a hereditary form as an isolated complaint (non-syndromic, idiopathic), or as part of the phenotypic spectrum of other hereditary diseases (syndromic migraine). Indeed, migraine is a recognized symptom in many other hereditary diseases. Pedigrees with mitochondrial encephalomyopathies due to mtDNA mutations, such as the 8356 np (92) and the 3243 tRNA(Leu) MELAS (93) show typical migraine both in patients displaying the other features typical of the disease and in otherwise asymptomatic carriers of the mutation, in whom therefore migraine may seem to occur in an isolated fashion.
CADASIL, which transmits as an autosomal dominant trait, represents another disease which may manifest primarily with migraine attacks. These occur in 38% of the cases, especially in the first decades (mean age of onset 26 years, MA in 87% of cases) (94), and prior to the development of subcortical strokes and dementia. CADASIL was mapped to chromosome 19 (95) and later shown to be due to mutations in the Notch 3 gene (13). Therefore CADASIL and FHM are genetically unrelated. However, CADASIL may occasionally manifest clinically as FHM (96). Notch 3 is one of a receptor gene family involved in the specification of tissue boundaries and cell fate in vertebrates and invertebrates, and does not code for an ion channel.
The frequency of migraine symptoms in mtDNA mutations, in which synthesis of mitochondrial enzymes of the respiratory chain is disrupted and in CADASIL, in which Notch 3 is mutated, challenges the concept that all migraines are neuronal channellopathies, and invokes other pathogenetic mechanisms, unless of course ion channels are shown to be secondarily disrupted in these conditions too. Migraine has been found to cosegregate also with autosomal dominant vascular retinopathy and Raynaud's phenomenon (97), in a family with HERNS (hereditary endotheliopathy with retinopathy, nephropathy and stroke) (98), with bilateral vestibulopathy (99) and with episodic vertigo and essential tremor (100). In the form of FHM, it segregates partially with a benign familial infantile epileptic syndrome (101). All of these conditions are too preliminarily known, their obligate link with migraine not definite as yet, and all remain genetically unmapped.
Comments
This review of the recent molecular genetic data in migraine is an attempt to classify the approaches taken and efforts made within the framework of various causative models, more or less justified by our current inadequate knowledge of the pathogenetic process. Hopefully, it may become outdated quite soon. At the moment, however, except for FHM, no conclusion on migraine genetics can be considered definitive, as is apparent from the long series of conflicting results enumerated above. Linkage analyses are usually negative, and association studies are either negative or conflicting. The latter though are becoming increasingly popular, on the assumption of migraine as a multifactorial disease.
It must be remarked that the results of genetic association often remain controversial, not only in migraine but also in other high prevalence diseases, likewise thought to be genetically multifactorial. Moreover, genetic association is not proof of pathogenic association. Apart from their intrinsic limitations (the need for large families or samples of patients and controls, their being most powerful especially in genetically isolated populations), linkage and association studies may also be limited by some wrong assumptions we make concerning the hereditary transmission and genetic heterogeneity of migraine. The different prevalence of the disease in the different decades of life, the different proportion of males and females affected, with a ratio itself variable across the ages, the different clinical manifestations of the disease according to age, etc., all represent significant constraints to genetic analysis.
Migraine is indeed, according to all available neurophysiological evidence, a disease with a threshold character (the threshold reflecting sex and age influences, besides environmental triggering factors), but there is no way to calculate this threshold and it is hard to take it into account in genetic methods of analysis. If validated, neurophysiological investigations, indicating a genetically determined excitability threshold in migraine (102–104) could hopefully be incorporated into genetic analysis. These methods may one day overcome some of the several limitations and permit a convenient characterization of migraine as a genetic disease.
Footnotes
Acknowledgements
I wish here to acknowledge the help of Dr P. Cortelli, L. Monari and M. Mochi, who reviewed the manuscript. Ms. A. Laffi typed the manuscript and helped with the references. The work was supported by CNR and MURST ex-60% grants.